Article Text

Statistics from Altmetric.com
See related article on page 10
The term failure to thrive (FTT) can imply very different conditions, depending on the context. To a general paediatrician, it might conjure up a respectably clad child, sitting on an anxious mother's lap as you study growth charts and test results in the hope of inspiration. To a social worker it might imply a wasted, miserable child found in a cold, dirty house. These differing images reflect not just the wide range of children who might receive the label “failure to thrive”, but also a diversity of ideas about what FTT is and how it should be managed. The term was first coined to describe a syndrome of delayed growth and development also called the “maternal deprivation syndrome”.1 Although it is now accepted that FTT has a predominantly nutritional cause,2the implication of an association with emotional and physical deprivation persists. However, all the early studies were of highly selected children, referred to hospital, and it is only in the past 15 years that population based studies have been conducted. What light have these studies shed on the subject and what implications do they have for practice?
Definition
FTT has been defined as “a failure of expected growth (usually weight) and well being”.3 Therefore, does this make it a problem of growth alone, or something more? A previous consensus concluded pragmatically that definitions should be growth based, because growth can be measured objectively, whereas well being cannot.4 However, even growth based definitions present problems. Many reference texts and research papers provide no objective definition, and the remainder offer a wide range of differing criteria.5 The most common definitions require cases to drop below a low centile, a method that identifies many children with poor weight gain. However, such approaches will also identify naturally small children with only minor variations in weight gain, but will miss children who drop from higher centile positions.6
In clinical practice, the diagnosis is more likely to be based on a fall down the centile chart. The problem here is knowing how much centile shift can be expected in normal infants. Infants show considerable variability in the early weeks, with 5% shifting up or down two intercentile spaces between birth and 6 weeks of age. A centile space is equivalent to the distance between two major centile lines on the UK 1990 centile charts (0.67 SD scores). Three centile spaces = 2 SD scores. From 6 weeks onwards, there is less variability, and only 5% of children will cross through two intercentile spaces between then and the age of 1 year,6and only 1% will cross three centile spaces.7 This guidance applies only to contemporary standards (UK 1990) because earlier standards show substantial variations compared with present weight gain patterns.8 An additional problem is that very large and small infants regress to the mean: 5% of children on the 98th centile will fall through three centile spaces, whereas only 1% of children on the 2nd centile will fall through two.7 If one does not allow for this, an excess number of large babies will be identified as having FTT, and very small children will be missed. For research purposes, we developed the “thrive index” to provide a linear measure of weight gain, adjusted for regression to the mean.6 For clinical application, this has been used to develop the “weight monitoring chart”, which incorporates an automatic adjustment.9 We have shown that this improves the accuracy of diagnosis, particularly in more severe cases.7 For practical purposes, the definition we have used is equivalent to a fall through two centile spaces for mild to moderate failure to thrive (slowest gaining 5%) and three centile spaces for severe (slowest gaining 1%).
In our clinical study of 97 children with mild to moderate FTT, as defined above, 90% were below the 10th centile for body mass index (BMI), and all but one showed at least some subsequent catch up weight gain.10 This implies that such children are predominantly relatively undernourished and not simply showing an unusual constitutional pattern.
Causes and correlates
Many risk factors have been identified in clinical case series, but these usually prove less clear cut in controlled studies and can disappear completely in population studies. This might be because referred populations have been selected for certain characteristics—for example, children with FTT who have oro-motor problems will be more likely to be referred to a clinic that specialises in such problems. Additional problems are posed by the varying definitions used. If a centile cut off is used there will tend to be an excess of infants with low birth weight, and apparent associations with FTT may result from confounding by risk factors for low birth weight. Finally, a comparatively rare risk factor might show an association with FTT, although explaining only a few cases. For brevity I have confined this review to the four factors most commonly mentioned: organic disease, abuse and neglect, deprivation, and undernutrition.
ORGANIC DISEASE
Despite the common emphasis on the search for underlying organic disease, major organic causes are rare. Three separate population based studies have found that 5% or less had major organic disease, mostly diagnosable from other symptoms or signs.11-13 It has also become apparent that one cannot clearly distinguishing organic from non-organic FTT, because even in the presence of organic disease the underlying cause still tends to be undernutrition.14 15
ABUSE AND NEGLECT
The role of abuse and neglect in FTT has probably been overstated. Two population studies16 17 found that only between 5% and 10% of children with FTT had been registered for abuse or neglect. However the study of Skuse and colleagues16 17 found that children with FTT were four times more likely to be abused than controls, which is in keeping with various clinical series.18-20 Therefore, children in abusing or neglecting families are probably at increased risk of FTT, but such families still only comprise a small proportion of all cases of FTT.
