Article Text

Abstract
Objective Limited data from pharmacokinetic studies in underweight and severely malnourished children have indicated an impaired activity of their hepatic enzymes. We used the caffeine breath test to assess the metabolising activity of cytochrome P450 1A2 (CYP1A2) enzyme in underweight children.
Methods Underweight children from the paediatric outpatient clinic, Lagos State University Teaching Hospital, Ikeja in Nigeria, were studied. After an overnight fast, 15 underweight children took 3 mg/kg labelled caffeine orally. Breath samples were collected in duplicate at −20, −10 and −1 min and at 15 min intervals for 2 h. The mean cumulative per cent dose recovered (CPDR) of labelled caffeine in the expired carbon dioxide was determined over the study period. This was repeated after 2–6 weeks of nutritional rehabilitation.
Results The mean areas under the enrichment-time curve before and after nutritional rehabilitation were 0.539±0.320 and 0.620±0.322 atom per cent excess minute, respectively. The difference between the two values was not statistically significant (p=0.528). The mean CPDR in the exhaled carbon dioxide of the underweight children over a period of 2 h was 7.56±4.01% and 7.95±3.68% before and after nutritional rehabilitation, respectively, and there was no significant difference in the mean values (p=0.603).
Conclusions The metabolism of caffeine was not significantly affected in underweight children compared with after 2–6 weeks of nutritional rehabilitation. This suggests that hepatic CYP1A2-metabolising activity was not significantly impaired in underweight children.
- Pharmacology
- Therapeutics
- Tropical Paediatrics
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What is already known on this topic?
Drug metabolism may be impaired in malnourished children including those who were underweight.
Breath samples are stable and require no special preservation before analysis.
The caffeine breath test can be used to study CYP1A2 activity.
What this study adds?
Metabolism of caffeine in underweight children was not significantly impaired.
Hepatic CYP1A2 was not significantly impaired in underweight children.
The caffeine breath test is a feasible method for studying drug metabolism in children in low resource settings.
Introduction
Globally, an estimated 15% (99 million) of children aged <5 years were underweight in 2012.1The latest WHO nutrition survey, expressed in weight-for-age z-score (WAZ), in South-East Asia has reported moderate underweight (WAZ <−2 to −3) among 29% of children aged <5 years and severe underweight (WAZ <−3) in 12% of the same population of children.2 The most common reason for being underweight is malnutrition due to lack of adequate food calories and nutrients.3
The risk of death from the four major childhood infectious diseases (pneumonia, diarrhoea, measles and malaria) is significantly higher for underweight children.4 The risk for multiple infections is higher in underweight than in well-nourished children. Drug therapy, especially the use of anti-infective agents, is therefore important in this group.
The most widely used method of classifying malnutrition is the Wellcome Trust Working Party classification based on physical signs and anthropometric parameters of the patient.5 The percentage of body weight deficit in the presence or absence of oedema serves as the criterion for classification. It recognises an underweight child as having 60%–80% of the expected weight in the absence of pedal oedema.
Drug metabolism in underweight children has been poorly studied6 and its clinical relevance with regards to drug dosing in this group of children has not been investigated. Limited data from pharmacokinetic studies in this group have indicated a decrease in the total clearance of antipyrine7 and quinine,8 as well as increased half-life of paracetamol.9 Other pharmacokinetic studies comparing severe malnutrition (marasmus, marasmic–kwashiorkor and kwashiorkor) with underweight children showed that drug disposition is impaired in severely malnourished children.6 These findings would suggest a need for drug dose modification in underweight and severely malnourished children.
The caffeine breath test (CBT) has been used to study both drug interactions and effect of disease on drug metabolism in children.10 ,11 The test involves oral administration of a non-radioactive stable isotope (13C on the 3-methyl group of caffeine). The labelled caffeine undergoes 3-N-demethylation which is a cytochrome P450 (CYP1A2)-dependent reaction. After the 3-N-demethylation, the labelled methyl group enters the one carbon pool and converts to formaldehyde, formate and bicarbonate.12 ,13 The bicarbonate is finally exhaled as carbon dioxide. The cumulative per cent labelled-caffeine dose exhaled as carbon dioxide over a 2-h period is the gold standard for measuring CYP1A2 activity.14–16
In a recent study, we have used the CBT to demonstrate a significant decrease in the metabolising activity of CYP1A2 in severely malnourished children.17 In order to gain more insight into the effect of underweight malnutrition on hepatic metabolism of medicines, we used the CBT to assess the metabolising activity of CYP1A2 in a group of underweight children, before and after nutritional rehabilitation.
