Article Text

Statistics from Altmetric.com
Neisseria meningitidis is the leading infectious cause of death in childhood in the UK.1 2 There were over 2500 cases and 246 deaths in 19973 and the disease has an overall mortality of about 10%.4 5 Although mortality rises to 50% in the most severely ill patients,4-6 data from our unit suggests that early recognition,7 aggressive resuscitation, specialist advice, and transfer to paediatric intensive care8 9 can reduce this mortality to less than 5%.10
Critically ill children are best managed in a specialist paediatric intensive care unit,11 but most patients with meningococcal disease will present to a hospital without tertiary care facilities and will require transport to a specialist centre. The immediate institution of lifesaving therapeutic measures is more crucial to patient outcome than the speed and urgency with which the paediatric intensive care retrieval team arrives.9Therefore, the resuscitation and stabilisation expertise available at the referring hospital must be harnessed while the specialist intensive care team is being mobilised. Decisions on when interventions (such as tracheal intubation) should be performed can be extremely difficult even for those who care for critically ill children on a regular basis. The decision making process at the referring hospital can be greatly facilitated by early telephone dialogue with a specialist centre.
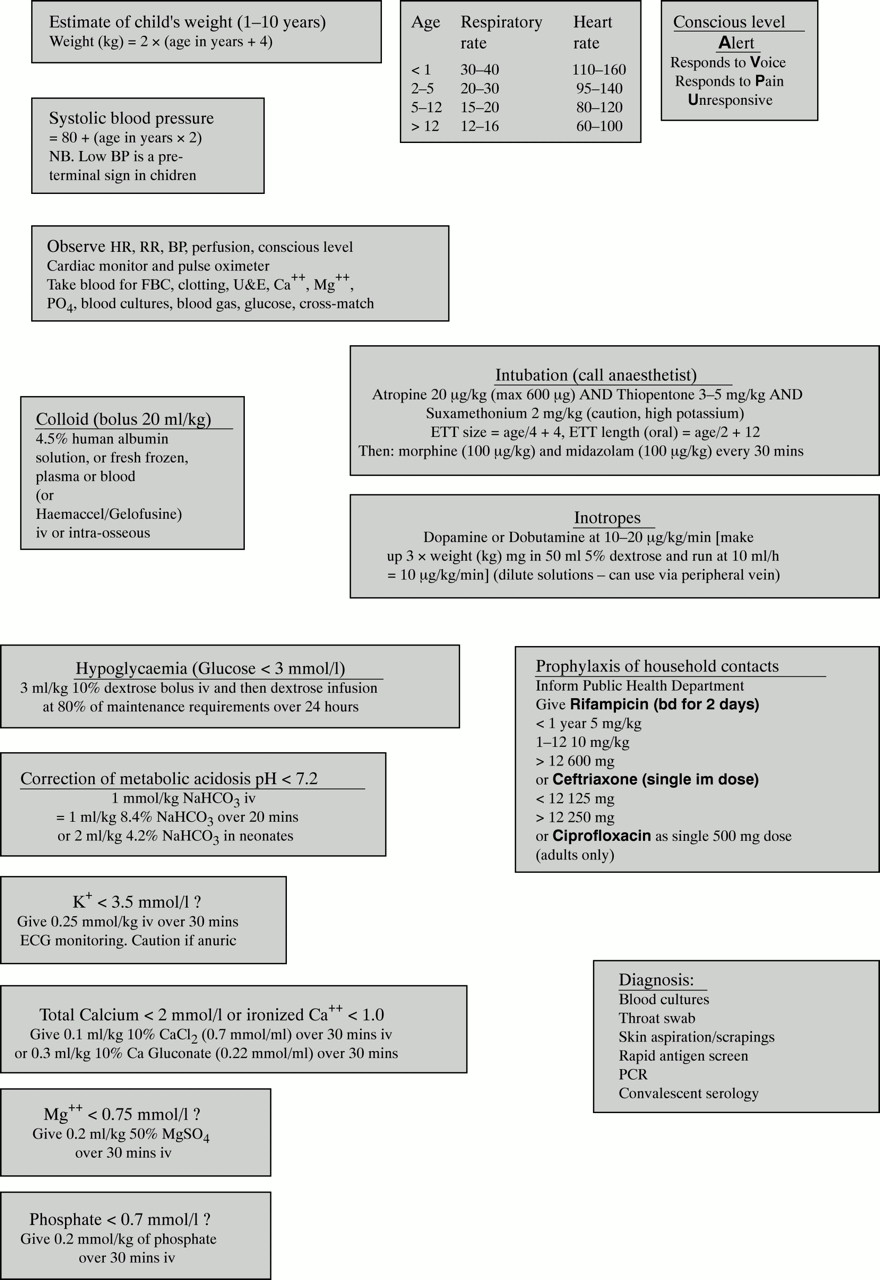
The department of paediatrics at St Mary’s Hospital in London, UK has a special clinical and research interest in meningococcal disease. Between June 1992 and September 1998, 425 critically ill children with meningococcal disease were referred to our paediatric intensive care unit from 72 different hospitals in the south east of England. The algorithm (fig 1 and 2 [AQ:1] ) presented in this article summarises our personal practice that has evolved as a result of this experience.

