Article Text

Abstract
Objectives: This study was designed to compare the stability and comfort afforded by the long spinal board (backboard) and the vacuum mattress.
Methods: Nine volunteers wearing standardised clothing and rigid neck collars were secured on to a backboard and vacuum mattress using a standard strapping arrangement. An operating department table was used to tilt the volunteers from 45 degrees head up to 45 degrees head down, and additionally 45 degrees laterally. Movements of the head, sternum, and pubic symphysis (pelvis) from a fixed position were then recorded. The comfort level during the procedure was assessed using a 10 point numerical rating scale (NRS) where 1=no pain and 10=worst pain imaginable.
Results: The mean body movements in the head up position (23.3 v 6.66 mm), head down (40.89 v 8.33mm), and lateral tilt (18.33 v 4.26mm) were significantly greater on the backboard than on the vacuum mattress (p<0.01 for all planes of movement). Using the NRS the vacuum mattress (mean score=1.88) was significantly more comfortable than the backboard (mean score=5.22) (p<0.01).
Conclusions: In the measured planes the vacuum mattress provides significantly superior stability and comfort than a backboard.
- vacuum mattress
- spinal board
- backboard
- spinal immobilisation
Statistics from Altmetric.com
Current teaching in trauma management in the ATLS1 and APLS2 systems supports the use of the long spinal board (backboard) for spinal immobilisation, despite knowledge of pressure problems and poor immobilisation in some patient groups.3 Mountain rescue teams in the United Kingdom use the vacuum mattress predominately as it is believed to provide better overall protection of an injured casualty and is perceived to be safer and easier to transport over the terrain encountered in these situations. There are advantages and disadvantages of the two methods, both in their extrication abilities and their comfort and stability levels during subsequent transport.
This study was designed to assess the stability and comfort of the two systems.
METHOD
The study involved nine healthy volunteers. Each wore a “WizLoc” (Ferno UK Ltd, Cleckheaton, UK) rigid cervical collar and their clothing was standardised so that each wore training shoes, trousers, and a waterproof jacket. Each was placed in turn on to both the backboard and the vacuum mattress and securely strapped to the device using the recognised method for each. The backboard or vacuum mattress was then securely fixed to an operating theatre table in a manner that prevented any movement of the immobilising devices. This ensured that any movement measured occurred between the patient-vacuum mattress or patient-backboard interface.
The operating table was levelled and its position as horizontal was confirmed by use of a spirit level. Measuring arms were then secured to the side of the operating table. These took the form of rigid metal wire “arms” (fig 1⇓) that extended from the side of the volunteer in a loop to finish in a position just above the body. Three measuring arms were used. One would rest just above the volunteer’s forehead, the next just above the sternum, and the third positioned just above the pelvis. The volunteer’s midline was found and marked using adhesive dots and the measuring arm adjusted to point exactly to these.
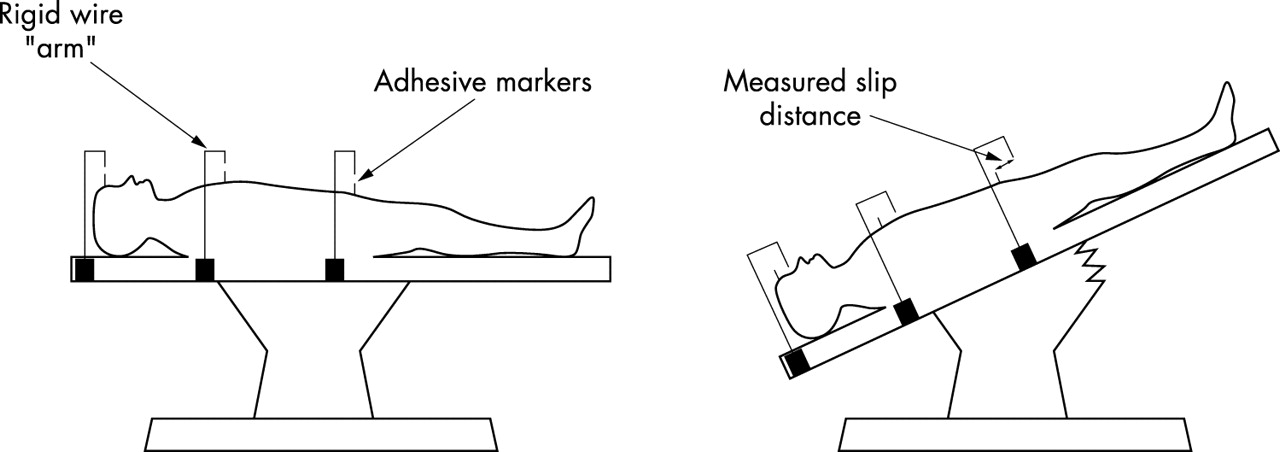
{kind=link}
Diagrammatic representation of the measuring arms showing horizontal postion (left), and measurement of pelvic movement in the head down position (right). The table was tilted at a uniform rate from +45° to −45° in two planes; head-up and head-down, laterally to the left and right. At the maximum angle the distance slipped by the volunteer within the immobilising device was measured using a steel ruler and method of no parallax. The volunteers were asked to assess the level of comfort of the two devices on a numerical rating scale (NRS) rating each between 1 and 10 where 1 was no discomfort and 10 represented the “worst pain imaginable”. Statistical analysis was performed using Student’s t test (paired two sample for means).
