Article Text

Statistics from Altmetric.com
Developing a conceptual framework
In the last few decades in Britain successive acts of parliament have attempted to tackle discrimination and promote equality of opportunities for women, members of ethnic minority communities, and disabled people. Currently there is discussion about eradicating “ageism”, including within health services, although this term is used only to describe discrimination against older people.1 One group—children—despite experiencing profound discrimination within society, are omitted from the general equality debate. Indeed many would think it ridiculous to include them. In fact, as will be illustrated in this paper, children experience significant discrimination, from both individuals and institutions. This discrimination affects both their health and the quality and delivery of child health services.
BACKGROUND
There was a growing and global commitment to the promotion of children’s rights in the last half of the twentieth century, culminating in the UN Convention on the Rights of the Child in 1989 and the establishment of Children’s Rights Commissioners in several, mainly Western, countries. Among industrialised countries, only the USA did not ratify the Convention. Although the UK government did so (with some reservations) it has, relative to many of its European neighbours, been slow to respond to these developments, not adequately addressing the undoubted disadvantages children experience as a result of what is, in effect, a society inherently discriminatory against them.
At local and regional levels there has been more encouraging activity, with many local authorities, NHS Trusts, public health authorities, and schools making use of the Convention to inform strategies and services. Even so children, and children’s services, remain marginalised. Even when there is a genuine commitment to children’s rights, poor understanding of how discrimination against children—that is, “childism”, is manifest, is compromising efforts to develop policies and services that are truly centred around the Convention.
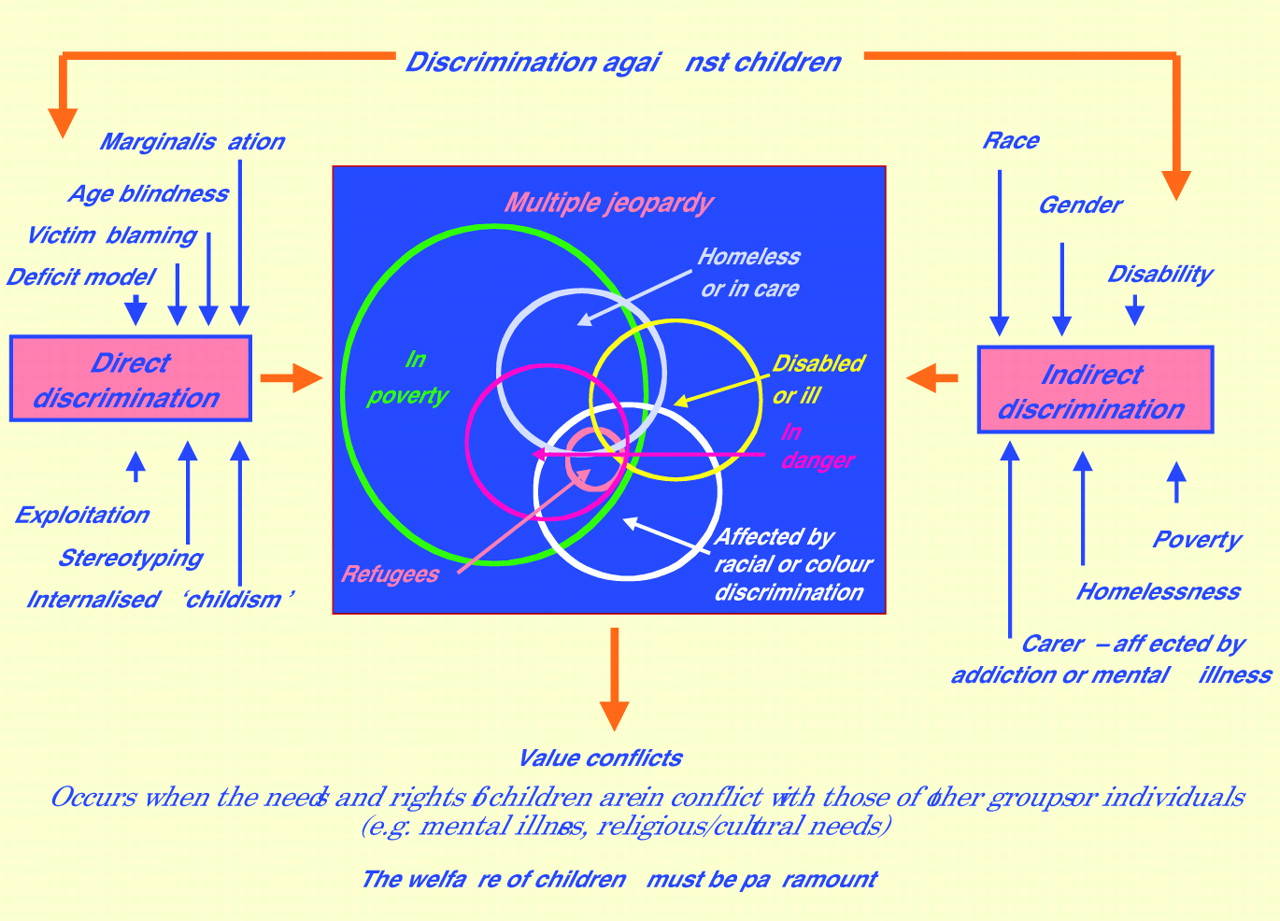
This paper will explore what forms this discrimination can take, the mechanisms via which it affects children, and its impact on health and health care. A conceptual framework will be developed (fig 1), using current understanding of racial discrimination (for which the debate is much more advanced) to better explain the concepts developed.
