Article Text

Abstract
Objective Key components in the assessment of a child in the emergency department (ED) are their heart and respiratory rates. In order to interpret these signs, practitioners must know what is normal for a particular age. The aim of this paper is to develop age-specific centiles for these parameters and to compare centiles with the previously published work of Fleming and Bonafide, and the Advanced Paediatric Life Support (APLS) reference ranges.
Design A retrospective cross-sectional study.
Setting The ED of the Children's Hospital at Westmead, Australia.
Patients Afebrile, Triage Category 5 (low priority) patients aged 0–15 years attending the ED.
Interventions Centiles were developed using quantile regression analysis, with cubic B-splines to model the centiles.
Main outcome measures Centile charts were compared with previous studies by concurrently plotting the estimates.
Results 668 616 records were retrieved for ED attendances from 1995 to 2011, and 111 696 heart and respiratory rates were extracted for inclusion in the analysis. Graphical comparison demonstrates that with heart rate, our 50th centile agrees with the results of Bonafide, is considerably higher than the Fleming centiles and fits well between the APLS reference ranges. With respiratory rate, our 50th centile was considerably lower than the comparison centiles in infants, becomes higher with increasing age and crosses the lower APLS range in infants and upper range in teenagers.
Conclusions Clinicians should consider adopting these centiles when assessing acutely unwell children. APLS should review their normal values for respiratory rate in infants and teenagers.
- Accident & Emergency
- General Paediatrics
- Physiology
- Resuscitation
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What is already known on this topic?
Heart and respiratory rates vary with age.
Health practitioners need to be able to interpret heart and respiratory rates in acutely unwell children and determine whether these are normal or abnormal, and if abnormal, how abnormal.
Different centiles and normal ranges are described in the literature, sometimes with conflicting results.
What this study adds?
There is still some controversy over defining the normal heart and respiratory rates in infants and children, and hence, what is statistically abnormal.
Clinicians should consider adopting these centiles when assessing acutely unwell children.
Introduction
The key components in the clinical assessment of a potentially unwell child in the emergency department (ED) are their heart and respiratory rates. All EDs have triage systems, and an integral component of the triage of a potentially sick child is the measurement and interpretation of these physiological parameters.1 An abnormal heart or respiratory rate can alert the triage staff to a potentially serious problem that may not be immediately obvious, such as a child with tachypnoea resulting from respiratory compensation for metabolic acidosis in sepsis or diabetic ketoacidosis.
Several paediatric triage systems exist and have variable sensitivity and specificity for detecting serious illness.2 A recent review of the Australasian Triage Scale (ATS) suggested that the system is valid for the most acute categories, but is less reliable for lower categories,3 and also there have been recent attempts made to improve the Manchester Triage System for children,4 the Canadian Triage and Acuity Scale paediatric guidelines (PaedCTAS).5
In order to interpret the heart and respiratory rates, practitioners must know what is regarded as normal for a particular age, as physiological parameters vary with age in children. Multiple, conflicting reference ranges for heart rates and respiratory rates have been published. These are often consensus-based and do not explain from where they were derived.6–8 It is imperative that reference ranges are accurate, else practitioners may make incorrect assessments of whether these signs are normal or abnormal. Deteriorating trends in these assessments form the basis of paediatric early warning systems, where changes in physiology can provide an early warning of a clinical deterioration. However, the literature suggests these systems may not apply to undifferentiated patients in the ED.9 ,10
In a recent paper, Fleming and colleagues presented new age-specific centiles developed for heart and respiratory rates by systematically reviewing all studies of these vital signs in healthy children.11 They then used these centiles to define new evidence-based reference ranges. Bonafide and colleagues have also developed centile charts for these parameters, but these are based on paediatric inpatients.12
The aim of this study is to develop age-specific centiles for heart and respiratory rates by reviewing patients presenting to a paediatric ED, and comparing these centiles with the previously published work of Fleming and Bonafide and the Advanced Paediatric Life Support (APLS) reference ranges.
Methods
This is a retrospective cross-sectional study of infants and children presenting to the ED of the Children's Hospital at Westmead (CHW), Sydney, Australia from November 1995 to April 2011. CHW is a tertiary referral paediatric hospital that also provides secondary care to the local community. The ED currently has 50 000 attendances per annum with a 25% admission rate. Ethical approval was obtained from the Sydney Children's Hospitals Network Human Research Ethics Committee.