Algorithm for the early management of meningococcal infection. (Copyright Pollard AJ, Nadel S, Habibi P, Faust I, Maconochie I, Britto J, Levin M 1998. Department of paediatrics, Imperial College School of Medicine, St Mary’s Hospital, London.)
{kind=link}
{kind=link}
Information to complement the algorithm in fig 1. (Copyright Pollard AJ, Nadel S, Habibi P, Faust I, Maconochie I, Britto J, Levin M 1998. Department of paediatrics, Imperial College School of Medicine, St Mary’s Hospital, London.)
Recognition of meningococcal disease
Meningococcal infection should be suspected in any child who presents with a non-blanching rash as 80% of bacteriologically proved cases will develop purpura or petechiae.12 The remainder of cases have either a maculopapular rash (13%) or no rash (7%) but both of these groups may develop severe disease. In addition to the characteristic rash, features of meningitis or septicaemia may be present. Most children presenting with meningococcal infection will have features of meningitis alone, 7−10% have features of septicaemia alone, and 40% present a mixed picture of meningitis with septicaemia.6 8 13
It is likely that many casualty officers and junior paediatricians will not previously have seen a case of meningococcal disease and training of these front line staff should include familiarisation with the clinical features. The initial diagnosis is clinical, and management should not be delayed while waiting for the results of laboratory investigations. Markers of an acute phase response (raised white cell count and C reactive protein) may be absent early in the course of the disease, especially in severe cases.14 15 Furthermore, in 50% of cases where meningococcal disease is suspected clinically, there is no laboratory evidence of the disease (cultures of blood, cerebrospinal fluid (CSF), throat swab or latex agglutination tests).
The clinical course in severe cases is rapidly progressive and mortality is high. Therefore, once the diagnosis of meningococcal disease is suspected, the appropriate consultant in the accident and emergency department, paediatrics, anaesthetics, or intensive care should be involved at an early stage while the process of evaluation and initial resuscitation is started. Although many affected children may not appear severely ill at presentation the disease may rapidly progress even after admission to hospital and starting appropriate treatment.7 Even children who appear well on admission must be closely monitored and repeatedly reviewed over the next 24 hours.
Depending on whether septicaemia or meningitis predominates, the major clinical management problem may be shock or raised intracranial pressure. In some cases both may be present, and others with mild disease have neither shock nor raised intracranial pressure.
Recognition of shock
Shock is a clinical diagnosis. Signs of early shock in children arise from the compensatory physiological processes that maintain perfusion of vital organs at the expense of perfusion of non-vital organs. Compensatory mechanisms include tachycardia and peripheral vasoconstriction (cold peripheries and prolonged capillary refill time), which maintain circulating blood volume and thereby stroke volume and cardiac output. Decreased urine output is a sign of renal hypoperfusion (< 1 ml/kg/h of urine measured with a catheter in the bladder). A decreased level of consciousness reflects central nervous system hypoperfusion and/or hypoxia. Metabolic acidosis reflects tissue hypoperfusion.
Shock should not be equated with hypotension. Previously well children with intact homeostatic mechanisms can compensate very well during hypovolaemic states. Changes in consciousness level and systemic hypotension signify the presence of decompensated shock, which is a premorbid event.16
Tachypnoea and hyperventilation are frequently seen in early shock and reflect several pathological processes. Hypoxia due to impaired oxygenation, decreased oxygen delivery, or increased oxygen extraction could manifest as tachypnoea. The increase in ventilation defends arterial Po 2 and attempts to correct the acidosis caused by tissue hypoperfusion. The increase in ventilation may also reflect pulmonary oligaemia in decompensated shock or onset of pulmonary oedema as a result of the capillary leak syndrome in the pulmonary vasculature.
Pathophysiology of shock in meningococcal disease
Septic shock in meningococcal disease results from loss of circulating plasma volume due to increased vascular permeability, maldistribution of intravascular volume due to changes in vasomotor tone, impaired myocardial function,17 and impaired cellular metabolism.8 Increased vascular permeability develops early in the course of meningococcal shock. Leakage of plasma proteins, including albumin, and water from the intravascular compartment into the interstitium results in hypovolaemia, decreased filling pressure of the heart, and, in turn, decreased stroke volume and cardiac output.
