Article Text

Statistics from Altmetric.com
In order to give the best care to patients and families, paediatricians need to integrate the highest quality scientific evidence with clinical expertise and the opinions of the family.1Archimedes seeks to assist practising clinicians by providing “evidence based” answers to common questions which are not at the forefront of research but are at the core of practice. In doing this, we are adapting a format which has been successfully developed by Kevin Macaway-Jones and the group at the Emergency Medicine Journal— “BestBets”.
A word of warning. The topic summaries are not systematic reviews, through they are as exhaustive as a practising clinician can produce. They make no attempt to statistically aggregate the data, nor search the grey, unpublished literature. What Archimedes offers are practical, best evidence based answers to practical, clinical questions.
The format of Archimedes may be familiar. A description of the clinical setting is followed by a structured clinical question. (These aid in focussing the mind, assisting searching,2 and gaining answers3.) A brief report of the search used follows—this has been performed in a hierarchical way, to search for the best quality evidence to answer the question.4 A table provides a summary of the evidence and key points of the critical appraisal. For further information on critical appraisal, and the measures of effect (such as number needed to treat, NNT) books by Sackett5 and Moyer6 may help. To pull the information together, a commentary is provided. But to make it all much more accessible, a box provides the clinical bottom lines.
The electronic edition of this journal contains extra information to each of the published Archimedes topics. The papers summarised in tables are linked, by an interactive table, to more detailed appraisals of the studies. Updates to previously published topics will be available soon from the same site, with links to the original article.
Readers wishing to submit their own questions—with best evidence answers—are encouraged to review those already proposed at www.bestbets.org. If your question still hasn’t been answered, feel free to submit your summary according to the Instructions for Authors at www.archdischild.com. Three topics are covered in this issue of the journal.
Should we glue lip lacerations in children?
Is nebulised tolazoline an effective treatment for persistent pulmonary hypertension of the newborn?
How good is clinical examination at detecting a significant patent ductus arteriosus in the preterm meonate?
Likelihood ratios
In order to judge a diagnostic test, we need to know how accurately it rules in and rules out disease. There are a variety of terms to describe the test’s properties. Some may be well known (sensitivity, specificity, predictive values), others unknown (likelihood ratio).
Likelihood ratios are the most useful way of describing a diagnostic test. They are a number which tells you how many times more likely a disease is, when you get the particular test result. For example, the presence tachypnoea (respiratory rate >60) in a 2 month old child makes the odds of pneumonia eight times more likely (that is, it has a likelihood ratio of 8). A lower respiratory rate makes the odds of pneumonia about half as likely (that is, it has a likelihood ratio of 0.55).
But what is a “good” likelihood ratio, and what is a “bad” one? As a rough guide, likelihood ratios of 1–2 are almost useless at making a diagnosis, and likelihood ratios (LRs) of 1–0.5 (that is, one half) are useless at ruling out a diagnosis. A moderate test has an LR of 2–10 (or 0.5–0.1), a good test an LR of 10–50 (or 0.1–0.02), and an excellent test an LR of >50 or <0.02.
The one difficulty with likelihood ratios is the need to apply them to odds of disease, rather than the more understandable probability of disease. (Unless you want to end up in Gambler’s Anonymous, don’t even try to understand odds. Ignore them, or if you need to use them, convert them into probabilities.) There is a way out of this—using the nomogram in fig 1⇓.
(If you really want to know, you convert probabilities to odds by taking the probability (as a decimal) and call it p, and odds = p/1−p. To convert them back to probabilities, take the odd as a decimal (o) and then probability = o/1+o.)

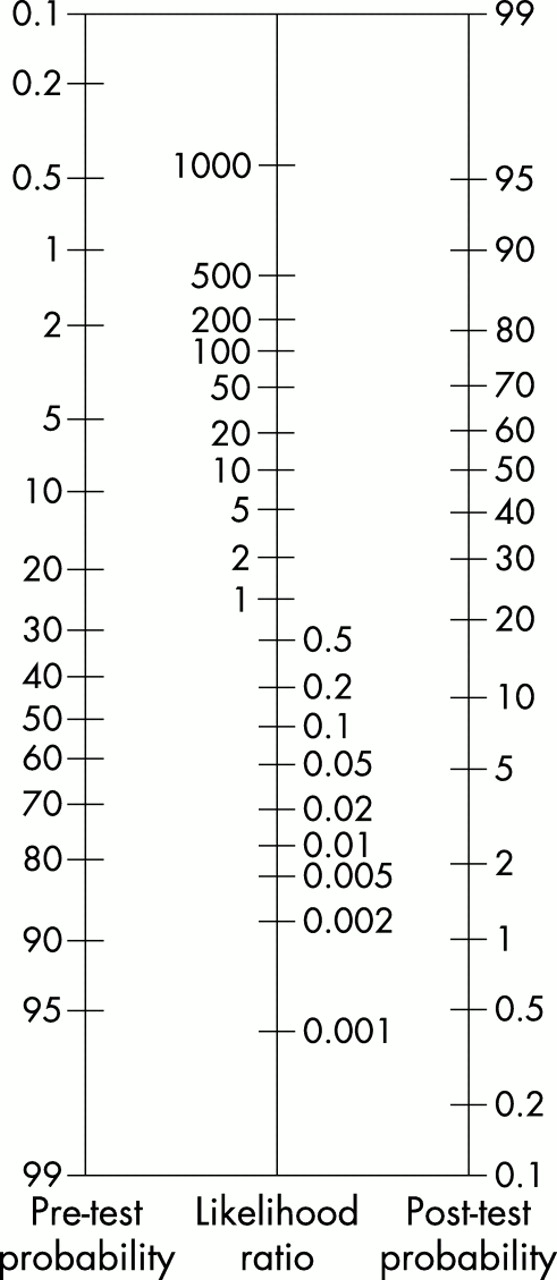{kind=link}
Nomogram for determination of likelihood ratio (from www.cebm.net).
Footnotes
Bob Phillips