DEPRIVATION
Most studies of FTT have been targeted at highly deprived groups, on the unexamined assumption that deprivation plays a major role. However, one population based study, although located in an extremely deprived borough of London, reported that mothers of infants with FTT were no more deprived than local controls.11 Our population study revealed that although subnormal weight gain was twice as common in the poorest parts of Newcastle compared with more “average” areas, it was these latter, much larger areas that contributed most of the cases.21 Likewise, in our clinical study, the children screened showed very similar demographic profiles to the city as a whole.17 There is evidence that, because deprivation is widely thought to be a risk factor for FTT, this itself influences which children are referred. In a study of all children below the third centile in a baby clinic population, those diagnosed as “constitutional short stature” were just as likely to show subsequent catch up weight gain as those diagnosed as “failure to thrive”, but were much less likely to be of low socioeconomic class.22
UNDERNUTRITION
In contrast, undernutrition is strongly implicated. Most children with FTT have been found to be substantially underweight for height,11 17 23 24 although the degree of underweight is not always obvious, even to experienced clinicians.25In our clinical study,26 26A moderate to strong evidence of undernutrition was eventually found in two thirds of the children, based on a combination of history, weight gain patterns, and food diaries.
It might seem puzzling that a healthy child in a loving affluent home can become undernourished. This is less so when one recognises the high energy needs of infants: approximately three times those of adults (for each kg body weight).27 Our studies,12 13and others,11 28 have found that the fastest decline in weight gain occurs in the early weeks of life (fig 1), when energy needs are highest and the highest proportion is required for growth. At that time, early weight faltering may result from any combination of factors that limits or interrupts intake. Catch up growth may then not occur for some time, if subsequent intake is merely sufficient for immediate needs. A wide range and combination of factors may contribute to either the decline or the failure to catch up. For example, we have found that at the age of 14 months, children with FTT have a relatively delayed progression on to solid foods, poorer appetites, and eat a more narrow range of foods.17
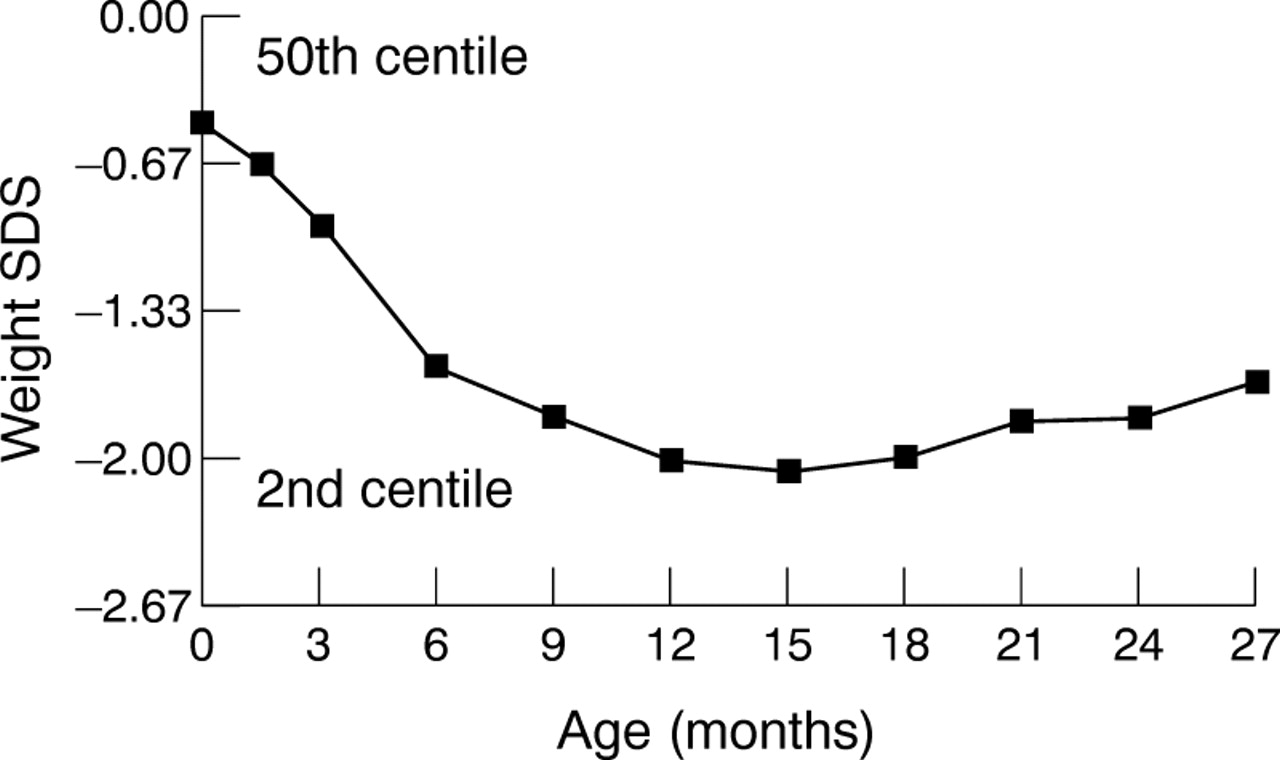
Mean weight standard deviation score (SDS) over time of 97 children with failure to thrive identified by population screening.
Consequences
GROWTH