Methods
Fifteen underweight children were recruited from the paediatric outpatient department of Lagos State University Teaching Hospital, Ikeja. A sample size of 12 participants was considered appropriate for this study based on 90% power calculation and assuming a 2% difference in the mean±SD score of the 2 h cumulative per cent of 13C from the baseline to 2–6 weeks of restudy after nutritional rehabilitation, at a 5% level of significance, using previous CBT studies as a reference.10 ,11 ,18 However, provision for dropout and withdrawal necessitated the use of a sample size of 15 participants. Inclusion criteria included participants in a stable clinical state, age ≥3 years, informed consent from the parent and assent from a participant aged ≥6 years. Exclusion criteria included participants with HIV or tuberculosis infection, on regular medications, and having hearing impairment, cerebral palsy or elevated blood pressure. Other exclusion criteria were persistent abnormal renal or liver function tests, persistent signs and symptoms of primary cardiovascular, respiratory or gastrointestinal disease.
Underweight malnutrition was diagnosed as a patient with 60%–80% of the expected weight without pedal oedema.5 Participants were first studied when underweight and after nutritional rehabilitation to attain over 80% of the expected weight for age.
Body weight and height of each subject were measured as described in our study in severely malnourished children.17 All the participants avoided caffeinated products for 20 h and fasted overnight prior to the CBT. All the CBTs were commenced at 9:00. Casilan, calculated as one-twelfth of the recommended dietary allowance of calories,19 was ingested at 8:30 before caffeine administration because of ethical issues surrounding fasting of the underweight children. Casilan is bland powder milk, rich in protein but very low in fat and carbohydrate.19 The subjects remain seated for 10 min prior to the collection of the first breath sample. Participants were kept busy by the lead researcher throughout the whole test so as to minimise physical activity which can affect endogenous carbon dioxide production and result in dilution of the labelled carbon dioxide.10 ,11
Participants consumed 3 mg/kg labelled caffeine made into solution at 9:00. The caffeine was obtained in powder form from Cambridge Isotope Laboratories (Cambridge, Massachusetts, USA). Each sample of the caffeine was dissolved in 10 mL of clean water. Non-sugary squash was added to the mixture to mask the bitter taste of caffeine. The container was washed with 20 mL of water, which was also consumed by the participants. Breath samples were collected in pairs while the subjects expired normally at −20, −10 and −1 min prior to caffeine (predose samples) and after caffeine ingestion (postdose samples) every 15 min over 2 h. Breath samples were collected into an Exetainer bottle by asking each child to blow via a straw. The vital signs of the participants were recorded and monitored throughout the study.
Participants were restudied after adequate nutritional rehabilitation for 2–6 weeks, thus serving as their own controls. Casilan and caffeine administration, as well as breath sample collection, was according to the protocol described for severely malnourished children after undergoing nutritional rehabilitation.17 The breath samples were stored in the Exetainer bottles for 12 weeks before transport by air for analysis at the Clinical Physiology Laboratory of the Graduate Entry Medical School of the University of Nottingham, UK.
The 13C-enrichment in the breath samples was determined by continuous-flow isotope ratio mass spectrometry20 using a SerCon-Automated Breath Carbon Analyser (CF-IRMS; Europa Hydra; SerCon, Crewe, UK). The details of the analytical procedure are as documented in our previous study.17
CYP1A2-metabolising activity was determined using the cumulative 13CO2 in the expired breath samples collected over 2 h as a gold standard. The cumulative 13CO2 output was determined as an average of the 13C-enrichment for the eight breath samples exhaled over 2 h multiplied by the average carbon dioxide output (VCO2) over the study period (300 mmol/body surface area per hour).21 ,22 The result was expressed as a percentage of the caffeine dose administered.
The Ethics Committee of Lagos State University Teaching Hospital, Ikeja, approved the study. Parents gave their informed consent, and subjects who were aged ≥6 years gave their assent.
The participants were compared when underweight and after nutritional rehabilitation, using a Student's paired t test at 5% level of significance.
Results
Analysis of the demographics and anthropometric parameters of the 15 underweight children showed that their mean age was 7.6±2.9 years. Their mean weight significantly increased from 17.9±5.6 kg (before nutritional rehabilitation) to 21.4±6.8 kg (after nutritional rehabilitation; Student's paired t test, p<0.005). All the children had reached at least 80% of their expected weight before the second breath test (table 1). Their mean height significantly increased from 115.4±16.3 cm (before nutritional rehabilitation) to 116.5±16.2 cm (after nutritional rehabilitation; Student's paired t test, p<0.005). They were restudied after a mean period of 3.7 weeks following nutritional rehabilitation.
