Article Text

Statistics from Altmetric.com
Introduction
Inadequate health systems are now widely recognised as major barriers to improved newborn and child survival and achieving Millennium Development Goal 4 that calls for a two-thirds reduction in under 5 mortality in low-income settings.1 A key challenge of the coming decade is thus to strengthen health systems and ‘scale-up’ delivery of safe, accessible and high quality care.2,–,4 The required interventions are often divided up into ‘essential packages’, each with their own training materials and dedicated training courses. Examples include essential neonatal care, essential obstetric care, malaria case management, case management of severe malnutrition and management of the HIV infected child. Reported examples of successful scaling-up of such packages are usually drawn from large, internationally well-funded programmes in fields such as HIV.5 In contrast, support for widespread implementation of cross-cutting interventions such as WHO/UNICEF's Integrated Management of Childhood Illnesses can be half-hearted even if the approach is formally adopted at policy level.6 7
For care of the seriously ill child, in theory concentrated in rural hospitals as a result of referral, a holistic approach, identifying and managing all needs given the available resources, is intuitively sensible rather than focusing thinking and training on only malaria, or only HIV or only severe malnutrition.8 Such thinking prompted development of WHO's Emergency Triage Assessment and Treatment (ETAT) training programme,9 designed with a similar philosophy to emergency care courses aimed at higher income settings (eg, European Paediatric Life Support, EPLS). However, work indicating outdated, poor quality of case management of serious illness10 11 revealed a need for knowledge and skills that went beyond emergency care. We therefore adapted and extended ETAT training to include aspects of neonatal care and management of serious paediatric illness covered by the WHO's Pocketbook of Hospital Care for Children,12 specific Kenyan, national guidelines13 and hospital self-assessment and improvement planning exercises to produce ETAT+ (described in detail in Irimu et al14). Although there are reports of better emergency care being introduced in low income African settings,15 16 descriptions of attempts to embed such approaches in a national health system in Africa are rare. We therefore describe our experience in this area.
Guiding our efforts have been evidence10 17 and local experience that: (1) most hospital staff did not have access to national or international guidelines; (2) training should take place within facilities and be non-residential for trainees; (3) effective teaching, particularly of skills, requires effective instructors/facilitators, who must therefore themselves be trained and quality assured, in contrast to most cascade approaches; (4) reaching preservice trainees was vital; and (5) activities must be embedded in local institutions and conducted in partnership with government. (For details of course content, design and all materials, please visit http://www.idoc-africa.org). Before we share our experiences, however, we should explain the term ‘scaling up’. Although the term has a range of meanings,18 a common thread is the idea of moving beyond efficacy or demonstrations of feasibility to routine uptake. In this usage there are clear overlaps with ideas around dissemination and knowledge transfer. We prefer the term scaling up as it perhaps captures better the deliberate attempts to deliver widely the new best practice guidelines and skills that are the subject of this discussion.
Observations on the context within which attempts at scaling up were made
Kenya's health sector development is guided by a National Health Sector Strategic Plan that articulates aims to deliver essential packages for health.19,–,21 However, there are no standard, over-arching mechanisms for knowledge translation that span development, approval, coordination and implementation of guidelines either for health workers already working in the health system or for those in preservice training. Defining guidelines or standards of care are thus the de facto responsibility of an array of government departments, divisions and programmes. In several areas, notably for HIV, malaria and reproductive or maternal health, considerable additional technical support is provided by global or bilateral partners, often operating through or with large non-governmental organisations. In practice this means that innovations to be considered for scaling up are typically identified and supported by a parent division or programme and their allied partners. Subsequently, the likelihood and scale of implementation efforts are related to the ability of such alliances to provide finance. The ‘vertical’ paradigm with funding tied, for example, to malaria or HIV, is thus readily apparent even at stages as early as identification and promotion of innovations.