The pathogenesis of myocardial dysfunction in septic shock is multifactorial.18 Metabolic derangements (hypoxia, acidosis, hypokalaemia, hypocalcaemia, hypophosphataemia, hypomagnesaemia, hypoglycaemia, and disturbed fatty acid metabolism) may also have an important role. In addition, bacterial mediators, the host inflammatory response,17 18 and an ill defined circulating myocardial depressant factor have been proposed as contributing to myocardial depression.19
Initial assessment
Initial assessment of the patient with meningococcal disease should include careful attention to patency of the airway, and adequacy of breathing and circulation. Emergency life support should start where indicated by this assessment. In most cases of severe disease, shock or raised intracranial pressure are the primary life threatening pathological process. Initial assessment should therefore define whether shock or raised intracranial pressure are the predominant problems. As shown in fig 1, subsequent management differs for the children in each category.
Circulatory support
The goal of circulatory support in shock is maintenance of tissue perfusion and oxygenation. The priority in achieving this goal is volume resuscitation to restore the intravascular compartment. Early fluid resuscitation is associated with improved survival.20 In addition, myocardial support with inotropes is frequently necessary to maintain end organ perfusion in more severely ill patients.
Peripheral venous access can be difficult in young children and may be impossible in shock. If attempts at peripheral intravenous cannula placement are unsuccessful after a few minutes, intraosseous access should be secured without delay.21 Establishment of central venous access, although desirable, can delay resuscitation and should wait until after initial stabilisation.
An initial bolus of 20 ml/kg colloid should be given over five minutes22 to children with signs of shock. The expected response to volume replacement is reduction of heart rate and improvement in peripheral perfusion (warming of peripheries and shortening of capillary refill time). In mild cases, where shock is rapidly reversed by this initial fluid bolus, repeated review is mandatory as the disease may progress and shock reappear even after initial stabilisation owing to ongoing capillary leak.
When signs of shock persist after an initial 20 ml/kg colloid, a further 20 ml/kg should be given over 5−10 minutes.20 If signs of shock persist after 40 ml/kg, there is a significant risk of pulmonary oedema and elective intubation and ventilation should be undertaken, even in the absence of signs of respiratory failure (see below). Continued volume resuscitation is required for persistent signs of shock. As myocardial depression invariably coexists with severe volume depletion, inotropic support should be initiated in patients who have persistent shock after 40 ml/kg of fluid. It is usually impractical to gain central venous access before intubation. Dilute solutions of dobutamine or dopamine can be given as an infusion through a peripheral vein until the airway is secured and central venous access is obtained. These drugs must be used cautiously because of the risks associated with extravasation. In refractory meningococcal shock, infusion of adrenaline, noradrenaline or both16may be required but they should only be infused into a central venous catheter.
The adequacy of volume replacement treatment should be monitored using heart rate, blood pressure, central venous pressure, urine output, metabolic status, and peripheral perfusion as indicators. It can be very difficult to decide whether persistently shocked children require further volume replacement or myocardial support with inotropes. Inotropic support should be initiated concurrently with continued volume resuscitation. Some children with severe capillary leak syndrome are only stabilised after replacement of more than twice their blood volume with colloid solutions and concurrent inotropic support.
Although, there is controversy about the use of human albumin solution for volume replacement treatment,23 24 4.5% human albumin solution has been the main resuscitation fluid in meningococcal sepsis for several decades. In our experience of treating 425 children, the exclusive use of albumin has been associated with the lowest mortality yet for severe disease.10 Until further evidence is available that other colloid preparations are as effective as human albumin solution in the support of meningococcal patients with profound capillary leak, it is difficult to justify a change in practice.24
Placement of a urinary catheter is an important part of the emergency management of shocked children, as urine output is a sensitive index of end organ perfusion.
Respiratory support
High flow oxygen should be delivered routinely during the initial assessment of the patient. If there is no major problem in airway or breathing, priority is given to the assessment and treatment of shock. However, early, elective intubation should be considered mandatory in any child who has persistent shock after 40 ml/kg of volume resuscitation as intubation and ventilation protects the airway, reduces the risk of pulmonary oedema, facilitates adequate oxygenation and ventilation, and reduces the work of breathing and oxygen consumption.25 26 Indications for immediate endotracheal intubation to protect the airway are decreased consciousness level (Glasgow coma score < 8), signs of raised intracranial pressure, hypoxia and/or respiratory failure, pulmonary oedema, and hypotension (decompensated shock).
