Article Text

Statistics from Altmetric.com
This paper is intended to provide evidence-based recommendations about the assessment and clinical management of infants and children with acute gastroenteritis. These guidelines were derived from a systematic review of published research. The diagnosis of gastroenteritis is not addressed; this is often presumptive and is based on a history of acute diarrhoea in the absence of other likely explanations. Microbiological investigation is not necessary in every case, but may be important in patients who require admission to hospital, in those who have bloody or mucoid diarrhoea suggesting colitis, in high risk patients such as those with an immune deficiency, and in cases where there is diagnostic uncertainty. Clinicians should apply general medical knowledge and clinical judgment in using these guidelines.
Scope of guidelines
The topics addressed are: assessment of the risk of dehydration; assessment of the degree of dehydration; oral rehydration therapy (ORT); strategies for rehydration and maintenance of hydration; management of hypernatraemic dehydration; nutritional management during and after the illness; and the role of pharmacological agents including antidiarrhoeals and antimicrobials.
Systematic review: search strategy and evaluation of the evidence
The search was performed using the medline and Cinahl databases, and covered the years 1966–97. Some relevant articles were also identified from the references cited in publications identified from these databases. The search was limited to studies of human subjects published in English. Subject headings employed were: “gastroenteritis”, “diarrhoea”, “rehydration solutions”, “dehydration”, and “hypernatraemia”. Textword searches were also done using the terms “infectious diarrh$”, “oral rehydration solution$”, and “hypernatr$ dehydration”. For each topic the terms “review”, “meta-analysis”, “randomised controlled trial”, “cohort study”, and “case control study” were applied. The Cochrane Library database of systematic reviews was searched under subject headings. Evidence from the medical literature and the strength of the recommendations given were then categorised according to a previously described scheme (table1).1
Categories of evidence and recommendations
Assessment of hydration
The risk of dehydration or, if already established, the severity of dehydration, can be assessed from a patient’s clinical history and physical examination.
RISK FACTORS FOR DEHYDRATION
The risk of dehydration in children is related to age.2 Young infants have an increased surface area:body volume ratio resulting in increased insensible fluid losses. They receive milk as the main source of nutrition; this constitutes a large osmotic load that may promote an osmotic diarrhoea, and a large protein load resulting in a high renal solute load. Finally, infants have an inherent tendency to more severe vomiting and diarrhoea compared with older children and adults.
It is logical to assume that severe symptoms, including frequent vomiting and watery diarrhoea, would predict an increased risk of dehydration. Retrospective case-control studies from developing countries have confirmed this.3 4 Studies from the Indian subcontinent have identified failure to give oral rehydration solution (ORS) and discontinuation of breast feeding during the illness as the greatest risk factors for dehydration.4 5 In those studies other variables contributing to risk included age (< 12 months), frequent stools (> eight/day), vomiting (> twice/day), and severe undernutrition. In studies from South America of children < 2 years old with acute diarrhoea, the use of bottle feeding rather than breast feeding was identified as an independent risk factor for dehydration.6 7 In a study on the significance of specific pathogens, Vibrio cholerae was associated with a high risk of dehydration, while other pathogens including rotavirus, Campylobacter jejuni, and enterotoxigenic Escherichia coli were comparable with one another with respect to risk of dehydration.8
CLINICAL ASSESSMENT OF HYDRATION
The severity of dehydration is usefully expressed in terms of weight loss as a percentage of total body weight. If a recent weight record is available (for example, from the parent held medical record) dehydration can be estimated with some accuracy.
The severity of dehydration can also be determined using certain specific clinical criteria. In a prospective cohort study of subjects between 3 months and 18 months of age, multiple regression analysis selected “prolonged skinfold”, dry oral mucosa, sunken eyes, and altered neurological status as the clinical signs that best correlated with dehydration as determined by pre-rehydration and post-rehydration weights.9 In that study, those subjectively judged to be “mildly dehydrated” showed weight gains of 3.6–3.9%, “moderate dehydration” was associated with weight gains of 4.9–5.3%, and “severe dehydration” with weight gains of 9.5–9.8%.