As we discovered therefore, developing your innovation with government or local institutions and having their strong backing does not necessarily make for success. Instead, technical meetings of policy makers and programme planners to discuss new interventions often see over-stretched government staff considerably outnumbered by their multi-lateral, bilateral and non-governmental organisation counterparts. They, as we did, have their own agendas often linked to fixed and strictly time-limited funding. Any discussions on integration or alternative courses are often therefore overtaken by concerns for rapid dissemination and implementation. Our guidelines and linked training, while having government and institutional support, did not fall into a clear disease-specific category and moreover were aimed at rural hospitals, a relatively unfashionable level of the health system.
Guideline dissemination and extending the reach of training – a short history
This context had obvious impact on the uptake of the 2006 national paediatric guidelines (figure 1). Thus, while nationally mandated, there were initially no funds to produce guideline booklets even though they cost less than £0.50 each. An initial run of 1000 copies, produced by the research team, was retained to support training courses, but absence of a powerful programme or donor ally meant it was 12 months after their official, government launch before 10 000 copies were printed with help from WHO in Kenya. Unfortunately no funds were allocated for distribution.

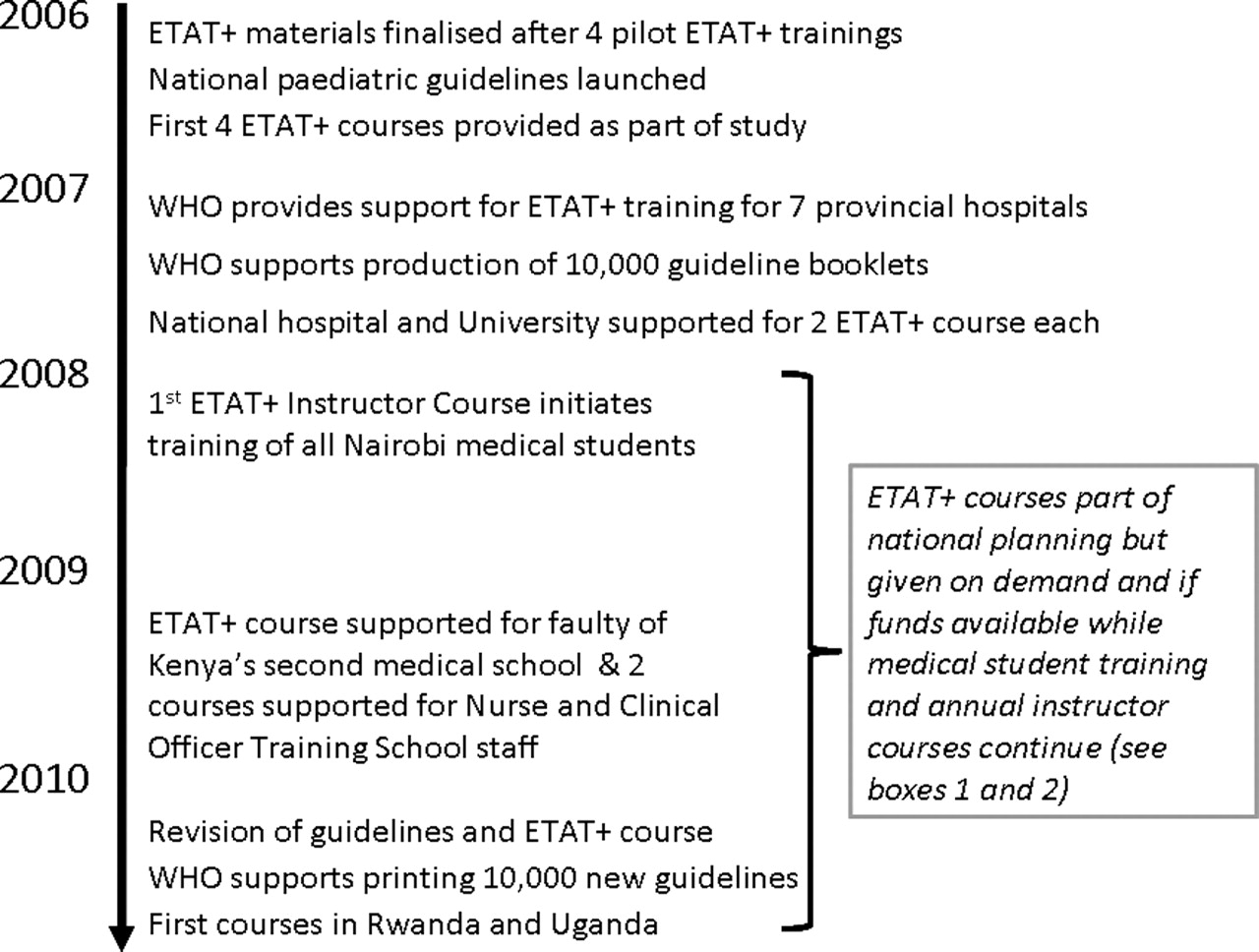
Summary timeline or history of ETAT+ development, 2006–2010.