Average cumulative per cent 13C-dose in the exhaled 2-h CO2 of underweight children, before and after nutritional rehabilitation
The mean areas under the enrichment-time curve before and after nutritional rehabilitation were 0.539±0.320 and 0.620±0.322 atom per cent excess minute, respectively. The difference between the two mean values was not statistically significant (Student's paired t test, p=0.528).
The average cumulative per cent doses recovered (CPDR) in the exhaled CO2 over a period of 2 h of the underweight children are shown in table 1. The mean CPDR was 7.56±4.01% before and 7.95±3.68% after nutritional rehabilitation, and there was no significant difference in the mean values (Student's paired t test, p=0.603).
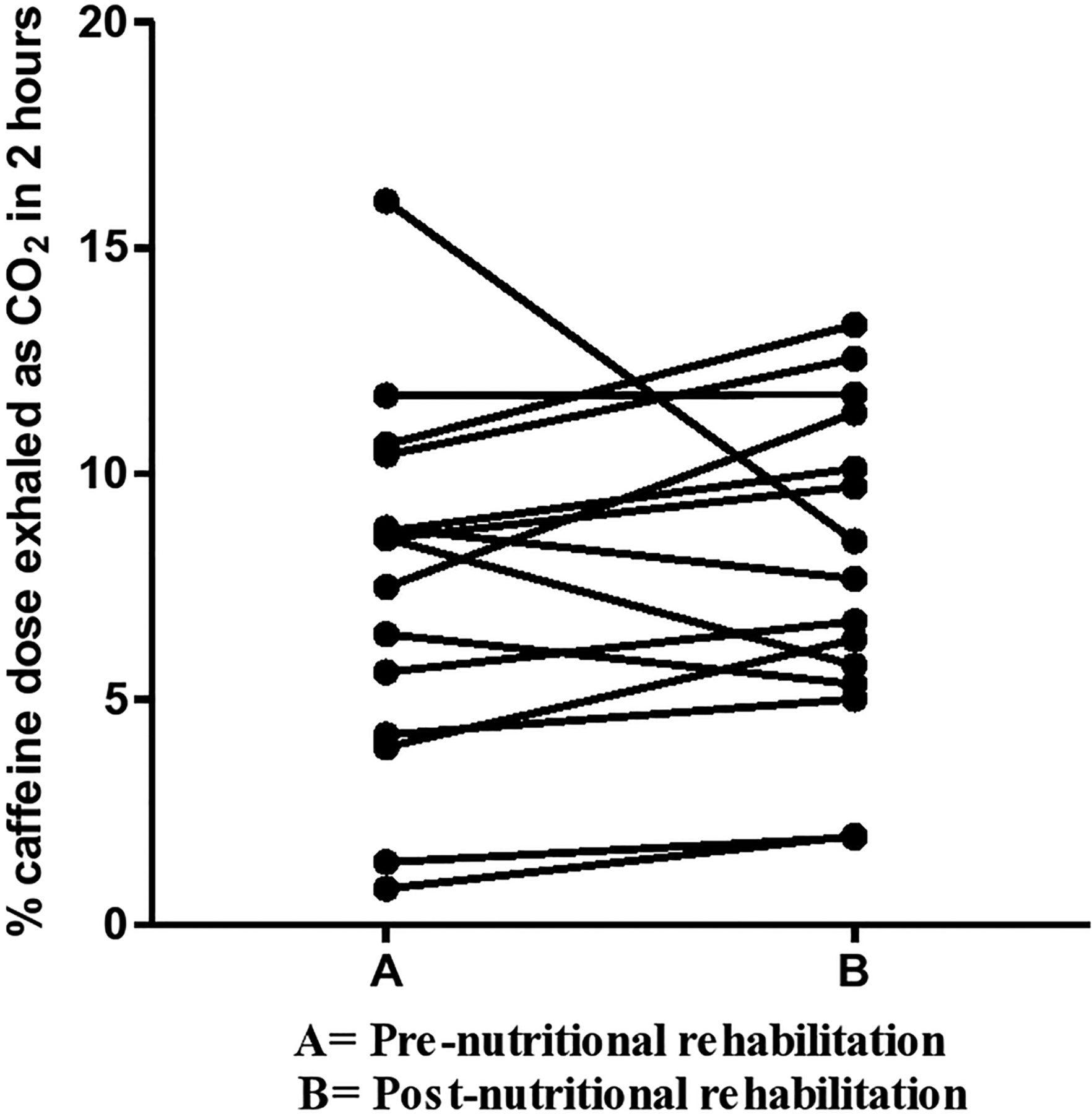
The individual cumulative per cent labelled caffeine dose exhaled as CO2 in a period of 2 h by each underweight child both before and after nutritional rehabilitation is presented in figure 1. There was greater interindividual variation seen before rather than after nutritional rehabilitation.