The natural history of FTT is gradual improvement over the preschool years, but with a lasting deficit. A Swedish study of 34 children with FTT29 found that by the age of 4 years the mean weight had risen from around the second centile to nearer the ninth. In our treatment trial, which followed up 229 children to the age of 3–4 years, very similar results were seen in the untreated group, whereas the treated group were half a centile space higher.12 In the follow up of our population study, 107 children with FTT were followed up at the age of 8–9 years and were found to be three quarters of a centile space (5 cm) shorter than controls, with the average BMI more than one centile space lower.13 This persisting underweight suggests that such children go on to under eat chronically. It could be argued that this is an inherent characteristic of appetite, except that in our treatment trial, the intervention significantly improved children's reported appetites as well as their growth.12
COGNITION
Although the growth consequences of FTT seem to be enduring there is now more reassuring evidence about its impact on cognition. Significant developmental deficits of between 7 and 10 developmental quotient (DQ) points have been found at the age of 1 year in two well conducted population based studies each of approximately 50 children with FTT.11 30 However, when followed up to the age of 6 years, no significant difference in IQ was found.31 In our larger follow up study of 107 children with FTT a small non-significant difference in IQ was seen at the later age of 8–9 years.13 In contrast, a small (n = 23) early study of stunted 4 year olds found a startling 20 point DQ difference,32 with a persisting deficit of 12 IQ points at the age of 11.33 However, the confidence limits in this study were wide and the different selection criteria make direct comparison difficult. On the whole, therefore, the evidence suggests that although FTT probably influences development in the short term, a permanent effect on brain growth is less likely.
Management
These findings have considerable implications for management. If FTT is both more common and less sinister than thought previously, the imperative to intervene is less. However, there are long term consequences for growth, and possibly appetite, which suggest that effective intervention would be worthwhile. In common with most non-drug paediatric interventions, there have been few trials of intervention in FTT. Four controlled trials have failed to detect any difference between home based and clinic interventions,24 34-36 but all lacked the power to detect any but the largest effects. One study, using historical controls, found a significant effect of dietary advice.15Compared with little or no treatment, our randomised treatment trial found significant benefit for a health visitor led intervention,12 and a non-randomly allocated Swedish study found pronounced treatment benefits for a small number of children receiving intensive home based support. A discussion of the range of therapeutic approaches available for persistent failure to thrive has been published recently,37 but few of these have been subject to any sort of systematic trial. What follows is a description of the therapeutic approach we have arrived at over the past 10 years as a result of work with several hundred families. It is designed to be feasible in average rather than ideal service settings, although the exact approach adopted will vary with local staffing arrangements. We have developed training materials and clinical tools that are now commercially available to help establish such programmes.38
SCREENING OR CASE FINDING?