The training linked to the guidelines (called ETAT+) was piloted in early 2006 in the national hospital, a rural hospital and a major medical training college before being delivered in four rural hospitals as part of the research programme in late 2006. It proved extremely popular and appeared to fill a relatively large gap in knowledge and skills related to management of the seriously ill newborn and child. A gap that WHO, with its training,9 had earlier partly attempted to fill with the government, although the attempt started and finished with only two ETAT courses run in 2004. With renewed enthusiasm for the 2006 ETAT+ course, the government successfully requested funds from WHO to provide one training course to all seven provincial (regional) hospitals in 2007/2008.
Positive responses to the 2007 ETAT+ training resulted in training of all major district hospitals becoming a specific aspect of the government's Annual Operating Plans in 2008, 2009 and 2010. However, despite this signal to donor partners that support was being sought and despite further requests to and through the WHO country office, no additional funds for guideline dissemination or ETAT+ training have been received to date (November 2010 at time of writing). This could indicate that the intervention is actually considered to be of low priority given the many competing demands for funding. However, the absence of support may also reflect absence of explicit decision-making mechanisms to rank priorities, our inability to align the broad-based training with a specific major vertical programme, lack of a coordinated national strategy for updating clinical practices, lack of funds for general health system strengthening, concern over the costs (a form of prioritisation) and, finally, possibly also a loss of faith in earlier attempts to scale up cross-cutting training in child health.7
Scaling up and serendipity
While attempts to garner significant financial backing and formal support met with little success, the guidelines and ETAT+ training continued steadily gaining support within government and from paediatric opinion leaders and practitioners as ad hoc, small-scale delivery approaches continued. It is the genesis of this support and what it illustrates about the reality we observed of scaling up that we now describe.
Core value
Appreciating that even seriously ill children and newborns are typically managed, even in hospital settings, by health workers with at most 10–12 weeks of paediatric training (usually only two are on newborn care), the guidelines and ETAT+ training target such providers.14 After initial engagement with local university paediatricians and the national hospital, two things quickly became apparent. First, it was realised that attempts to implement standardised clinical practice at hospital level, using available evidence, had rarely been taken seriously in the past. Secondly, it was appreciated that most providers did not actually have appropriate skills to deal with a seriously ill newborn or child and were unaware of the basic resource implications of providing such care (eg, most providers were unaware how to use oxygen correctly with a nasal catheter). Paradoxically these ‘blind spots’ perhaps arose because conditions such as pneumonia were considered so routine that they required little thought. As a consequence, a general consensus emerged that the guidelines and ETAT+ training provided an opportunity to provide standard, appropriate knowledge and skills to health providers with limited experience or prior training. (This largely explained governmental support and incorporation into government annual operating plans.) Within Nairobi's medical school (which trains >70% of all doctors and specialists nationally) this led to the incorporation of ETAT+ training into the induction period for new, trainee paediatricians and, in modified form, the integration of ETAT+ training into undergraduate medical training in paediatrics. Such efforts have resulted in introductory training of almost 1000 medical students between 2008 and 2010 (see box 1).
Progress in disseminating guidelines and training

Plot of total number of health workers (y axis) receiving full ETAT+ training since 2006 (black bars) and number of health workers trained each year (grey bars) over the period 2006 to November 2010 (x axis). An additional 900 medical students have received an adapted 3 days of training since 2008.


Schematic of approach to developing an instructor pool within the University of Nairobi where paediatric trainees deliver an adapted ETAT+ course to medical undergraduates.