{kind=link}
Individual cumulative per cent 13C-dose recovery in 2 h for each underweight child, both before and after nutritional rehabilitation, expressed as a percentage of the oral caffeine dose administered.
Discussion
In the present study, underweight children were studied before and after nutritional rehabilitation. Nutritional rehabilitation for 2–6 weeks enabled the underweight children to attain the expected weight-for-height of well-nourished children before they were restudied, thus serving as normal weight controls. We have demonstrated no significant difference in labelled CO2 exhaled over 2 h. This suggests that the metabolism of labelled caffeine was not significantly affected in children when they were underweight compared with when they had attained at least 80% normal weight after nutritional rehabilitation.
A limitation of our study is that the children were studied immediately after nutritional rehabilitation. It is possible that hepatic enzyme recovery significantly lagged behind nutritional recovery. However, our findings are consistent with those of Tranvouez et al24 who determined the plasma clearance (CL) of antipyrine (a drug, ie, partially metabolised by CYP1A2) in underweight adults and showed no significant change after nutritional rehabilitation.24
Three other studies, in contrast, have shown decreased CL of different drugs in underweight patients. Specifically, antipyrine CL was decreased in underweight adults,25 while the CLs of acetylsalicylic acid and penicillin decreased in underweight children.26 ,27 Different types of CYP450 enzymes are responsible for the metabolism of caffeine and acetylsalicylic acid, while penicillin is usually eliminated without undergoing hepatic metabolism. Acetylsalicylic acid is metabolised by CYP3A4, while caffeine is predominantly metabolised by CYP1A2. Variation in the activity of the metabolising enzymes may account for the differences in the disposition of caffeine and other drugs in underweight children.
The present results of underweight children are in contrast to those of severely malnourished children.17 CYP1A2 enzyme activity was significantly impaired in severely malnourished children with marasmus, marasmic–kwashiorkor or kwashiorkor.17 It is important therefore to be aware that malnutrition is a spectrum of nutritional disorders and its effect on drug metabolism will vary with the type of malnutrition and the accompanying physiological changes. The mechanism involved in the altered CYP1A2 activity and decreased caffeine metabolism in severe malnutrition remains poorly understood. It has been postulated that impairment in drug metabolism in children with marasmus may be partly related to an adaptation to insufficient energy intake, resulting in reduced total microsomal haeme, phospholipids and flavin adenine dinucleotide levels, all of which are necessary for microsomal drug metabolism.28 Altered drug metabolism in children with marasmic–kwashiorkor has been linked to substantial changes in the quantities of microsomal membrane proteins, particularly the CYP450.29 ,30
Impairment of drug metabolism in children with kwashiorkor has been attributed to maladaptation to nutritional deprivation, which includes hepatic fatty infiltration, rough endoplasmic reticulum and mitochondria deformity and reduced peroxisomes.31
CYP1A2 is a major metabolic pathway for caffeine, theophylline, naproxen, haloperidol and the antidepressants duloxetine and fluvoxamine.32 It is also a contributory metabolic pathway for many other drugs.32 The findings from our study suggest that dose adjustment is not necessary for underweight children who are receiving caffeine, theophylline, haloperidol, naproxen, duloxetine or fluvoxamine. It is important, however, to recognise that our findings are only relevant for drugs where CYP1A2 is a major metabolic pathway. The effect of being underweight needs to be studied separately for each of the different metabolic pathways.
In conclusion, the CBT has demonstrated no significant change in the metabolism of caffeine in underweight children. This suggests that the doses of medicines that are primarily metabolised by hepatic CYP1A2 do not need to be modified in underweight children.
References
Footnotes
Contributors KAO conceived and designed the study, collected and analysed the samples, performed the data analysis and wrote the initial and final draft of the manuscript; HS and IC contributed to the conception and design of the study, reviewed the data analysis, edited and approved the final draft of the manuscript; KS contributed to the sample and data analyses and reviewed the initial draft of the manuscript.
Funding KAO was, at the time of this research, a postgraduate research student at the University of Nottingham, UK. He was jointly sponsored for the postgraduate education by the Lagos State Government and Lagos State University.
Competing interests None.
Patient consent Obtained.
Ethics approval Research and Ethics Committee of LASUTH.
Provenance and peer review Not commissioned; externally peer reviewed.