Article Text

Statistics from Altmetric.com
Kenya, in common with many developing countries, has committed itself to Millennium Development Goal (MDG)-4, which calls for a two-third reduction in 1990 mortality levels in under 5-year-old children by 2015.1 Improving the management of common severe childhood illnesses is one of many strategies likely to be needed to achieve this goal since hospital mortality rates as high as 15% are reported.2 3 Two further points also suggest the potential value of improved basic care to improve outcomes. First, the majority of deaths are attributable to a handful of illnesses and second, assessments demonstrate that the quality of care provided to children in low-income countries is often poor and has considerable scope for improvement.3 4
Clinical practice guidelines (CPGs) are intended to assist the health provider in evidence-based decision making and promote the provision of optimal care. Previous studies have shown that adherence to such evidence-based guidelines is associated with improved health outcomes.5–7 For some conditions such as pneumonia8 and diarrhoea,9 10 the World Health Organization has made CPGs available for many years. In 2000 evidence and expert opinion were used to provide comprehensive advice on the care of sick children in hospital with common conditions.11 However, few hospitals or health workers in Kenya have access to either the WHO recommendations or modern local practice guidelines3 and it is known that a wide range of factors affect the actual ability to improve care and outcomes.12–15
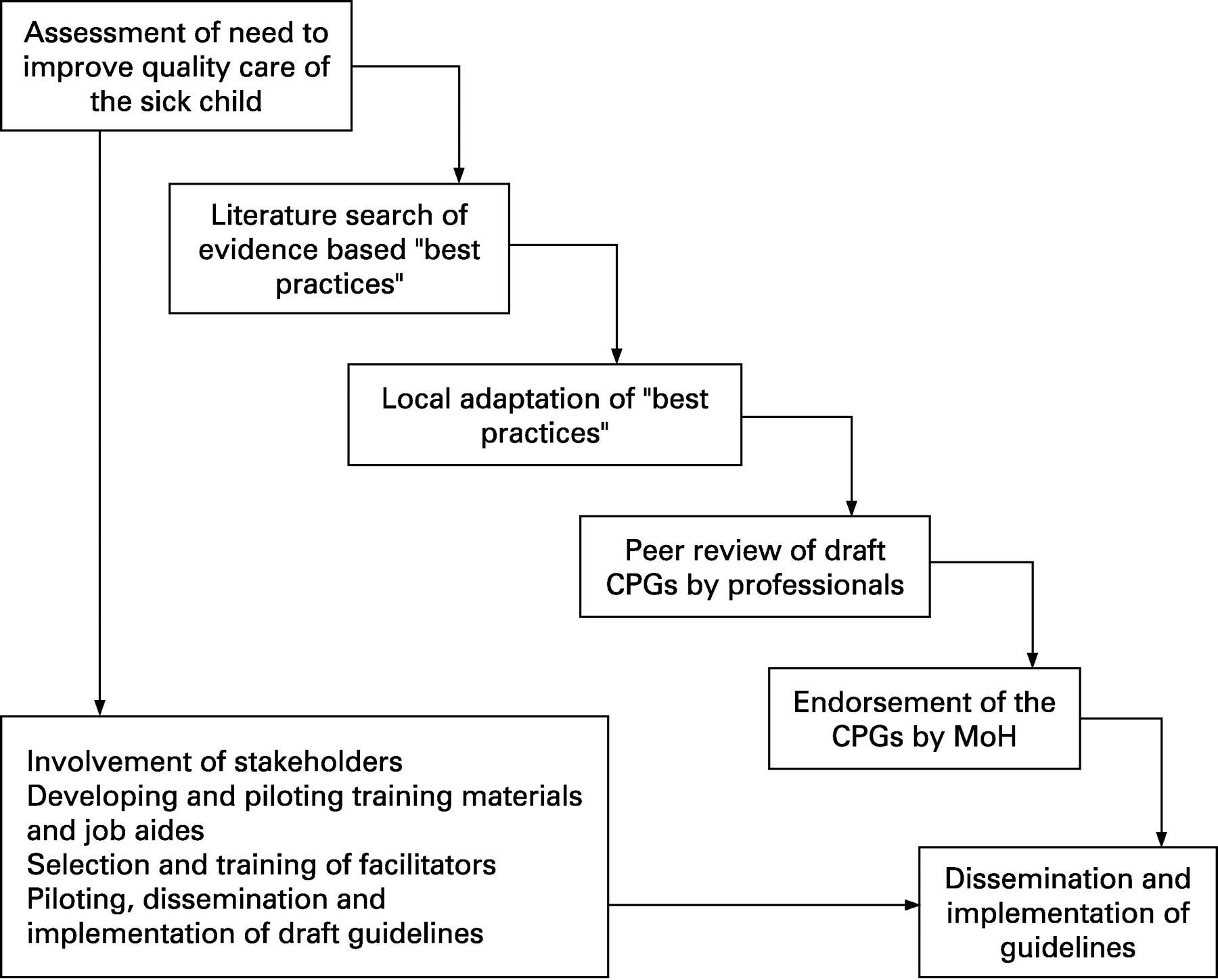
We therefore aimed to develop simple CPGs for conditions commonly associated with mortality in Kenyan hospitals and an in-service training package to facilitate their implementation. The effect on quality of hospital care of a multifaceted intervention project (including these CPGs and training) is the subject of ongoing research. Here we report the process of developing the CPGs and training, and our initial experience with a model for implementation (fig 1). We have previously reported the findings that established the need for improved paediatric care in Kenyan district hospitals.3

{kind=link}
DEVELOPMENT OF CPGS
Defining targets
Target illnesses responsible for more than 80% of paediatric hospital deaths locally2 16 were identified and included: malaria/anaemia, pneumonia/asthma, diarrhoea/dehydration, severe malnutrition, meningitis, neonatal sepsis, birth asphyxia and prematurity/low birth weight. In addition to these illnesses, lack of basic life-support, convulsions, hypoglycaemia and HIV were considered additional problems. For HIV the main focus was on recognition and diagnostic counselling and testing in line with available local guidelines.17