FTT does not fit many of the criteria for a screenable condition. However, it is the main condition identified by the existing programme of weight monitoring and already precipitates a large number of referrals. The recommendation agreed at the recent Coventry consensus meeting was that one should weigh less often, with more attention being paid to the weights that are collected (table 1).39Children need only be weighed at birth, at the time of their immunisations, and at surveillance checks until the age of 1 year, with only those causing clinical concern weighed thereafter. There was less consensus on whether explicit screening criteria should be applied to weight gain patterns. I would argue that these help staff to reassure the worried well and to identify all children with FTT: both our treatment trial12 and another study22 have suggested that up to one half of children with FTT are never identified. However, the unthinking application of rigid criteria might create worry and unnecessary referrals. If individual districts chose to apply standard criteria, such as a fall through two centile spaces identifying the slowest gaining 5%, it would have to be recognised that such children only constitute a high risk group who would merit closer investigation, rather than a definite diagnostic group.
Recommendations from the Coventry consensus meeting: growth monitoring in children under the age of 2 years
PRIMARY CARE MANAGEMENT
Whether identified by screening or not, FTT is common and often resolves with simple interventions. Thus, except in ill children or those with continuing weight loss, as opposed to slow or static weight gain, first line management should remain in primary care. In the UK, health visitors are ideally suited to undertake this work, with appropriate support and training, because of their statutory responsibility to families with young children. A home visit might reveal obvious dietary issues and this input alone often results in improvement.40 It is crucial that parents are told at an early stage and in simple terms that undernutrition is the likely cause, while emphasising what a common phenomenon this is. Avoiding an explicit diagnosis does not prevent parents from feeling criticised, but it may prevent them from discussing their concerns.