{kind=link}
Discrimination against children.
The definition of “a child” is as in the UN Convention—that is, those aged less than 18 years.
THE NATURE OF DISCRIMINATION
Discrimination can be direct or indirect. Indirect discrimination is the inequitable treatment of one group disadvantaging another, as opposed to direct discrimination in which the focus of discriminatory attitudes, actions, and policies is the group itself. Discrimination can act at the level of the individual, but can also be institutional. Institutional discrimination occurs when the structures or operating policies of organisations result in certain sections of the community being disadvantaged. This concept is most familiar as institutional racism,2 but can apply to any group disadvantaged by stigma and discrimination, including children.
Direct discrimination
This can be manifest in the following ways.
Overt discrimination
The late nineteenth and early twentieth centuries saw the beginnings of the exclusion of children from adult spaces, not for their safety or wellbeing but for the convenience of adults. This separateness of the child’s world is now seen as natural. The resulting discrimination is so much a norm that it is both ubiquitous and unrecognised, with hotels in the UK routinely refusing access to children (and dogs).
Marginalisation
“Through their constructed otherness, children’s status in British society is as non-persons relegated to a social, economic and political marginalisation”.3
Marginalisation is when a group experiencing discrimination is not seen as part of the core business or service. In the context of health care it is not only a modern phenomenon:
“… when sick children are admitted promiscuously with adults, the former never have so much attention paid them as the latter”.4
In 1994 both the confidential local audits performed by the Audit Commission (S Farnsworth and B Fitzsimon, personal communication, 1994) and other research5 revealed that the needs of children were not prioritised in the commissioning process. Little has changed since.6,7 When government first outlined plans for National Service Frameworks, they did not include the health of children. The implications of this marginalisation in policy, at local and national levels, for the health and welfare of children are fully explored by Aynsley-Green and colleagues.8
Children are similarly under-represented in funding for research and development, resulting in an inadequate evidence base for much paediatric practice,9,10 particularly evident in the development of new therapeutic drugs. Over two thirds (67%) of 624 children admitted to wards in five European hospitals received drugs prescribed in an unlicensed or off label manner.11 Although the problem is complicated by the ethical problems encountered around consent for child participation in trials,12,13 it is largely profit driven. Drugs are not tested in children and thus not licensed for paediatric use. Even licensed drugs are prescribed off label “resulting in children becoming therapeutic orphans sometimes with tragic consequences”.12
Age blindness
This is equivalent to colour blindness in racial parlance—treating everyone in the same manner, so ignoring or denying different needs. Such an approach can exclude children: for example, marina developments with inadequate barriers between toddlers and deep water.
Although huge strides have been made within the health sector to respond to the accommodation needs of children—providing facilities for play, and ensuring parents can accompany their children—there are still examples of poor practice, with shared waiting rooms in primary and secondary care in which carers have to spend considerable time with very young children in surroundings that are unsuitable and stressful.
The deficit model of childhood
Children are seen as immature—that is, incapable or unfinished; simply on the road to adulthood rather than people in their own right.