Capillary refill time (> 2 seconds) has been proposed as a useful indicator of dehydration.10 This technique lacks sensitivity and specificity, but a normal capillary refill time is very unlikely with severe dehydration.11 12
Recommendations on assessment of hydration
-
Assess risk of dehydration on the basis of age (highest in young infants) and frequency of watery stools and vomiting [II,B]
-
Assess presence/severity of dehydration on the basis of recent weight loss (if possible) and clinical examination. Signs of proved value in assessing dehydration include “prolonged skinfold”, dry oral mucosa, sunken eyes, and altered neurological status [I,A].
Fluid management
In children with clinical evidence of dehydration, biochemical investigations including serum electrolytes, urea, and creatine and assessment of acid/base status may be helpful. Irrespective of the serum electrolyte concentrations, however, dehydration from gastroenteritis is invariably associated with total body deficits of sodium and chloride. In addition, there is often significant potassium depletion and acidosis. Hyponatraemia and hypernatraemia are simply indicative of the relative losses of water and sodium. The rehydration fluid should replace both water and electrolyte losses. In many cases an initial phase of rehydration is necessary, followed by a fluid maintenance phase aimed at preventing the recurrence of dehydration (fig 1).

Management of hydration in gastroenteritis.
ORAL REHYDRATION THERAPY
In all but the most seriously ill patients rehydration is possible using ORT. The effectiveness of ORT was first proved 30 years ago in major clinical studies undertaken during cholera epidemics in Bangladesh.13 14 These studies were possible after the discovery in the 1960s that intestinal water absorption was mediated by an active transport process in which sodium and glucose were cotransported in an equimolar ratio. Studies in the laboratory animal showed that glucose stimulated intestinal sodium absorption.15 Studies in human subjects confirmed this observation in man, and showed that the sodium-glucose cotransporter continued to function in patients with cholera.16-19Subsequently, controlled studies showed the effectiveness of ORT in infants and children with non-cholera diarrhoea.20 21
The use of ORT in the management of gastroenteritis in the UK was associated with a dramatic fall in mortality, from 300 deaths annually in the late 1970s to about 25 in the late 1980s.22Hypernatraemic dehydration, a major cause of mortality in acute gastroenteritis, also became much less common.23
COMPOSITION OF ORAL REHYDRATION SOLUTIONS
A range of ORS products are currently available, and these vary markedly in their sodium and glucose concentrations (table 2). Although these are generally effective in the treatment and prevention of dehydration, there has been controversy about the ideal composition for ORS.14 24
Composition (mmol/l) of available oral rehydration solution preparations
Sodium
In the 1970s the World Health Organisation (WHO) adopted a glucose-electrolyte solution (WHO-ORS) containing 90 mmol/l of sodium, and this was promoted for worldwide use. This solution was originally evaluated in adults with cholera or cholera-like (toxigenic) diarrhoea, the category of patients for whom it was primarily designed. Later, however, its use was extended to children with non-toxigenic diarrhoea, including rotavirus gastroenteritis.25 In the underdeveloped world, diarrhoeal disease is often associated with large stool sodium losses.24 In patients in Western countries, sodium loss is generally less severe, and so there has been concern about the risk of hypernatraemia with WHO-ORS, especially in infants < 3 months of age.26 27 Moreover, controlled clinical trials in infants < 3 months and in older children have shown that an ORS with a sodium concentration in the range 50–60 mmol/l is safe and effective in the treatment and prevention of dehydration.28-33 The European Society for Paediatric Gastroenterology and Nutrition (ESPGAN) published guidelines based on these studies, recommending a sodium concentration of 60 mmol/l for European children.34
Glucose
The ideal carbohydrate concentration in ORS must be related to the sodium concentration. The WHO has recommended a glucose:sodium ratio of less than 1.4:1.14 Hyperosmolar ORS containing excessive amounts of carbohydrate could induce osmotic diarrhoea as a result of carbohydrate malabsorption, and the associated water loss would increase the risk of hypernatraemia. ESPGAN has therefore recommended the use of a hypo-osmolar ORS for European children.34
Glucose may be provided as monosaccharide or as a complex carbohydrate (for example, glucose polymer or starch). Complex carbohydrates have the theoretical advantage of forming solutions of reduced osmolality, although they require digestion before absorption. In underdeveloped countries, cereal based ORS has been successfully employed.35 A recent meta-analysis of 13 clinical trials examined the effect of rice based ORS on stool output and duration of diarrhoea; there appeared to be a worthwhile benefit in patients with cholera, but the effect in children with acute non-cholera diarrhoea was uncertain.36 Appropriately therefore most solutions currently in use contain glucose as monosaccharide (table2).