Data selection
All presentations between the study dates were retrieved from the ED electronic medical record (Health E-Care, MCare Systems, Sydney). Data were then restricted to infants and children aged 0–15 years, who were assigned a Triage Category 5. Australian EDs use a 5-point triage system with 1 being the highest and 5 the lowest priority. Category 5 patients should be seen within 120 min of arrival and should have no respiratory or haemodynamic compromise, be alert, have no or minimal pain, and no risk factors for serious illness or injury.13
We removed duplicate records (data from the same presentation defined as the same medical record number, date of birth and date of presentation) to ensure only one set of observations per patient per visit were included, and restricted analyses to children with a temperature at triage of <38°C. Analyses were also limited to children who had both pulse and respiratory rates recorded. We also excluded a small number of observations that were clear errors. We excluded any observations for which the respiratory rate was ≤5 or ≥80 breaths per minute, and observations for which the pulse was ≤30 bpm, as these were clinically implausible for stable patients.
Data analysis
Data were obtained in Excel and edited in SPSS (V.19·0. Armonk, New York, USA: IBM) before being analysed using the freeware statistical program R V.2·5·2.14
We developed centile charts using quantile regression analyses, which are commonly used in creating growth charts. Quantile regression is a preferred method of providing median values as a measure of central tendency, and to obtain quantile values. This method is more robust against outliers than linear least squares regression, which provides estimates of mean values that may be biased by outliers. In the quantile regressions, we modelled age at triage in years as a predictor of pulse and respiratory rates. We also calculated 95% CIs about the quantiles.
The quantile regression parameters gave an estimate of the change in a specified quantile of the response variable produced by a one unit change in age. To improve the fit of the models and smooth the curves, cubic B-splines were used to model the centiles (1st, 5th, 10th, 25th, 50th, 75th, 90th, 95th and 99th).15 For respiratory rate, we used fixed knots at 1, 2, 4, 6, 8, 10, 12 and 14 years of age. For pulse, we used knots at 1 month and 6 months, and at 1, 2, 4, 6, 8, 10, 12 and 14 years in order to allow for greater flexibility in the centiles for children ≤1 year of age in the models. This also allowed for a possible increase in pulse in the first month of life, before a decrease, which has been observed elsewhere.11
We compared our centile charts with those of Fleming, Bonafide, and the APLS charts by plotting the estimates concurrently. Fleming supplied us with their centile data that enabled us to compare results from their meta-analyses with our centile results. Information for Bonafide and APLS was obtained from published documents.6 ,12 Graphics were produced in the programme R.14
Proposed heart and respiratory rates cut-offs were then derived using 1st, 5th, 10th, 25th, 50th, 75th, 90th, 95th and 99th centiles to maintain consistency with previously published papers.11 ,12
To estimate whether there was terminal digit preference in the recording of heart and respiratory rates, we estimated the proportion of pulse and respiratory rate readings ending in each digit from 0 to 9.
Results
Participants
Records numbering 668 616 were retrieved for all ED presentations in the defined period. After restricting to age 0–15 years and Triage Category 5, 220 193 records remained. A total of 54 071 duplicates, 24 423 records with incomplete data were also removed, leaving 141 699 records. Restriction to afebrile children with temperature <38°C left 111 784 records. Eighty-eight implausible records were removed leaving a total of 111 696 unique individual respiratory and heart rates for use in the study.
Demographics
The number of patient records in each age bracket is described in table 1.
Demographics and derived centiles for heart and respiratory rates
Main results
Figures 1 and 2 demonstrate the 1st, 50th and 99th centiles for heart and respiratory rates, with a graphical representation of the 95% CIs for centiles derived by us. The same centiles from the Fleming and Bonafide papers have been charted for graphical comparison. Data for all centiles are described in table 1 and compared with the Fleming and Bonafide centiles in online supplementary tables S1 and S2.

Centile charts for heart rate in infants and children, with visual comparison against the centiles derived by Fleming and Bonafide.

Centile charts for respiratory rate in infants and children, with visual comparison against the centiles derived by Fleming and Bonafide.