Consideration was then given to the potential major users of the CPGs. In Kenya most initial clinical care for hospitalised children is provided by clinical officers (who undertake a 3-year diploma training course) and nurses, the latter being the major providers of newborn life support and immediate care of the sick newborn in nurseries.2 Junior physicians provide some care, but senior physicians or qualified paediatricians are rarely available early in an admission.
Finally, the scope of the CPGs was considered. Most deaths of children in hospital in Kenya occur within 24–48 h of admission.18–20 The CPGs were therefore aimed specifically at trying to ensure that appropriate initial care could be provided by health workers with limited paediatric training by providing highly directive guidance on illness severity assessment and the use of 10 immediate and distinct, therapeutic, life-saving strategies, including cardiopulmonary resuscitation (newborn, infant and child), anti-convulsants, parenteral glucose, parenteral antibiotics, rapid acting bronchodilators, antimalarials, intravenous fluid resuscitation, specific nutritional support, oxygen and blood transfusion. In addition, explicit guidance was also given on the use, where available, of simple laboratory tests, including haemoglobin estimation, blood slide for malaria, HIV test, blood glucose and CSF microscopy.
Promoting local ownership
The effective absence of local guidelines for common conditions indicated in part a lack of recognition of their value for conditions as common as pneumonia or diarrhoea. As the results of early work3 suggested that any guidelines were likely to conflict with everyday practice, this problem was tackled, over 2 years, in a number of ways:
1) The first crucial step was a workshop, hosted by the Division of Child Health of the Ministry of Health (MoH), that included representatives from other MoH divisions, senior paediatricians from national referral hospitals, the private sector, university teaching hospitals, the Kenya Paediatric Association and the Kenya Medical Research Institute (KEMRI). Participants began the task of adapting to the Kenyan context the WHO recommendations for inpatient care.11 At this meeting the algorithm format of basic CPGs was presented and approved as a mechanism to assist in the implementation of the recommendations.