Children as incapable
We continue, for the most part, to exclude children from decision making or, at best, fail to take their input seriously. Although there is a commitment within the NHS to children’s participation in decision making14 and no shortage of guidance,15–19 participation in health service development remains exceptional. For example, of 509 Trusts and health authorities in the UK, only 27 consulted children on services for chronically ill or disabled children, and only 11 of these went beyond consultation to meaningful participation in policy.20 Young people with serious illness have reported feeling marginalised in decision making.21 Although there are problems in achieving full and meaningful participation, not least the competing rights of children and parents,21,22 children can be effective partners in the management of their own treatment,23 and there is plenty of convincing evidence from the Child-to-Child programme showing how children can contribute effectively to health alliances and transform their lives and health.24
Children as “immature”
Delinquency conceals two distinct categories, each with a unique natural history and aetiology. One group engages in antisocial behaviour at every life stage—“life course persistent”, whereas another is antisocial only during adolescence—“adolescence limited”. Adolescent onset delinquents do not share the pathological backgrounds found for those with life course persistent antisocial behaviours. Moffit and Caspi25 suggest that this phenomenon is a consequence of what he terms “a contemporary maturity gap” in which, in modern post-industrial societies, essentially mature individuals are infantilised by extended education and delayed work opportunities, resulting in antisocial behaviours “that are normative and adjustive”. This is an important issue. Around 25% of British men under 25 will have accrued criminal records to accompany them through their adult life, of which over half will have been adolescent onset delinquents.
Victim blaming
This term describes the phenomenon in which a vulnerable group are blamed when they experience disadvantage or harm.
Pedestrian injuries, a leading cause of childhood mortality, provide a good example. Children are blamed, with prevention strategies continuing to stress child behaviours, rather than addressing necessary and more effective changes in the structure of transport systems.
“The strength and pervasiveness of the ideology of victim blaming in child pedestrian injuries is explained by the special position that the road transport system holds in relation to dominant economic interests. Victim blaming ideology is a strategy that serves to maintain these interests at the expense and suffering of children”.26
Another example is the “Lolita” syndrome, in which children are blamed for their own sexual abuse. In 1993 a man found guilty of the rape of a girl, aged 9, was given two years’ probation. The presiding judge said: “I have been provided with information which leads me to believe that she was not entirely an angel herself”.27 Although Lord Taylor stated on appeal that this comment should not have been made, it is a view met elsewhere. On Alice Liddell, the girl with whom both John Ruskin and Lewis Carroll were infatuated, Prose writes: “what seems clear is that Alice was by no means a frail flower attracting these predatory bees; she pursued and actively encouraged their attentions”.28
Stereotyping
Children can be viewed as poor witnesses, more likely to lie than adults. This has had serious consequences for vulnerable children in care:
“The negative response (to complaints) especially in relation to reports of physical abuse, justified the pervading cynicism of most residents in care about the likely outcome of any complaints that they might make”.29
There is also a pervasive stereotype of children, particularly poor children, as inherently naughty, with distress frequently mistaken for “badness”. Research evidence shows clear links between life course persistent delinquency and abuse, poor parenting, poverty, and socially disorganised communities.30,31 Many of these young people also have neurodevelopmental problems, of which the most common is attention deficit hyperactivity disorder (ADHD).29,30 Growing up with abuse and violence can also lead to anxiety and attachment disorder, both of which may lead to children fulfilling criteria for ADHD. Some children with primary hyperkinetic disorders will also be abused, or subject to poor parenting. There is thus a complex inter-relationship between abuse/poor parenting, poverty, delinquency and neurodevelopmental difficulties32 which ought to, but does not, inform both preventive and responsive strategies to this problem. Instead governments of all persuasions in the UK have tended to focus largely on a punitive approach.
Internalised discrimination
Discrimination can be internalised. A member of a group experiencing discrimination adopts and shares the views of a hostile society, thus seeing him/herself as inferior. A powerful example of internalised racism is provided by Nelson Mandela in his autobiography.33 He describes an incident during a period of exile in which he panics on noticing that the pilot of an aeroplane in which he is travelling is black—even Mandela had internalised the view that a black person could not be capable of such a task.
Children also take on society’s view of themselves—as someone adults can pass in a queue unchallenged, as people having nothing to say worth hearing, as lawful victims of physical assault.
Exploitation
As with any powerless group, children are vulnerable to exploitation by the powerful—that is, adults. This may be private and secret, for example, the sexual exploitation of children within families. It may be commercially driven, for example, child labour (including sexual exploitation), advertising aimed at, or using, children; or politically driven—consider the exploitation of athletic prodigies in former Eastern Europe, given anabolic steroids in adolescence with serious consequences for their health.
Child labour is traditionally seen as a problem of low and middle income countries, but Field argues that we see emerging another equally exploitive form of labour—a tests and outcomes dominated education system, an “insatiable schooling industry” with education as “endless labour”.34 Although Field is writing about Japan, her work makes for uncomfortable reading.