Potassium, bicarbonate, and base precursors
Most ORS products contain 20 mmol/l of potassium, and this appears sufficient to prevent hypokalaemia despite individual variation in stool potassium losses.24 Most contain bicarbonate, or more often a stable base-precursor such as acetate, lactate, or citrate. These constituents were originally included to correct the acidosis that may accompany dehydration, and to promote water and sodium absorption. In fact there is no evidence that inclusion of base is necessary or beneficial.24
REHYDRATION
In the past many regimens aimed at gradual rehydration over 24 hours or longer, but this approach was not evidence based. It seems both illogical and potentially disadvantageous to delay the process of recovery in these children by prolonging the rehydration process. Nowadays most authorities recommend rapid rehydration over a three or four hour period.2 13 14
The degree of dehydration is estimated as outlined above and expressed as percentage of body weight. The fluid deficit can then be calculated: thus, an estimated 5% dehydration would be treated by giving 50 ml/kg of replacement fluid. ORS may be given by bottle, cup, or spoon as appropriate, and frequent administration may be necessary to repair the deficit within four hours. Most dehydrated children are thirsty and will take fluids readily, but some seriously ill children may require ORS given via an enteral tube. Rehydration should be done under medical supervision, and the state of hydration should be reassessed during rehydration and at the end of the four hour rehydration period. If the patient is still dehydrated then the residual deficit is again estimated and the rehydration process is continued. If children vomit during the process of rehydration, more ORS is immediately given.
Most authorities recommend that children with signs of shock (inadequate perfusion of vital organs) should receive intravenous rehydration initially.2 14 Although oral rehydration is quite possible in such cases, the intravenous route helps to guarantee rapid rehydration in these critically ill patients.
In cases of hypernatraemic dehydration (serum sodium > 150 mmol/l) slower fluid replacement over 12 hours has been recommended to reduce the risk of seizures (“slow ORT”).37 There is a consensus that the use of ORT can in itself reduce the risk of seizures during rehydration.14 In one report none of 34 infants with hypernatraemic dehydration suffered seizures when rehydration was repaired with WHO-ORS over 12 hours.38 In the largest published controlled trial of intravenous versus oral rehydration, 470 children under 18 months of age, all with severe gastroenteritis, were randomly assigned to receive either ORS or intravenous fluid.39 Of 34 hypernatraemic patients in the ORT group, 2 (6%) developed seizures compared with 6 of 24 (25%) in the group given intravenous treatment. These studies are reassuring, although it may be significant that WHO-ORS (sodium 90 mmol/l) was used, as opposed to the ORS currently recommended in Europe (sodium 60 mmol/l). It is therefore important that the serum sodium concentration be closely monitored during rehydration because rapid reductions are associated with an increased risk of cerebral oedema and convulsions.
MAINTENANCE TREATMENT
Various strategies have been recommended to prevent dehydration and to prevent the recurrence of dehydration from ongoing fluid losses when rehydration is complete.2 13 40 Children require their normal maintenance fluid, and this can be calculated from body weight. A useful method is to provide 100 ml/kg/day for the first 10 kg of body weight, 50 ml/kg/day for the next 10 kg, and 25 ml/kg/day thereafter.2 In practice, fluids are offered ad libitum and in almost all cases children will meet or exceed such calculated “maintenance requirements”. Maintenance fluids can be given as breast milk, formula, or other fluids appropriate for age.