The intricate web of demand, capacity and ownership
Although demand can be frivolous, influenced by clever marketing or raised by perverse incentives, such as the habit of paying allowances to attend training (course participants for ETAT+ are generally trained within their own institution and no allowances are paid), it is also an index of value. While there was no distribution strategy for the national guidelines, hospitals, health workers and students mobilised to ensure ad hoc distribution of 10 000 copies within 18 months. Much unmet demand remained, partly alleviated by wide-scale reliance on photocopies and, recently, by internet publication. Demand for in-service ETAT+ training also continued to grow. Within the national hospital, funding was provided to train clinical officers and nurses working in paediatric areas. Rural hospitals have made written requests for training to senior government staff and some have managed to provide courses by advocating for funds from local donor partners (see box 2). Most recently, self-financing courses for the private sector and for the national paediatric association and co-funded courses for lecturers from medical training colleges and the faith-based sector have been run (see box 2). While such activities represent a form of demand-led scaling up, and have been made possible by small but critically important core grants (since 2007, the ETAT+ programme has benefitted from small grants from the David Baum International Foundation and the Hillman Medical Education Fund that support some core functions, including instructor training, and post-graduate and undergraduate training in the University of Nairobi), limited funding has meant response to the actual level of demand is inadequate and making more strategic, medium term plans has not been possible.
Expanding access to training in response to demand
With competent instructors in government hospitals and the private sector as well as inside the university system, it has been possible to both promote conduct of training courses and work with partners who can provide funding for such courses. Thus, since 2009 four larger, government district hospitals have worked with a donor agency in their region to run training courses for health workers from smaller hospitals and health centres in their locality with instructors largely drawn from within the government sector. The major private sector children's hospital in Nairobi has also begun offering the training to its own staff, running four courses in 2010, and, in response to requests from staff at a refugee camp in Northern Kenyan, a course has been supported by the International Red Cross. In late 2010 with support from funds to two small regional projects, two courses were run, one in Uganda and one in Rwanda, to introduce the course concept in these countries.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
To respond to demand for training clearly requires instructor capacity as well as funding. Participants' acquisition of knowledge and especially skills are likely to depend on the quality of the trainer. Instructors need (at least) to be highly proficient and have appropriate communication skills and a desire to train. All too often these somewhat obvious statements are ignored in low-income settings where the number of trainees and not the knowledge or skills gained are the metrics of scaling-up. Thus a common partner-funded model of rapid scaling up involves start-up training, often led by international ‘;master trainers’. This is expected to be a catalyst for system change after (miraculously) becoming self-sustaining or, un-shepherded, permeating the entire clinical culture.
However, producing good trainers means establishing mechanisms to develop them. If investments of this sort are to be reasonably efficient, they demand a medium term agenda and the ability to retain, coordinate and reutilise trainers. Prompted as much by the reality we encountered as by a prior philosophy, our ‘tortoise’ approach has resulted in three annual instructor courses to date. These 3-day courses, run to standards similar to the UK Resuscitation Council's Generic Instructor Course, have yielded 57 current instructor graduates. A good fraction are within the University of Nairobi where we have worked to a low-cost plan to develop a sustainable instructor pool who can run courses for medical students (see box 1). Paediatricians or nurses in larger, rural government hospitals provide a further pool of instructors utilised for providing training within the public sector (see box 2). The modest number of instructors provides the opportunity for individuals to gain considerable training experience and hone skills. Although all our evidence is anecdotal, this seems to result in the continued provision of high quality training, appreciative trainees and expanding demand. A strong cadre of trainers encouraged to explore and understand the evidence and rationale for what they are teaching also seems to have expanded the credibility and sense of ownership of the guidelines and the training. More confident instructors have also initiated in-house, focused training in some rural hospitals, for example, several run in-house newborn resuscitation programmes. This expression of confidence is probably helped by clear endorsement from government, strong links to a local university, and increasing engagement with the Kenya Paediatric Association and the recently constituted National Resuscitation Council of Kenya. With greater ownership comes, however, further demand and increasing pressure from a variety of partners for sustained relevance and quality. Such pressure led to a major collaborative revision of both guidelines and training materials in 2010, including probably the first major effort to use the Grading of Recommendations Assessment Development and Evaluation (GRADE) approach22 at country level in Africa (see http://www.idoc-africa.org). (The GRADE approach is a structured approach to evidence synthesis, summary appraisal of quality and development of clinical guideline or policy recommendations.)