Rapid sequence intubation using atropine, thiopentone, and suxamethonium is preferred.27 The aim should be to intubate before decompensated shock or severe hypoxia occurs, as induction of anaesthesia may exacerbate hypotension with worsening of shock as a result of vasodilation and removal of sympathetic drive. Children with decompensated shock may further deteriorate on induction unless close attention to volume resuscitation and inotropic support is made before, during, and after ventilation. In this situation ketamine is preferred over thiopentone as it causes less cardiovascular compromise. Boluses of colloid and inotropes should be drawn up and available to give if shock worsens during intubation.
Correction of biochemical and haematological derangements
There has been increasing awareness that children with meningococcal sepsis have profound derangements in metabolism.8 28 These abnormalities in the metabolic environment may contribute to myocardial depression and should be corrected. Anaemia and hypoglycaemia are common findings and should be detected by repeated blood testing, and treated. A 10% glucose infusion should be started as maintenance fluid early in resuscitation to prevent hypoglycaemia. Coagulopathy is common and is probably caused by both consumption of clotting factors and their loss through capillary leak. There may be bleeding from venepuncture sites and even pulmonary, gastric or cerebral haemorrhage, particularly if there is associated thrombocytopenia. Correction of coagulopathy with fresh frozen plasma and, in severe cases, cryoprecipitate, may prevent life threatening haemorrhage. In general, correction of thrombocytopenia is not required but if haemorrhage from venepuncture sites or spontaneous mucous membrane bleeding occurs despite replacement of clotting factors, platelet transfusion may be required. Metabolic acidosis is invariably present in severe shock. Although the use of bicarbonate is controversial, severe acidosis impairs myocardial contractility and, if the pH is < 7.2, sodium bicarbonate should be infused (fig1).16 Acidosis and oliguria would be expected to cause hyperkalaemia but, paradoxically, most patients with meningococcal shock have hypokalaemia.29 30 In view of the impaired myocardial function and risk of arrhythmia associated with low serum potassium, hypokalaemia should be corrected. Hypocalcaemia is also common in sepsis31 and is corrected with the intention of achieving stabilisation of myocardial function and improving blood pressure,32-34 although calcium supplements in sepsis remain controversial.35 36 If there is also hypomagnesaemia, hypokalaemia may be refractory to treatment37 and potassium homeostasis improves when magnesium is maintained at high normal values.38Hypomagnesaemia may cause cardiac arrhythmias and has been associated with increased mortality in sepsis.32 Phosphate is important for tissue oxygen utilisation, glycolysis, smooth and striated muscle strength (including diaphragmatic), and left ventricular contractility.39 Symptoms are unusual until serum phosphate falls below 0.32 mmol/l.40 These features of hypoposphataemia are mainly related to ATP depletion. Hypophosphataemia should be corrected if serum phosphate falls below 0.7 mmol/l as phosphate. Repeated biochemical monitoring to detect electrolyte abnormalities should be undertaken at hourly intervals during resuscitation and derangements corrected as described in fig 1.
The child with raised intracranial pressure
Although most critically ill children with meningococcal infection have shock as their primary clinical problem, a proportion present with signs of raised intracranial pressure. Most patients with meningitis have mildly raised intracranial pressure,41 however, clinically significant raised intracranial pressure is an uncommon presenting feature of meningococcal disease. Signs of raised intracranial pressure include a declining level of consciousness, focal neurological signs including unequal, dilated or poorly responsive pupils, hypertension, and relative bradycardia. Papilloedema is a late finding in acute raised intracranial pressure. Sending a child for computed tomography (CT) may delay lifesaving treatment. Moreover, detection of raised intracranial pressure depends on clinical features and is not reliably shown by CT.42 In a patient with raised intracranial pressure, infusion of mannitol and elective intubation is indicated as suggested in fig 1.