2) As appropriate to guideline development, attempts were then made to base the CPGs on the best available evidence. Thus, literature searches were undertaken and evidence summaries21 22 sought for all the identified conditions with the exception of infant and child resuscitation. These were undertaken according to the methods suggested by the International Child Health Review Collaboration (http://www.ichrc.org) and complemented this initiative, resulting in the development of a local database of evidence summaries and 434 key references.
3) After much of the evidence was collected and summarised, a dissemination forum entitled “Child Health Evidence Week” was hosted where eight local topic experts and two international experts presented and discussed the evidence with participants. The 36 participants were drawn from Kenya (26) and Tanzania (10) and consisted of senior academic/training staff from medical training schools (for nurses and clinical officers) and universities, the MoH and WHO.
4) Draft copies of the CPGs were produced under the auspices of the MoH Division of Child Health. These were reviewed by senior paediatricians from the University of Nairobi and the Kenya Paediatric Association and discussed in post-graduate teaching seminars at Kenya’s largest university medical school.
5) The final version of the CPGs was then reviewed within the Ministry of Health, endorsed and approved for publication as a 31 page booklet entitled Basic paediatric protocols.
DEVELOPMENT OF A TRAINING APPROACH TO ASSIST CPG IMPLEMENTATION
How adults learn
Training was based on conceptual models23–28 (table 1) and teaching methods29 that aim at improving knowledge translation and execution of recommendations through sequenced and multifaceted activities. It was directed at nurses, clinical officers and doctors to promote team working, as studies have shown that nurses can often perform as well as clinicians in basic initial steps of management.30–32 Both didactic and interactive sessions were delivered. Didactic interventions may change knowledge, skills or attitudes or may act as predisposing elements to change, particularly if delivered by a respected peer leader. Interactive sessions promote the use of acquired knowledge by participants and provide the opportunity to practice and hone skills.33 34 As successful adult education is learner-centred, active rather than passive, relevant to the learner’s needs, engaging and reinforcing,3 35–37 opportunities for questioning and reflection together with positive reinforcement and encouragement were a consistent feature of the course and defined the role to be played by facilitators.
Training course development
We initially adapted the existing WHO Emergency Triage, Assessment and Treatment (ETAT) course (http://www.who.int/child-adolescent-health/publications/CHILD_HEALTH/ETAT), adding a considerable amount of new material on newborn resuscitation and the common causes or consequences of serious illness in the newborn or child to produce “Emergency Triage Assessment and Treatment plus Admission Care” (ETAT+). The didactic training materials were initially tested for content and ease of understanding with 10 trainee paediatricians and two senior nurses. In the second step, the identified instructors were trained by the principal course designer over 5 days and each lecture and practical session was discussed. The training materials were then revised and compiled into a draft instructor manual. Three full-scale pilot training courses were then held in a district hospital not earmarked for the project (28 participants), the national hospital (14 participants) and a medical training college (34 participants). During and after each pilot training course, instructors discussed problems and revisions were made to the course materials and instructor manual.
The result was an ETAT+ course comprising 17 lectures interspersed with practical sessions (table 2). Practical sessions were undertaken in small groups (approximately eight people) and were designed to reinforce practice change messages and progressively build knowledge and skills using role play with manikins and simple equipment. Each practical session emphasised the assessment of airway, breathing, circulation and disability (ABC&D), the appropriate provision of life saving interventions, problem solving and team involvement. In addition, all training emphasised and encouraged the use of specific job aides including the Basic paediatric protocols booklet containing all the CPGs, drug and fluid dose charts and standardised paediatric and newborn admission record forms2 that focused attention on the symptoms and signs included in the CPGs.
The role of facilitators/instructors
Instructors or facilitators need to be authoritative and as a group present a consistent approach. Their selection and training is therefore likely to be critical to the ability of a course to influence practice. Our initial instructor group consisted of four paediatricians, two medical officers (equivalent to senior house officers) and one clinical officer working as a tutor in a medical training college. During development and pilot testing of the training course, all instructors and facilitators completed the Paediatric Advanced Life Support Course (PALS) and the UK Resuscitation Council’s Generic Instructors Course (GIC) in Kenya. The aim was to equip them with skills and techniques relevant to adult learning and teaching and harmonise their approach as instructors. Consistency amongst the instructors was further promoted by jointly providing group teaching and a rotating allocation of instructors to groups, lectures and practical sessions.