DIETARY ASSESSMENT
In persisting FTT, in the absence of organic symptomatology, the ideal second line of treatment is the paediatric dietician. In our experience, direct access can be negotiated, particularly if linked to clear cut referral criteria. A one off home visit, shared with the health visitor, usually proves fruitful, whereas repeat visits, particularly in a clinic setting, tend to be unrewarding (fig 2). In our clinical study, a fifth of the children showed improvement in their growth pattern immediately after dietary advice.26A
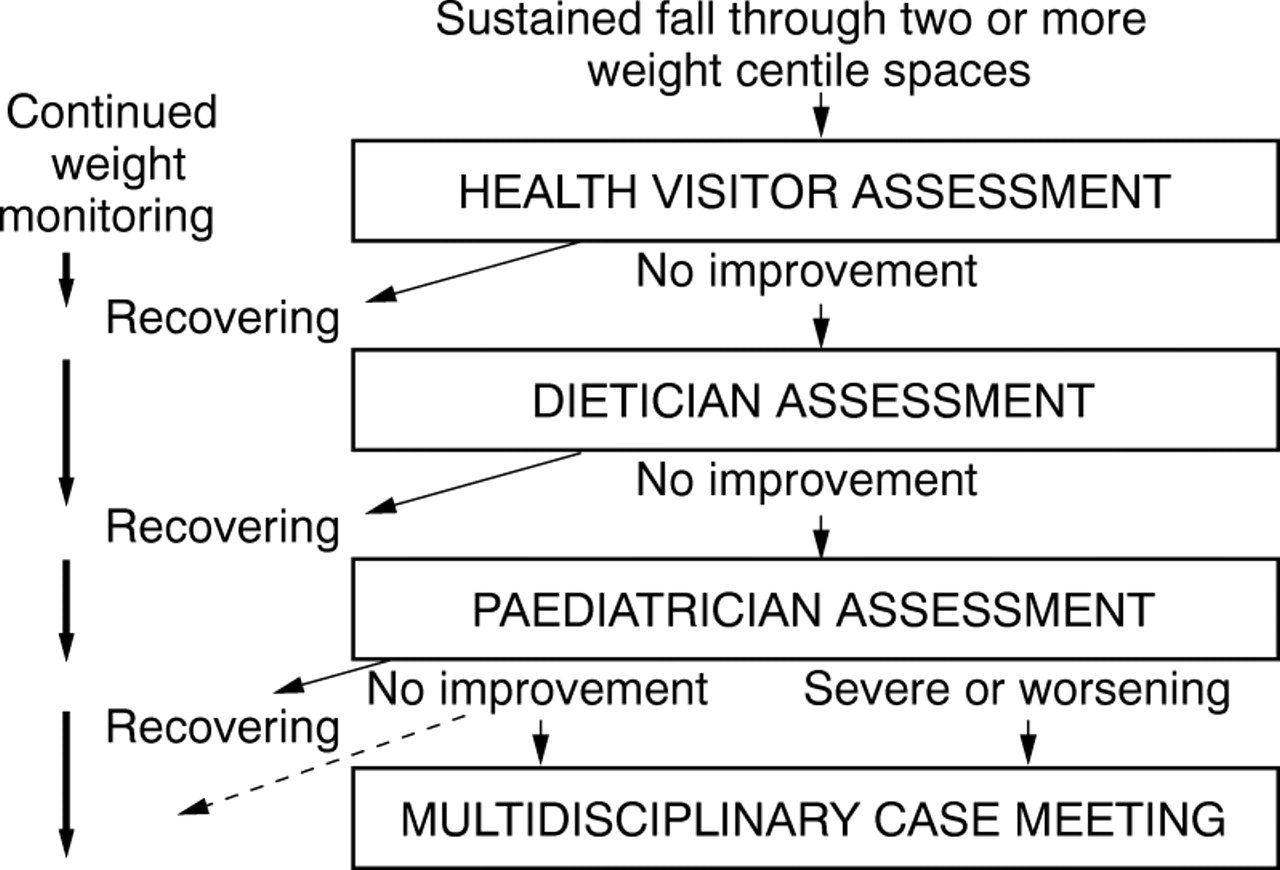
A pathway of care for failure to thrive.
The purpose of the assessment is to identify potential areas for tailored intervention, not to diagnose dietary insufficiency. The dietary history should include the child's feeding history since birth, information on the variety and frequency of foods offered and eaten, meal time routines, and drinking pattern, as well as some impression of the mother's own interest in food and cooking. Information on shopping, budgeting, and cooking equipment in the home may also be revealing. A three day food diary can be highly informative in qualitative terms but should not be relied on too heavily: it may be embroidered or even fabricated and reported dietary patterns can change rapidly in response to professional involvement, even if weight gain has not.26A
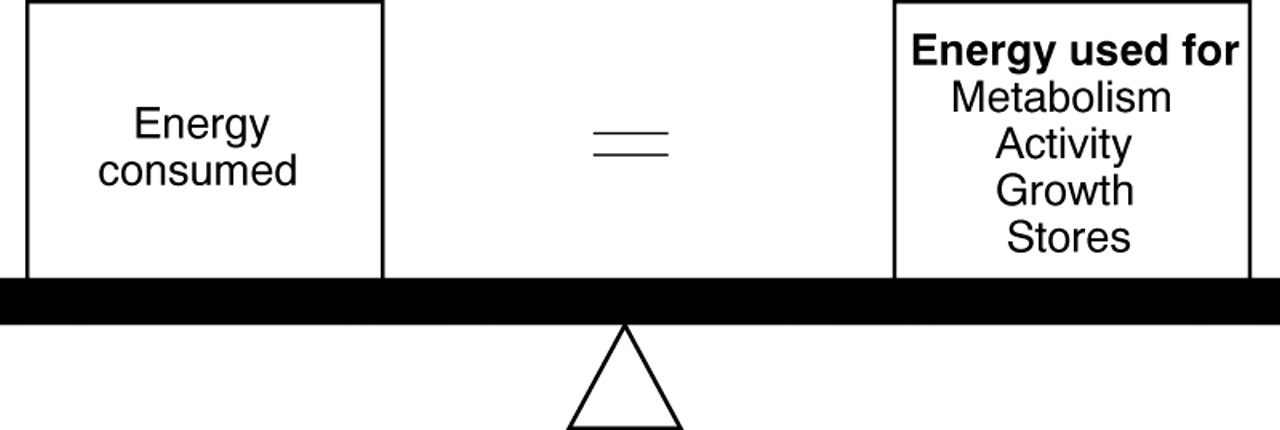
A firm grasp of the energy balance equation is essential for the successful management of FTT (fig 3). However much food a child appears to be consuming, if they are underweight for height and failing to gain weight at the expected rate, or failing to catch up, they are not consuming sufficient for their needs and advice on energy enhancement is needed. It might be helpful to remember (and to explain to parents) that children's energy requirements can vary widely, as can intake from day to day, and that a greater than average energy intake will be required for catch up growth.