In addition to maintenance requirement, however, continuing losses due to persistent diarrhoea or vomiting should be replaced with extra feeds of ORS. One strategy is to alternate freely normal feeds with ORS feeds.2 An alternative is to give approximately 10 ml/kg for each diarrhoeal stool passed.14
Recommendations on fluid management
-
An ORS containing sodium 60 mmol/l, glucose 90 mmol/l, potassium 20 mmol/l, and citrate 10 mmol/l with an low osmolality of 240 mmol/l is safe and effective for the prevention and treatment of dehydration in European children with acute gastroenteritis [I,A]
-
In the vast majority of cases rehydration should be carried out using ORT [I,A]
-
Rehydration should normally be completed over a three to four hour period [II,B]
- (a)
- “Mild” dehydration (3–5%): 30–50 ml/kg as ORT over three to four hours
- (b)
- “Moderate” dehydration (5–10%): 50–100 ml/kg as ORT over three to four hours
- (c)
- “Severe” dehydration (10% +): 100–150 ml/kg as ORT over three to four hours
- (d)
- Reassess hydration immediately after giving the estimated deficit
-
Severe dehydration with signs of shock: 20 ml/kg boluses of normal saline intravenously [III,C]
-
When organ perfusion is restored begin ORT.
In hypernatraemic dehydration, ORT is safer than intravenous rehydration [II,B]
-
In hypernatraemic dehydration use “slow ORT”, aiming to complete rehydration over 12 hours, and monitor serum sodium to avoid a rapid reduction [III,C]
-
To prevent primary dehydration or recurrence of dehydration, allow unrestricted fluids, and in high risk cases either (a) alternate normal drinks (for example, milk or water) with ORS [III,C], or (b) give normal drinks and 10 ml/kg ORS after each watery stool [III,C].
Nutritional management
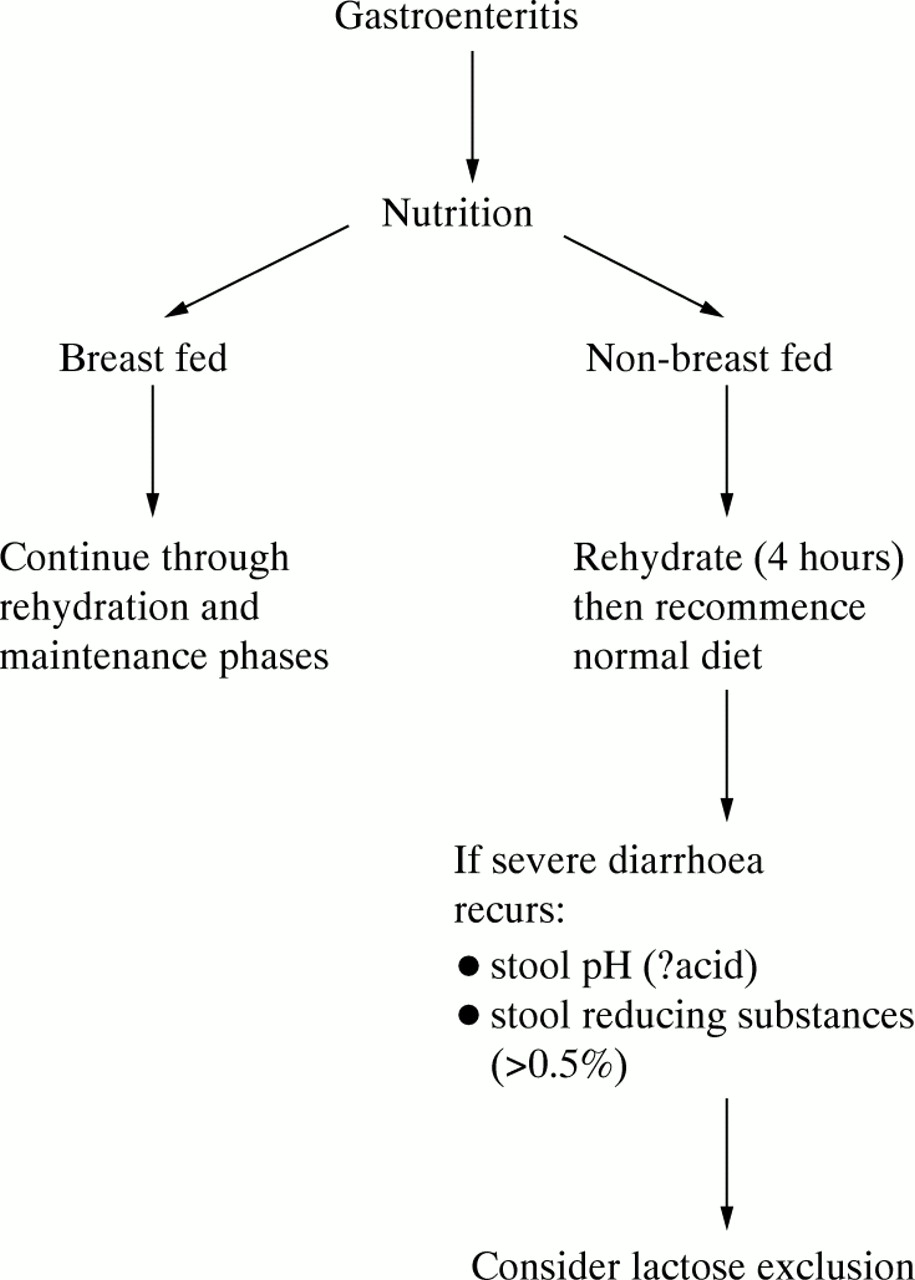
