Article Text

Abstract
Background/aims Children with idiopathic short stature (ISS) constitute a heterogenous group. Recombinant IGF-I (rhIGF-I) have been licensed for the treatment of severe short stature (height <−3 standard deviation scores (SDS)) in ISS children with low IGF-I levels (IGF-I<−2 SDS). However, children with low IGF-I levels remain poorly characterised. We aim to characterise the clinical features and growth outcomes of ISS children with low IGF-I levels in a tertiary paediatric endocrinology clinic.
Methods Children with ISS were identified by a retrospective review of patients who underwent GH provocation tests during 2000-2011 using the criteria (i) pre-pubertal state (ii) age <13 years in girls, and <14 years in boys (iii) height <−2 SDS (iv) absence of organic causes of pituitary dysfunction and (v) peak Growth Hormone levels (GH) > 8 µg/L (vi) birth weight >−2 SDS.
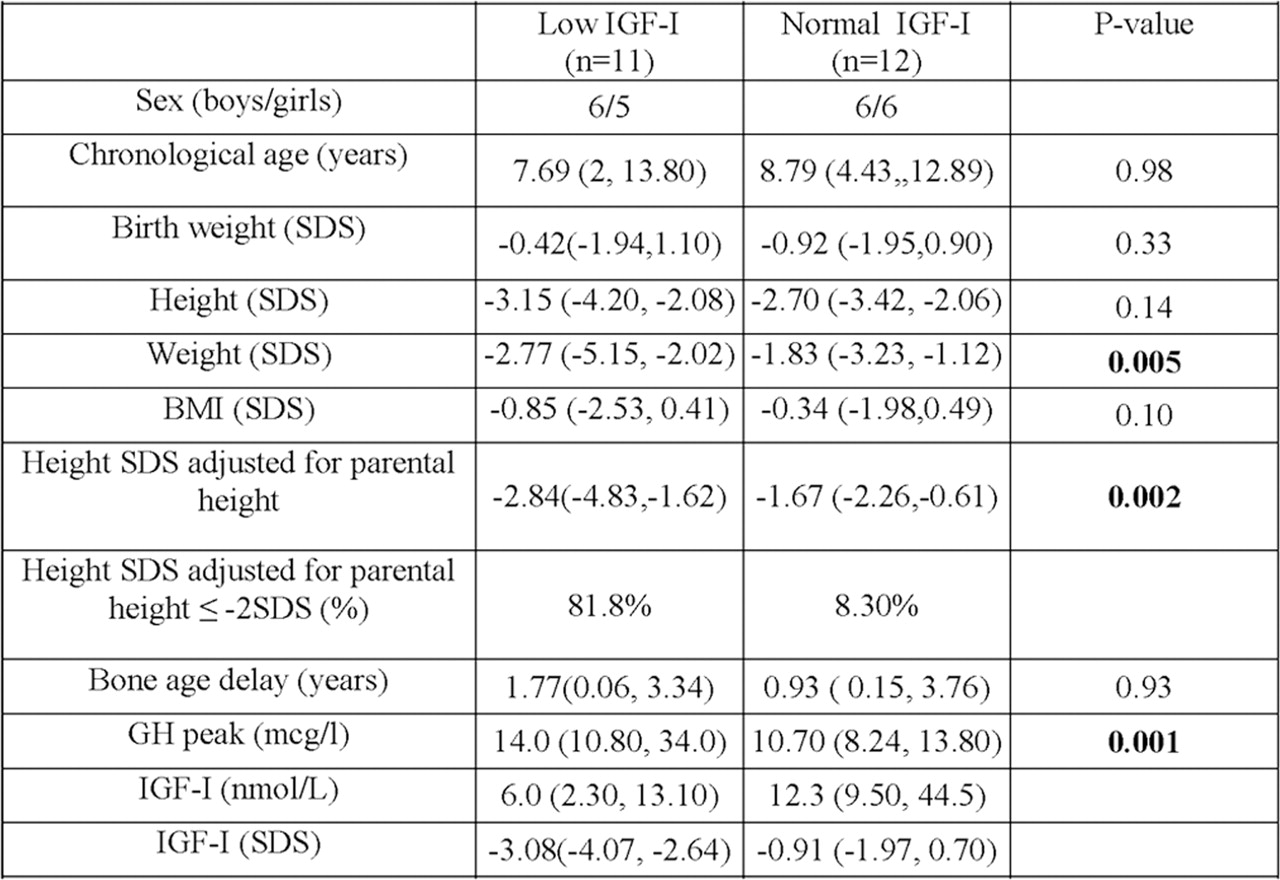
Results We identified 11 (47.8%) children with low IGF-I levels among 23 ISS children. They had a lower height SDS adjusted for parental height (p=0.002) and weight SDS (p=0.005) as compared with ISS children with normal IGF-I levels (table 1). These children also had increased peak stimulated GH levels (p=0.001). However, abnormally high levels (>24µg/L) were not observed. Of the 9 children with low IGF-I levels, who had subsequent IGF-I measurements, 5 increased their levels to >−2 SDS spontaneously (figure 1). Among the 7 of these children who were followed up to puberty, 4 improved their height to >−2 SDS without any treatments. Six of the 11 children with low IGF-I levels (54.5%), had a height of <−3 SDS and were eligible for rhIGF-I therapy by the current guidelines (table 1 and figure 1).

Subsequent IGF-Is measured during follow up in the 11 ISS children with low baseline IGF-I levels. Dashed lines indicate improvement in IGF-I, solid lines indicate persistently low IGF-I.
{kind=link}
{kind=link}
Baseline data of children with idiopathic short staure. Data presented as medians, range(min,max). P values calculated according to Mann-Whitney Test with significant values in bold.
Conclusion We found that 47.8% of ISS children had low IGF-I levels. They were shorter and weighed less than other ISS children and exhibited GH resistance. However, alterations in GH/IGF-I axis were transient in almost half of these children, leading to increases in height SDS and IGF-I SDS with time. Improvements in nutrition or onset of puberty may explain the spontaneous increases in IGF-I levels. Persistently low IGF-I levels may be used to select children for further evaluation including molecular analysis in the absence of classical features of GH resistance.