Promoting change
Although training tends to focus on changing knowledge, reluctance to change practice and unsupportive working environments may be significant barriers to knowledge use.38 Several strategies were therefore adopted at the individual and institutional level aimed at facilitating implementation of practices in line with the CPGs. This began with pre-course preparation as participants were sent authoritative WHO reading material39 40 approximately 1 month prior to the training course and informed that they would sit multiple choice and practical exams at the end of training. The course itself was delivered by credible and respected authorities, the role of evidence in developing the CPGs was emphasised and a majority of the training time was focused on the active use of knowledge and problem solving. To promote institutional change, we aimed to train a large number of personnel from different professions but a single institution together and incorporate active team working. We also incorporated self-assessment in the form of audit of patients’ hospital records and a hospital site and practice survey conducted by participants with discussions aimed at reflection on the gap between actual and desired practice.
Our initial experience with training to implement the CPGs through ETAT+
To reduce the cost of training, we planned for it to be conducted on-site or in the vicinity of a hospital. No payments were given to the participants, but refreshments and a midday meal were provided. Due to the nature of the training and the requirement for 32 staff to be available for 5.5 days, a preliminary visit was made to the four initially identified sites to explain and plan for the training course. Although the training was aimed at those with clinical responsibility for admitting sick children, pharmacists, nutritionists and laboratory staff were also invited for specified topics. Each hospital’s administrators actively co-operated to achieve this aim and also re-scheduled staff leave and some clinical services and, in some cases, arranged routine medical cover by consultant staff.
Details of who attended the training in the first four hospitals are provided in table 3. After the first day, when training rules were agreed, punctuality and attendance were excellent. The absence of any per diem payment did not result in absenteeism. The typical cost of providing one 5.5-day training course for 32 participants including all costs for the five facilitators was approximately US$5000 per site (although this does not include costs for course development and instructor training). As our aim was to promote understanding, use of and belief in the CPGs, participants were allowed access to these during the written, multiple-choice examination. Marks from this examination were affected by the extent to which participants took advantage of this and are thus not a very useful guide to individual performance. However, table 3 gives a summary of the participants’ practical assessment results. At the end of the training course we asked participants to evaluate the course components in terms of relevance and value, the feasibility of introducing the CPGs and their commitment to change using a self-administered questionnaire requiring responses on five-point Likert scales. Responses are described in table 4.
DISCUSSION
We have described the development of CPGs for emergency and hospital care for children (0–4 years of age) as well as a means for their implementation that has been attempted in four district hospitals in Kenya as part of a longer term evaluation of their impact. District hospitals are the primary targets for the CPGs as, although staffed by health workers with little or no specialist paediatric training, they are the major referral sites for sick newborns and children from peripheral health units and therefore represent the clinical service area with the greatest potential for reducing mortality.41
Interestingly, although aimed at the district hospital, the CPG booklets, which also contain drug, fluid and feeding guidelines, are being introduced by the MoH and WHO-Kenya to major provincial and national hospital settings and training facilities at a cost of US$0.85 per copy. This perhaps reflects the fact that the development of the CPG booklet was a long term, careful process that included the government, academics, clinical teachers, paediatricians and others from priority settings3 37 in guideline drafting, evidence review, development of job aides,2 peer review of draft guidelines and dissemination, thus enhancing local ownership. The CPGs produced consist of clear and direct recommendations for best practice in delivering emergency and early inpatient care for common problems and largely reflect the international recommendations for provision of life-support and care presented in the WHO Pocket book of hospital care for children. As such, our CPGs reflect an attempt to implement referral level or inpatient IMCI.