Until recently it was considered that the early reintroduction of feeds after acute gastroenteritis risked exacerbating the illness, causing protracted diarrhoea. Children were routinely starved for 24 hours or even longer.41 Evidence has now emerged, however, favouring the early reintroduction of feeds (fig 2).

{kind=link}
{kind=link}
Management of feeding in gastroenteritis.
Firstly, there is indirect evidence to support this strategy based on studies revealing the positive effects of luminal nutrition on mucosal growth and regeneration. Early refeeding was shown to reduce the abnormal increase in intestinal permeability that occurs in acute gastroenteritis.42 Increased permeability is considered to indicate a loss of mucosal integrity. Early refeeding may also enhance enterocyte regeneration, and may promote recovery of the brush border membrane disaccharidase.43 43A
Many studies have now indicated that there is no advantage to the practice of “regrading” feeds—that is, gradually increasing the feed concentration during the recovery phase after gastroenteritis.44-49 In malnourished children, early refeeding has been associated with significant nutritional advantages.50 In a recent multicentre European study, 230 weaned children < 3 years of age with acute gastroenteritis were randomly assigned to “early refeeding” or “late refeeding”.51 These children were not generally malnourished before the onset of their illness. Oral rehydration was carried out over four hours. The “early refeeding” group then received a normal diet without further delay. The “late refeeding” group received maintenance ORS for a further 20 hours, and then restarted a normal diet. Both groups were offered ORS 10 ml/kg after each watery stool. Breast fed infants continued to feed during the rehydration and maintenance phases. There was no difference between the two groups in the incidence of vomiting or watery stools on days 1 to 5, and weight gain was similar in both groups on days 5 and 14.