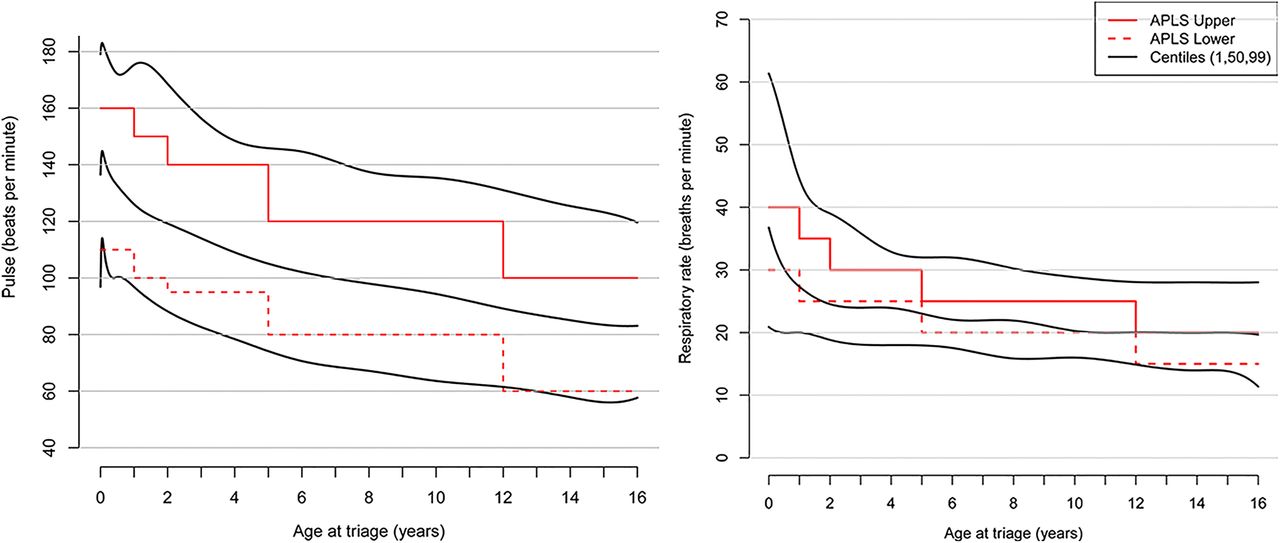
Comparison with APLS reference ranges
Figure 3 illustrates the results derived from plotting 1st, 50th and 99th centiles against the APLS reference ranges for heart and respiratory rates.
{kind=link}
{kind=link}
{kind=link}
Centile charts for heart and respiratory rates in infants and children, with visual comparison against the Advanced Paediatric Life Support (APLS) reference values.
Terminal digit preference
The proportion of readings that ended in a 0 was about 30% for both pulse and respiratory rates in contrast to the 10% that would be expected if there was no terminal digit preference. We also found that odd final digits were under-represented in the dataset; for pulse and respiratory rate, 76% and 93% of terminal digits were even numbers, respectively.
Discussion
We have analysed the heart and respiratory rates of 111 696 children presenting to a tertiary paediatric ED, categorised as Triage Category 5, and created centiles based on this data. Compared with other datasets that have been created from sporting or school environments, we feel this data are particularly valuable, as clinicians need to be able to assess infants and children in this environment and determine whether the child's heart rate or respiratory rate is normal, abnormal, or how abnormal.
When compared with the recent work of Fleming, our data are interesting. With respiratory rate, our data are graphically and clinically different. In infants, our 50th centile comes close to Fleming's 1st. Fleming only had respiratory rate data for 3881 children, and it is unclear how many were in each age bracket. Fleming also comments that the scatter plot for infant respiratory data is quite wide. Our data suggest that in children less than 3 years old, the respiratory rates are lower than those produced by Fleming, but as the child's age increases to over 3 years, our centiles are higher and become more pronounced as age increases. On comparing our heart rate centile data with Fleming's, in infants and children over 12 months of age, our centiles are also higher. One possible explanation for the higher respiratory and heart rates in older children could be anxiety associated with a visit to an ED; however, this does not explain the lower rates in children less than 3 years old.
To our knowledge, no literature exists on the change in physiology of well children attending an ED. We know that fever elevates both heart and respiratory rates,16 ,17 which is why we excluded patients with fever from the study. We also know that sleeping children have lower heart and respiratory rates,18 ,19 which is unlikely to influence our study results, as most children are awake at the time of triage as they are being examined by the nurse. Awake versus asleep observations may be important when considering activation criteria for rapid response systems, as asleep children may trigger an abnormally low heart rate or respiratory rate.