{kind=link}
{kind=link}
{kind=link}
The energy balance equation.
The assessment might suggest a range of possible interventions (table2). It is sensible to decide with parents which would be most feasible or acceptable. Whatever advice is offered it should be summarised in writing, ideally in the form of a letter to the parents, with copies going to the health visitor and any other professionals involved with the family, to allow reinforcement and avoid conflicting messages.
Possible strategies for increasing energy intake
THE ROLE OF THE PAEDIATRICIAN
Arriving at a reliable diagnosis by integrating the weight gain pattern with an accurate measurement of length and parental heights usually requires the involvement of a paediatrician, although chart reviews will suffice in most cases. However, if medical causes are suspected, a consultation will be required. If investigations are undertaken they should be completed promptly, ideally at one visit. Our routine screen usually comprises full blood count and ferritin, renal, and thyroid function tests, anti-endomesial antibodies, and mid stream urine, with chromosome analysis in girls and a chestx ray and sweat test in very young infants, or where there is a history of respiratory infection. However, our experience,10 in common with others,41 42 is that laboratory investigations alone reveal no occult disease. In fact, when major organic disease was found (even potentially occult conditions such as coeliac disease) the children presented as obviously ill. Thus, most tests are undertaken to exclude pathology rather than to arrive at a diagnosis. Once this has been achieved, the paediatrician should reiterate the likely nutritional cause and ideally refer back to mainly health visitor management.
When the paediatrician is the first point of referral, having ruled out organic disease, the challenge is to engage the child's health visitor and involve her in the further assessment and management of the child, with or without the help of a dietician. This approach requires active collaboration between paediatricians, health visitors, and dieticians, but is repaid by the saving in hospital attendances,12 and the increased competence and independence of community staff.
AND IF AT FIRST YOU DON'T SUCCEED . . .
After support from the health visitor, dietary advice, and exclusion of medical conditions, there will still be children with persistent FTT. If a child is growing steadily, just two centile spaces below their expected position, no further action may be needed. However, a child with a longer fall and a more variable pattern should not be dismissed so easily. In these cases, discussion with the health visitor, ideally involving the family as well, usually reveals new possibilities, as well as offering an opportunity to reinforce earlier messages to parents.40 Nursery nurse input or nursery placement often produces steady improvement. Treatment for the mother herself, or help with related behavioural problems such as sleep disturbance, might also be helpful. In some cases there will be a need for social work input. In our experience, there is almost never a role for either food supplements or hospital admission. Toddlers with FTT often have a low intake of immature, low energy foods, with a high fluid intake. Thus, the aim of management is to expedite their progression on to more energy dense solid foods. Liquid supplements or tube feeding merely delays this, whereas hospital admission exposes children to the risk of infection and further disruption of routines. The dramatic gains that children can make at home in response to advice and support alone are often not appreciated.10
Conclusions
Research findings over the past 15 years suggest that slow weight gain is a common feature of early childhood which, although weakly associated with social or medical ills, most commonly occurs in isolation. The term “failure to thrive” tends to be seen as perjorative and many clinical staff are reluctant to make the diagnosis in otherwise “blameless” families. There is an argument for avoiding the term “failure to thrive” and relying instead on the more specific terms “slow weight gain” and “undernutrition”.
Slow weight gain does have long term consequences and appears to be amenable to community based treatment. It is important to make an objective diagnosis, recognise the likely nutritional cause, and explain this to parents, while emphasising that this is a common phenomenon at an age when energy needs are extremely high and feeding easily disrupted. We propose that a systematic approach to treatment that draws more on the skills of health visitors and dieticians, with leadership from paediatricians, will be both more effective and more supportive of parents for whom FTT is often a cause of great distress.40
Acknowledgments
None of the foregoing would have been possible without the long labours of the health visitors of Newcastle, the members of the Parkin service team, and the support of Newcastle City Health, Newcastle and Durham Universities, and the NSPCC. The programme was started by Mike Parkin before his untimely death in 1990. This work was funded by the Wellcome Trust, Henry Smith Charity, Northern and Yorkshire NHS, and Newcastle Hospitals Special Trustees.
See related article on page 10
References
Linked Articles
- Current topic