Transient lactase deficiency is common, particularly after rotavirus gastroenteritis. Occasionally it persists, and lactose intolerance may be a cause of post-gastroenteritis diarrhoea.52 In Europe this appears to have become a rather uncommon clinical problem.53 Moreover, a meta-analysis of clinical trials has indicated that a lactose free diet is rarely necessary after acute gastroenteritis.54 In a case-control study of Bangladeshi children < 3 years, multivariate analysis using a logistic regression model showed that discontinuation of breast feeding during the illness was associated with a fivefold increase in the incidence of dehydration.5 There is some evidence that continued breast feeding may actually reduce stool output.56
Based on these studies, ESPGAN recently issued guidelines with regard to feeding in childhood gastroenteritis.57 The recommendations were for oral rehydration over a period of three to four hours, followed by immediate reintroduction of normal feeds thereafter. It was also recommended that breast feeding should be continued throughout the rehydration and maintenance phases of treatment. It was considered that lactose free formulas were rarely necessary. Although persistent lactose intolerance is now uncommon, it was suggested that if persistent diarrhea occurred after the reintroduction of milk, stool pH and stool reducing substances should be measured, and a lactose free formula should be considered if the stool was acid and contained more than 0.5% reducing substances.43A
Recently we reported a series of infants in whom the administration of a glucose polymer formula resulted in severe protracted diarrhoea.58 These infants were eventually found to have congenital sucrase-isomaltase deficiency. Unfortunately, in such cases the diarrhoea is likely to be attributed to post-gastroenteritis syndrome. Congenital sucrase-isomaltase deficiency is not rare, and the inability of these infants to digest glucose polymer had not previously been appreciated.59
Recommendations on nutritional management
-
Breast feeding should continue through rehydration and maintenance phases of treatment [II,C]
-
Formula feeds should be restarted after completion of rehydration [I,A]
-
If there is persistent diarrhoea after reintroduction of feeds, evidence for lactose intolerance should be sought. If the stool pH is acid and contains more than 0.5% reducing substances a lactose free formula should be considered [III,C].
Pharmacotherapy
ANTIDIARRHOEAL AGENTS
In the past antidiarrhoeal drugs were often employed in the treatment of acute gastroenteritis, but with little evidence of benefit.60 Bismuth subsalicylate has antisecretory and bactericidal properties, and it may have some effect on the clinical symptoms.61 There is no evidence that other agents such as cholestyramine, loperamide, kaolin, pectin, and diphenoxylate have an effect.62-65 Nowadays, none of these drugs is considered to have a role in the treatment of gastroenteritis in children, and it is possible that their use may have adverse consequences.60
ANTIMICROBIAL AGENTS
Although C jejuni gastroenteritis is often a mild and self limiting illness, one randomised controlled trial indicated that if erythromycin was started at first presentation, before stool culture results were available, the clinical course of the illness was shortened.66 Several other randomised trials in which erythromycin was started after isolation of the organism showed a shortened period of bacterial excretion, but no effect on the clinical course of the illness.67 68 A single randomised controlled trial of treatment in children with Y enterocolitica using trimethoprim/sulfamethoxazole failed to show any useful benefit.69 The role of antibiotics in the treatment of E coli associated acute gastroenteritis in the UK is unclear.70 Non-typhoidal salmonella gastroenteritis is usually self limiting, and studies have failed to show any benefit from antibiotic treatment.70 In one study, ampicillin or amoxycillin treatment appeared to be associated with prolonged salmonella excretion in children.70 It has been suggested that antibiotic treatment may be indicated in the very young, in immunocompromised patients, and in those who are systemically ill.70 There is clear evidence that antibiotic treatment is worthwhile in patients with shigella dysentery, in whom it shortens the clinical illness and the duration of pathogen excretion.70
Recommendations regarding pharmacotherapy
-
Infants and children with gastroenteritis should not be treated with antidiarrhoeal agents [I,A]
-
Most bacterial gastroenteritis does not require or benefit from antibiotic treatment [I,A]
-
Antibiotic treatment may be indicated for salmonella gastroenteritis in the very young, in immunocompromised patients, and in those who are systemically ill [III,C]
-
Patients with shigella dysentery should receive antibiotic treatment [I,A].
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 43A.
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