Article Text

Abstract
Context Globally, there is increasing concern regarding antibiotic resistance but good hand hygiene practice has been promoted by the World Health Organisation (WHO) as one way to reduce the problem.
This project was undertaken in a resource poor district referral hospital in Kenya and involved all healthcare workers on a paediatric ward, with improved patient care being the main focus.
Problem Staff did not practice good hand hygiene as outlined in WHO and Kenyan Paediatric Association (KPA) guidelines and demonstrated poor knowledge on the subject. The ward did not have the resources to facilitate good practice thus patients and staff were at increased risk of communicable diseases.
Assessment of problem and analysis of its causes Initial audit comparing current practice against guidelines demonstrated poor compliance of all ward staff with hand hygiene guidelines with only one of the fourteen staff using hand sanitiser and none being “bare below elbows” or using soap and water.
Results were discussed with local staff, who helped to identify factors contributing to poor compliance. Healthcare worker knowledge and awareness of guidelines was poor and the hospital lacked a culture to promote good hand hygiene. Facilities on the ward were insufficient with only one out of seven sinks working, no soap or hand towels available and with the single hand sanitiser bottle locked away. Ward staff suggested solutions to overcome these problems including increased provision of soap and sanitiser, working sinks, posters to raise awareness and the championing of good practice through an infection control committee.
Intervention Training sessions were used to teach good hand hygiene emphasising it’s importance and visual reminders reinforced this message. Supplies of hand sanitiser were located within the hospital and made available at point of care and all sinks made functional. An infection control committee was started to ensure long-term advocacy of good hand hygiene practice and on-going supply of resources. Local staff were praised for good practices and encouraged to promote these practices to peers. Finally, staff members were educated on the importance and practice of audit so they could evaluate practice to ensure sustainable improvement.
Study design This project used prospective audit to measure baseline practice and subsequent improvements and observational study of facilities and behaviours.
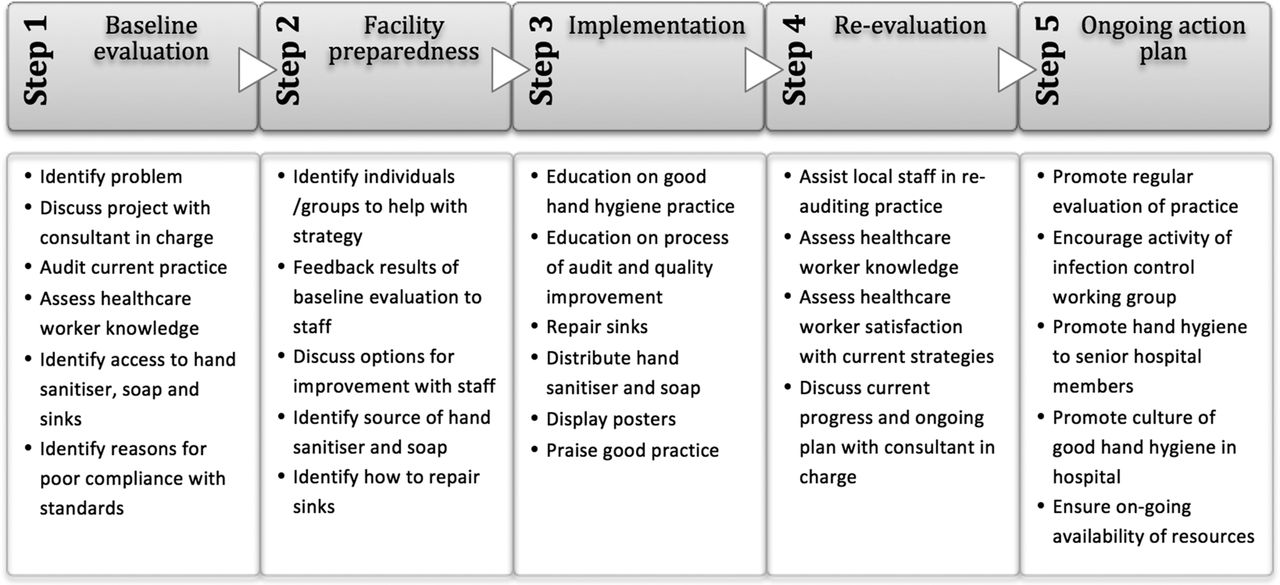
Strategy for change The WHO 5-step strategy for improving hand hygiene was adapted to suit staff and available resources. This included evaluation of current practice followed by review of resource availability and procurement. Interventions were suggested in partnership with local staff at ward and hospital levels and implemented through education and provision of resources with local staff undertaking re-evaluation and continuing to champion change. The initial timetable for change was three months with the intention of sustained change (See Figure 1).

{kind=link}
Step-by-step strategy for improving hand hygine
Measurement of improvement Re-audit was carried out monthly by local staff, initially under supervision but subsequently performed independently.
Effects of changes By the end of the first three months following implementation there was increased compliance with 100% of staff compliant with good practice standards. There was an increase in available resources with bottles of hand sanitiser available at point of care and all sinks functional. Re-evaluation by staff and compliance with guidelines was sustained.
The problems faced in this process were resistance to change due to ingrained habits of poor hand hygiene and reluctance to procure resources.
Lessons learnt It is important to have local permanent staff championing quality improvement work that can identify how best to implement change, seek appropriate resources and continue good practice. In addition, use of a structured approach to quality improvement-such as the five step process used in this project-can simplify and increase the project’s effectiveness.
Message for others Successful quality improvement interventions should be acceptable, available and appropriate to the setting to ensure sustainability; involve local or permanent staff to champion change, facilitate sustainability and create a culture of good practice.