However, the CPGs will be useless if they are not understood and if recommended practices are not delivered appropriately. We therefore designed a training approach around the CPGs by adapting and considerably extending the scope of an existing WHO course (ETAT) to produce ETAT+. This course links our local CPG booklet and training to standardised admission forms that appear to be acceptable and effective,2 and should cost less than $30 per 1000 patients admitted. We hypothesise that the approach of institutional learning will promote change in the short term and minimise negative social influences.42 Such an approach could go some way to mitigate the effect of the rapid staff turnover that is a feature in many Kenyan hospitals. Training health providers of different clinical backgrounds together may also empower cadres with less perceived authority to prompt and promote change. Although there are challenges to delivering training at an institutional level, we have shown that district hospitals in Kenya are willing to work to make such an approach possible if given adequate time to prepare. Further, our decision not to offer a per diem payment (the former norm for training courses run by the government or NGOs) did not appear to effect training as 99% of the participants completed the course and punctuality was excellent. This, together with the decision to host the training courses in sites close to these relatively rural hospitals and the need for only five facilitators resulted in relatively low training costs.
From the beginning of training, our observations indicate that it became progressively apparent to the participants that there was a major gap between what they had been practicing and best practices possible even in a situation with limited resources. We feel this created a positive motivation for learning in order to change practice. Thus, by the end of the course over 80% of participants performed well in their practical assessment, nearly 20% excellently. We made no attempt to formally characterise those who performed poorly. However, our observations suggested that some of the older clinicians (although interestingly not nurses) with deeply engrained practices were the least likely to have completed their pre-reading, were the most likely to perceive change as disadvantageous in terms of the personal effort required and the least likely to perform well.
Decay of knowledge and loss of skills pose a real threat to the ongoing success of best practice care interventions.43 We are currently attempting to evaluate the real-life effectiveness of CPGs allied to support supervision in selected district hospitals. Further challenges for implementing and maintaining best practice care on a national scale include the capacity to update CPGs and sustain provision of job aides, to provide peer leadership and expert instructors, and, ideally, to integrate best practice into training institutions. Particularly if training institutions can promote the use of evidence and CPGs in Kenya, then in time an increasing number of health workers, sensitised to the concept and aware that practice change is ongoing, may accept and even demand updated best practice advice.
Acknowledgments
The authors would like to thank: all those who contributed to the development of the CPGs and in particular Dr Santau Migiro and Dr Assumpta Muriithi; the invaluable contribution of the ETAT+ instructors (Thomas Ngwiri, Violet Aswa, John Wachira and Patricia Mururi); Dr F Kimani, Deputy Director Medical Services for facilitating the secondment of Ministry of Health paediatricians to the training team; Dr SK Sharif, Deputy Director Medical Services for his ongoing support; and the administration and staff of all the hospitals involved in pilot and final training. In addition we are grateful to Elizabeth Molyneux, Sheila Simpson, Andrew Coleman, Roy Ellington and Ian Maconachie for advice on approaches to training and sharing their experience. The work reported was supported by KEMRI and the KEMRI/Wellcome Trust Research Programme and is published with the permission of the Director of KEMRI.
REFERENCES
Footnotes
Contributors: AW, FW, AW and NP helped oversee the development of the CPGs, participated in their review and production and helped co-ordinate key activities at each stage of the process. In addition, AW acted as the link between the project and the Ministry of Health. SN, PA and NO contributed to evidence reviews, production of the CPGs, development and refinement of ETAT+ training materials and (for SN) took part in ETAT+ course development and implementation. GI helped oversee the development of the CPGs, participated in their review and production, worked on the development and refinement of ETAT+ training materials, took part in ETAT+ course implementation and end of course evaluation and wrote the draft manuscript. ME conceived the idea for the major study, obtained funding for this work, helped oversee evidence synthesis and the development of the CPGs, participated in the review and production of the CPGs, produced the draft ETAT+ course and worked on its development and refinement, took part in ETAT+ implementation and end of course evaluation and oversaw the development of the manuscript. All authors reviewed and approved the final version of the manuscript.
Funding: This work was supported by The Wellcome Trust through a Senior Fellowship awarded to Dr Mike English (#076827). Support for the Child Health Evidence Week was provided by a grant from the David Baum International Foundation of the Royal College of Paediatrics and Child Health. The funders had no role in the design or conduct of the work reported and no role in preparing this report or the decision to publish.
Competing interests: None.