Indirect discrimination
As children are dependent and powerless they are particularly vulnerable to indirect discrimination, in which their carers are disadvantaged as result of gender discrimination, racial discrimination, or the disadvantage many marginalised groups experience because they are poor, ill, disabled, or stigmatised for other reasons. Table 1 provides examples of how indirect discrimination affects children.
Indirect discrimination
Children may of course experience, for example, racism and sexism directly—a possible explanation for the high exclusion rate of African-Caribbean boys in UK schools,40 and certainly the cause of the excess mortality of girls in India.41 However, the focus of response strategies would still be to combat racism and gender discrimination, not childism per se.
For children, indirect discrimination always compounds direct discrimination, with some children experiencing multiple jeopardy. For example, a child may be disabled, belong to an ethnic minority community, be living in poverty, and have a parent with mental health problems. Such a child will be victim to layers of discrimination, all of which will affect his or her circumstances. The effects of such multiple disadvantage may not be simply additive, but act in synergy to paralyse services and leave children in danger.42
Racial discrimination as an example of indirect discrimination
Poverty
As a result of societal racism many black or ethnic minority (BEM) communities in the UK are at risk of poverty with some, notably the Pakistani and Bangladeshi communities, in “serious poverty”.43 Many adults in BEM communities are either unemployed or in low paid work, with their children more likely to attend poorly resourced inner city schools, be in the public care, and/or excluded from school. All these factors are linked with adverse health outcomes.
Access to information
Many parents in BEM populations, particularly mothers, do not have a working knowledge of English, and may not read. Without adequate provision of interpreters these parents are unable to access information crucial to their ability to make informed choices, to liaise with health, welfare, and education, and to advocate for their children when they are in need. Their situation is somewhat analogous to that of an illiterate mother in the developing world, a factor long known to be linked to high infant mortality.44 It would seem reasonable to hypothesise that the language status of unsupported migrant parents is likely to impact on the health of their children.
Access to health services
BEM communities do not have equality of access to services.45 There are examples of institutional racism. For example, services are dependent on postal addresses, which disadvantages asylum seekers and travellers. Services are often planned using whole population data. For BEM populations there is a mean age shift to the left. Nineteen per cent of white British people are aged under 16, but 38% of British Bangladeshis are under 16 (see table 2). Using whole population data to plan services ensures that areas with high BEM populations are undermanned and under-resourced for children’s services, despite the increased needs of these communities as a result of poverty.
UK % of ethnic groups aged under 1646
Services are also discriminatory in that they are culturally inappropriate, inaccessible, and with BEM clients stereotyped in ways that interfere with their care.44
VALUE CONFLICTS
These arise when the rights of one group are in conflict with those of another. The rights of children may conflict with those of other groups or individuals. This may be as a population; for example, the right of children to play in a safe place is often in conflict with the needs of car drivers. On an individual level there may often arise situations in which parental rights, religious rights, or cultural needs may appear to be in conflict with the wishes of children, or even their best interests. For example, a teenager may be in conflict with her parents with regard to whether or not to terminate her pregnancy. Such value conflicts are not easy to resolve, and may require the help of an independent advocate.47 In the context of child abuse, value conflicts can be extremely difficult to resolve, with the safety of children at odds with, for example, the right of a severely mentally ill parent to care for her children, or the right of religious or ethnic minority groups to discipline children in ways they regard as appropriate to their culture.36 Even within the Convention itself there may be conflicts; for example, the right of a child to be safe may conflict with the right to family life. It is imperative in such situations to focus firmly on Article 3 of the UN Convention of the Rights of the Child—what is in the best interest of the child?
CONCLUSIONS
In this paper a conceptual framework has been developed to describe the nature of discrimination against children. By applying this framework to the literature, and current political developments within the UK and beyond, examples of direct and indirect discrimination have been related to the health of children.
Children’s advocates, and that includes paediatricians, need not only to identify when children are being disadvantaged but why and how they are disadvantaged. Without an understanding of how discrimination affects children it is not possible to identify the appropriate focus for action in any particular case. Is a child being disadvantaged because she is a refugee, because she is disabled, or because all children’s services are not prioritised in a Primary Care Trust? The conceptual framework developed here provides a tool to improve the recognition of discrimination against children, and help identify the precise mechanisms by which any child, or group of children, is disadvantaged. This will enable advocates to more effectively combat discrimination against children and successfully implement the UN Convention.
Developing a conceptual framework
REFERENCES
Footnotes
-
This paper is based on a presentation first given to the Annual Conference of the European Forum of Child Welfare, Limmassol, May 2001