In the assessment of the child with raised intracranial pressure from meningococcal infection, initial assessment may reveal coexistent shock. In this case the priority of management is to correct the shock before addressing specific measures to control intracranial pressure. An adequate blood pressure is necessary to perfuse the brain, particularly if the intracranial pressure is raised. In the presence of raised intracranial pressure, the airway should be secured and the child should be intubated and ventilated to control CO2 in the low normal range.43 A common error is to undertake intubation but then fail to monitor CO2 and maintain adequate ventilation. Repeated blood gas analysis and end tidal CO2 monitoring is essential following intubation to avoid hypercapnia. Failure to do this may cause a rise in CO2that would be associated with an increase in cerebral blood flow and a further rise in intracranial pressure. Sedation is essential following intubation to prevent spikes in intracranial pressure caused by agitation and coughing. Diuretic treatment with either frusemide or mannitol may control raised intracranial pressure.43
Neurointensive care should be instituted using a 30° head up position, head midline, minimal suction, deep sedation, and strict avoidance of hypercapnia.44 Ideally the internal jugular vein should be avoided for central venous line placement as these catheters and positioning the patient for their insertion may reduce venous return from the brain and raise intracranial pressure further. In this situation the femoral vein is the safest option. Maintenance crystalloid need not be restricted in meningitis.45
Lumbar puncture
Lumbar puncture may be temporally associated with deterioration in some patients with meningococcal disease because of exacerbation of cardiorespiratory compromise or the risk of cerebral herniation.7 42 46 Therefore, lumbar puncture should be avoided where there is cardiorespiratory insufficiency, raised intracranial pressure, or coagulopathy.47 48 Indeed, lumbar puncture should probably be avoided or deferred in the initial assessment of all patients with clinically obvious meningococcal disease because the additional information provided by the procedure adds little to the diagnosis.
Antibiotics
Cefotaxime (80 mg/kg) or ceftriaxone (80 mg/kg) is preferred asinitial treatment in shocked patients with a clinical diagnosis of meningococcal disease. Penicillin resistance is rare among clinical isolates of N meningitidis in the UK and this antibiotic is the logical choice when the microbiological diagnosis has been made. However, until microbiological information is available, there remains the possibility of both penicillin resistance or alternative bacterial diagnosis that might not be adequately treated by penicillin. Other rare bacterial causes of purpura fulminans include Streptococcus pneumoniae, Staphylococcus aureus, and Gram negative septicaemia.
Steroids
Steroids given with the first dose of antibiotics reduce the incidence of neurological sequelae in bothHaemophilus influenzae type b and pneumococcal meningitis in children.49 Although data are not available for meningococcal meningitis, the pathophysiological events are likely to be similar to those in other forms of bacterial meningitis. Systemic dexamethasone should be given in cases of suspected bacterial meningitis with the first dose of antibiotics in an attempt to reduce the incidence of neuronal damage.49-52A dosage of 0.15 mg/kg four times a day for four days is generally recommended53 but 0.4 mg twice a day for two days is equally effective.52 Steroid use is not indicated in meningococcal shock in the absence of meningitis.54 55However, if hypoadrenalism is suspected because of unresponsive shock, adrenal replacement doses of hydrocortisone may be given.
Diagnosis
The diagnosis of meningococcal disease is based initially on typical clinical features but cultures of blood, throat, CSF (in the absence of contraindications) and skin aspirates may provide microbiological confirmation. Rapid latex antigen tests may assist with diagnosis but have a high false negative rate.56Polymerase chain reaction of blood or CSF to detect meningococcal genome is particularly helpful in confirming the diagnosis in patients who have already received antibiotics.57-59 Serology may be helpful if a rising titre is later demonstrated in the convalescent phase.
Transfer to intensive care
Most children presenting with meningococcal disease will not require intensive care. However, those with persistent shock after initial volume resuscitation (> 40 ml/kg) or signs of raised intracranial pressure should be managed in a specialist paediatric intensive care unit. The decision to move such children can be difficult. A prolonged period of resuscitation may be necessary in the accident and emergency department before a child with profound shock is stable enough to move. Transporting children before they are resuscitated adequately can be hazardous and the child should be fully stabilised and monitored before moving to the paediatric intensive care unit. Transport related morbidity and mortality is reduced by the use of a specialist paediatric intensive care team.9
Public health
Policy in the UK is to provide antibiotic chemoprophylaxis to household contacts of the child with meningococcal disease.60 In practice this usually involves only the child’s immediate family. It is often convenient to arrange this at the hospital where the child is admitted. Questions are often posed by parents and other contacts about wider chemoprophylaxis but these should be referred to the local consultant in communicable disease control as the issues involved are complex. Notification of cases of meningococcal disease is a legal requirement.
Summary
Meningococcal disease remains a major cause of mortality in children in the UK. Aggressive early volume resuscitation, meticulous attention to the normalisation of all physiological and laboratory parameters, and prompt referral to specialist paediatric intensive care may lead to a sharp reduction in mortality. Application of the management algorithm described in this article may be helpful to those involved in the early part of management of critically ill patients with meningococcal disease.
Acknowledgments
We are grateful to all the staff of the paediatric intensive care unit at St Mary’s Hospital for their assistance in the evolution of this article. We are especially grateful to Ian Maconochie and Saul Faust for their helpful comments in the construction of the algorithm.
References
Linked Articles
- Rapid responses
- Rapid responses