RESULTS
Tables 1⇓, 2⇓, 3⇓, and 4⇓ show the results.
Volunteer selection
Movement (mm)
Mean movement (mm)
Mean comfort levels
It was shown that the vacuum mattress prevents significantly more movement in the longitudinal and lateral planes when subjected to a gradual tilt. Perceived comfort levels are significantly better with the vacuum mattress than with the backboard.
DISCUSSION
Reviews on spinal immobilisation have focused mainly on the use of the long spinal board and its association with pressure injury,4 unsatisfactory immobilisation and positioning, and the pain that it can cause.5
The pressure injury problem has been looked at by Lovell in terms of the high interface pressures that develop at contact points while a casualty resides on a backboard, possibly leading to pressure sores in those who have sustained injury to the spinal cord.6 This may be compounded by peripheral vasoconstriction occurring in the wet/cold prehospital environment. The amount of time casualties remain on backboards7 (sometimes averaging more than three hours), can exascerbate the problems of pain and pressure. Ambulance journeys and waits in accident and emergency may be lengthy and there may be long distances involved in mountain rescue/prehospital transport. As a partial solution it has been recommended that the backboard should be removed as soon as possible after arrival in acident and emergency departments, ideally after the primary survey and resuscitation phases,8 while ATLS recommends removal from the backboard after two hours.1
Other studies have looked at the patient position obtained during immobilisation on a long spinal board and found it to be suboptimal. The backboard may force the neck into a relative kyphosis and in paediatric treatment, it has been demonstrated that no single method with a backboard will actually place the head in the neutral position.3 Modifying the backboard with padding may improve position and comfort,9–,11 although this is dependent upon where the padding is placed. Lerner found that a 2 cm occipital elevation placed the adult casualty in a more favourable position for cervical immobilisation. However, this did nothing to reduce the severity and incidence of occipital pain.12 Conversely for young children, a recess for the occiput or a pad to raise the chest prevents undesirable cervical flexion.
In addition to pressure injury and poor immobilisation, the backboard may be the cause of pain even in otherwise healthy volunteers, leading to unnecessary investigations/radiographs and potential ambiguity regarding the cause of the pain.4
The evidence suggests that the backboard itself is not ideal and far from a “gold standard”, and that modifying it produces equivocal results. This has led to the suggestion that the backboard “should not be the preferred surface for the transfer of patients with spinal injuries”.13
These problems have led to studies involving other splint systems. In one study seven support surfaces for the spinally injured were investigated.13 Two of these were vacuum splint devices, and other studies have compared vacuum splints and backboards in terms of the degree of stability and comfort14 afforded to the casualty, and the speed of immobilisation at the scene.15 The vacuum mattress has been shown to dramatically reduce sacral interface pressures from the potentially ischaemic levels generated with the backboard.16 In this study and in previous ones,17 the amount of movement in longitudinal and lateral tilts is significantly reduced by the vacuum mattress and it proved considerably more comfortable than the backboard. These findings may justify the conclusion that the “vacuum splint is a more effective and more comfortable alternative to the backboard for cervical spine immobilisation.”14
However, current practice (such as the APLS/ATLS formats) has not changed from the use of the long spinal board to other systems. There are many possible reasons for this.
Other systems provide superior stabilisation in only certain planes. The backboard has good longitudinal rigidity whereas the vacuum mattress will collapse if supported solely at each end, with potentially disastrous results. While this is not the recommended carrying technique it means that it may not be carried by two persons alone, limiting its use for a paramedic crew.
The speed of extrication is no different between the backboard and the vacuum mattress and the safety and ability of extrication using the vacuum mattress is poorer. The backboard’s ability to “scoop” casualties from all manner of situations (mountain crags, motor vehicle entrapments, easing patients with fracture neck of femur from armchairs)15 and then sliding them on its slippery surface, facilitates extrication. Conversely the non-uniform surface, large size (when spread out) and comparatively high friction surface of the vacuum mattress makes its use as an extrication tool more difficult.
The backboard is permanently rigid and cannot suffer catastrophic failure, such as a loss of vacuum in the vacuum mattress. This may be a problem in the mountain rescue environment with rough rocky surfaces leading to puncture of the vacuum mattress. In contrast the paramedic environment may be less arduous but the everyday use of the vacuum mattress may lead to wear and tear.
If the two systems were combined then perhaps a safer splint would develop. This could be by either extricating on the long spinal board and then placing the board with the casualty into the vacuum mattress, or by extricating the casualty onto the backboard and then log rolling off the backboard and on to the vacuum mattress.
The former is favoured by Edale Mountain Rescue team although we speculate that while more stable if tilted, the disadvantages as regards comfort and position on the backboard are still present. However, the removal of the casualty from a stabilising device with a further log roll would increase the risk of problems, especially as the log roll itself has been shown to present the greatest possibility of spinal movement for certain spinal injuries.18
What is clear from this and other studies is that no single system appears to provide the ideal for extrication and transport of a trauma casualty, but that each system has its own qualities. A combination of systems may confer benefit. However, before disregarding one system in favour of another, careful consideration should be given to the advantages and disadvantages of each, as the potential for serious injury is great. The vacuum mattress provides a solution to some of the drawbacks of the long spinal board.
REFERENCES
Linked Articles
- Primary Survey