Comparing the derived centiles with those of Bonafide shows a good agreement for 50th centile for heart rate, with wider 1st and 99th centiles, possibly due to the sicker hospitalised patients in the Bonafide dataset. The 50th centiles for respiratory rate are different, but less extreme than the Fleming's centiles, following the same pattern. The 99th centiles show extreme variance across all age groups, probably related to the number of inpatients with diseases causing tachypnoea in the Bonafide dataset. The similarity in the 50th centiles between our data and Bonafide's suggests that these derived 50th centiles are quite robust and valid for a hospital setting. It is difficult to explain the differences found between Fleming's community data and the hospital-derived data, and further studies are required to investigate this, possibly including a further meta-analysis.
APLS is a respected resource for the acute care of children. It is important that the normal values they advocate are true and accurate. Graphical comparison suggests a good fit for heart rate across all age groups with the 1st and 99th representing extremes, and the 50th centile through the centre. By contrast, the respiratory rate plot reveals the APLS minimum range to be above the 50th centile up to around 5 years. This could mean that based on our data, children with normal respiratory rates could be classified as abnormally low based on the APLS guidelines.
We have used a retrospective dataset with no standard definition of how the variables should be measured. We feel that this gives strength to the study as this is real-world data, recorded as it would be in the medical record to be interpreted as it is recorded. However, we have shown with our results that it is likely that there was some rounding, or terminal digit preference, which is consistent with previously published studies.12 ,20 There are some practices that may explain this, for example, taking a reading over 10 or 15 s and multiplying the measurement to provide a rate per minute. Staff may also preferentially record to the nearest multiple of 10 or to a round number in a situation where a few units difference in readings does not influence clinical practice. We do not believe that such rounding practices would lead to consistent under-recording or over-recording.
Nurses are taught to measure heart rate and respiratory rate in a standard way, but this may not occur on every occasion. We have also used patients defined as Triage Category 5. It is possible that some patients could have been mis-triaged, and had an illness or injury significant enough to alter their baseline physiology, although with the number of patients included in this study, this is unlikely to have influenced the results.
All three studies have defined the extreme centiles, attempting to statistically define what is abnormal. This is really clinically irrelevant. What clinicians need to know is what is clinically abnormal. A patient may suffer a significant deterioration when they reach the 75th centile for heart rate, rather than the statistically significant 90th or 99th—we don't know. Clinical early warning scores are often derived from these statistical values and further work is required to determine the clinical variation from normal for age in children, which predicts a likelihood of deterioration.
There are now three major datasets on normal values in children: this study on well children attending the ED; Bonafide's on inpatients, and Fleming's meta-analysis and it is unclear which centiles clinicians should use for individual patients or populations. A further meta-analysis, or even a prospective study, with predefined subgroup analysis for these defined populations may be helpful. In the meantime, clinicians should be aware that different centiles do exist and normal ranges may have to be adapted for different settings.
Conclusions
Clinicians need to be aware that there is still some controversy over what represents a normal respiratory or heart rate in infants and children of various ages. The centiles derived from this study differ from those of the recent meta-analysis of Fleming, but have similar 50th centiles as in the work of Bonafide. Clinicians should consider adopting these centiles when assessing acutely unwell children. Additionally, although we have defined the extreme centiles, further work is required to determine at what centile the abnormality becomes clinically significant. Furthermore, APLS should review their current reference ranges for respiratory rates, particularly in infants and teenagers.
Acknowledgments
The authors would like to thank Dr Susannah Fleming, Department of Primary Care Health Sciences, Oxford, UK, for providing her original data to enable us to reconstruct her centiles and undertake the visual comparisons.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table 1
- Data supplement 2 - Online table 2
Footnotes
Correction notice This paper has been amended since it was published Online First. There was a typographical error in the Results section in the abstract. The Results section date has been corrected to “1995 to 2011” rather than 2001.
Contributors FO originated the paper, designed the methodology, participated in the analysis and wrote the paper. He is the guarantor of the paper. AH designed and implemented the statistical analysis of the data and contributed to writing the paper. JP designed the methodology, contributed to the statistical analysis of the paper and contributed to writing the paper. FL designed the methodology and wrote the paper.
Competing interests None.
Ethics approval Sydney Children's Hospitals Network review board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data have been published.