So what have we learned?
We increasingly hear the term scaling-up linked to delivery of appropriate, evidence-based health worker practices to achieve high coverage with accessible, high quality services. The literature discusses vertical, horizontal or, more recently, diagonal approaches to scaling up.18 These models, while different, all tend to convey the sense that we can set a trajectory, act and define an endpoint to the process. Our experience with introducing basic, national guidelines aimed at improving care for the seriously ill newborn or child at district hospital level indicates that unseen, unpredictable currents and forces result in a far from linear course. Any progress we have made has been relatively slow, not often as planned, and with effects that are hard to measure, although recent data are encouraging.23 This experience may best represent scaling up efforts for interventions without major financial backing. Indeed, such backing is hard to obtain despite government engagement that extends to requests for resources through health system strengthening mechanisms as part of global fund applications.
Those with technical expertise and the intention to help (including ourselves) are also perhaps part of the problem with concerted efforts at scaling up. During the last 4 years, many groups from different countries have offered a variety of emergency care courses even in the fields of paediatric and newborn care. The same is true in other clinical areas, including adult and obstetric emergency care. Some groups provide as little as one course, others multiple courses over a period of months. Such fragmented efforts are unlikely to be in the best interest of the country as a whole and are likely cost-inefficient. It is also likely that until available resources and capacity from multiple partners, small and large, are linked to long term strategies to build mechanisms at national and even subnational levels for prioritising, integrating, coordinating, disseminating, implementing and supervising emergency care, many efforts to improve care will have results that are unpredictable at best and minimal and short term at worst. In part, such fragmentation reflects gaps in the capacity to manage and co-ordinate care, a human resource challenge less often highlighted than inadequate health worker numbers.24 However, packaging, disseminating, explaining and supervising the introduction of new clinical guidelines and training demands a particular skill set. It seems willingness or ability to invest, in a collaborative fashion, over the long term in developing locally authoritative institutions to take on such roles is limited.
Conclusion
Modernising care of the seriously ill child or newborn in low-income settings should be thought of as a continuous process as practices must be sustained and inevitably evolve. We often do not appreciate this reality in our enthusiasm to help. The literature on scaling up also confuses people, suggesting that efforts to scale-up can be time-limited and follow a clear, project management trajectory. This may be true of well-funded vertical programmes, but our experience argues that support for initial efforts to change practices and subsequent, incremental expansion and revision supported by long term partnerships are likely to be needed in many cases. Such approaches would usefully be embedded in local health systems with engagement of government, teaching institutions and professional associations. In the race to improve health systems through scaling-up, when most are concerned with rapid impact, we suggest the tortoise, a more measured and inclusive strategy, also deserves some attention.
Acknowledgments
The authors are grateful to their staff and colleagues whose insights helped us develop this manuscript. They are also grateful to Professor Elizabeth Molyneux, Sheila Simpson, Roy Ellington and Andrew Coleman who have helped initiate and/or support the ETAT+ training programme. There would be no experiences to report if those trained as instructors had not supported the ongoing provision of courses and to all these people and those in other arms of the Ministries of Health in Kenya we are grateful. The authors would like to thank the David Baum International Foundation and the Hillman Medical Education Fund that have contributed within the period 2005–2010 to activities including guideline development meetings, ETAT+ instructor training and quality assurance, ETAT+ training for medical students and ETAT+ training for medical training college lecturers. They also thank WHO-Kenya for funding the printing of guideline booklets. This work is published with the permission of the Director of KEMRI.
References
Footnotes
-
Funding Funds from a Wellcome Trust Senior Fellowship support ME (#076827) and GI. AW and RN are employed by the Government of Kenya.
-
Competing interests The authors ME, BB and GI have all had an active role in developing or delivering the guidelines and ETAT+ training.
-
Provenance and peer review Commissioned; externally peer reviewed.