Article Text

Abstract
AIM To determine blood glucose levels in a population of healthy, breast fed, term infants of appropriate size for gestational age.
METHODS In a cross sectional study, the blood glucose concentration of 223 healthy, breast fed, term infants of appropriate size for gestational age was determined at different times (between one and 96 hours) after delivery. One sample of blood glucose was taken from each infant independent of the feeding time. The glucose concentration was correlated with sex, method of delivery, delivery with or without analgesia, smoking status of the mother, gestational age, umbilical cord pH, and Apgar score. Infants suspected of suffering from intrapartum hypoxia were excluded.
RESULTS Blood glucose concentration one hour after delivery was not significantly lower than at any other time. Only two infants had low blood glucose concentrations one hour after delivery (1.4 and 1.9 mmol/l). There were no significant differences in blood glucose concentration between sexes, methods of delivery, infants delivered with or without analgesia, and infants born to smokers or non-smokers, and there was no further correlation between blood glucose concentration and gestational age, umbilical cord pH, or Apgar score.
DISCUSSION Very few healthy, breast fed, term infants of appropriate size for gestational age have low blood glucose levels, and there is no indication for blood glucose monitoring in these infants.
- blood
- glucose concentration
- appropriate for gestational age
- hypoglycaemia
Statistics from Altmetric.com
Glucose is a very important substrate of metabolism especially in the brain, and severe and prolonged neonatal hypoglycaemia is associated with a risk of long term neurodevelopmental sequelae.1-3 Many different neonatal groups are at risk of developing low blood glucose concentrations—for example, preterm infants, infants who are small for gestational age, and infants born to toxaemic or diabetic mothers.
In another study we found that infants exposed in utero to valproate are at risk of neonatal hypoglycaemia4, and we now recommend routine determination of blood glucose in these infants during the first few days of life. The controversy about the definition of hypoglycaemia, the large differences in its incidence, and the significance of hypoglycaemia in the neonatal period prompted us to set up this prospective study to determine the normal level of blood glucose in a population of healthy, breast fed, term infants of appropriate size for gestational age.
Materials and methods
During the period January 1996 to April 1997, we determined in a cross sectional study the blood glucose concentration of 223 infants at different times after delivery. We included healthy, term infants (259 days < gestational age < 294 days), who were of appropriate size for gestational age according to intrauterine growth curves based on ultrasonically estimated fetal weights,5 and with a one minute Apgar score of > 7 and a five minute Apgar score of 10.
We excluded infants of mothers with insulin dependent diabetes and gestational diabetes, infants with any disease or malformation, and infants suspected of suffering from asphyxia during the birth and for that reason instrumentally delivered.
The study sample consisted of 96 boys and 127 girls with a mean gestational age of 39.5 weeks and a mean birth weight of 3533 g (range 2580–4600).
The infants were delivered vaginally (n = 172), mainly without anaesthetic (n = 161), or by caesarean section (n = 51). The anaesthetics used during vaginal delivery were epidural analgesia with bupivacaine, pudendal block, and infiltration analgesia with lidocaine/adrenaline. Caesarean sections were mainly performed during spinal analgesia (with bupivacaine) (n = 41), but general analgesia (n = 6) and epidural analgesia (with bupivacaine) (n = 4) were used too.
All infants were breast fed on demand. Feeding times were not recorded, but the routine of the department was breast feeding within the first hour of life and thereafter every second or third hour.
The smoking status of the pregnant women was recorded, except in three cases; 166 were non-smokers and 54 were smokers.
None of the mothers had glucose infusion during labour or delivery and no β-agonists were used. Table 1 gives the characteristics of the patient sample.
Characteristics of the patient sample
Immediately after delivery, the infants were randomised to determination of blood glucose at one of the following times after delivery which was independent of feeding time: 1, 2, 4, 6, 12, 24, 48, 72, and 96 hours of age. The samples at 1 hour of age were taken after the first feed.
Capillary blood samples were collected by heel prick into 20 μl heparinised micropipettes containing fluoride and analysed immediately (within 10 minutes).
The study consisted of 22 infants, in which the blood glucose level of mixed arteriovenous blood of the umbilical cord was determined (0 h).
The samples were analysed by the glucose dehydrogenase photometric method6 in an Hitachi 911 analyser with an analytical standard deviation of 0.08 mmol/l both within and between series and a combined preanalytical and analytical standard deviation of 0.15 mmol/l, both within day and day to day.
Statistical analysis was by the Mann-Whitney rank sum test and Fisher's probability test. The significance level was set at 5%.
Written informed consent was obtained from the pregnant women before the onset of labour.
The protocol was approved by the local ethics committees.
Results
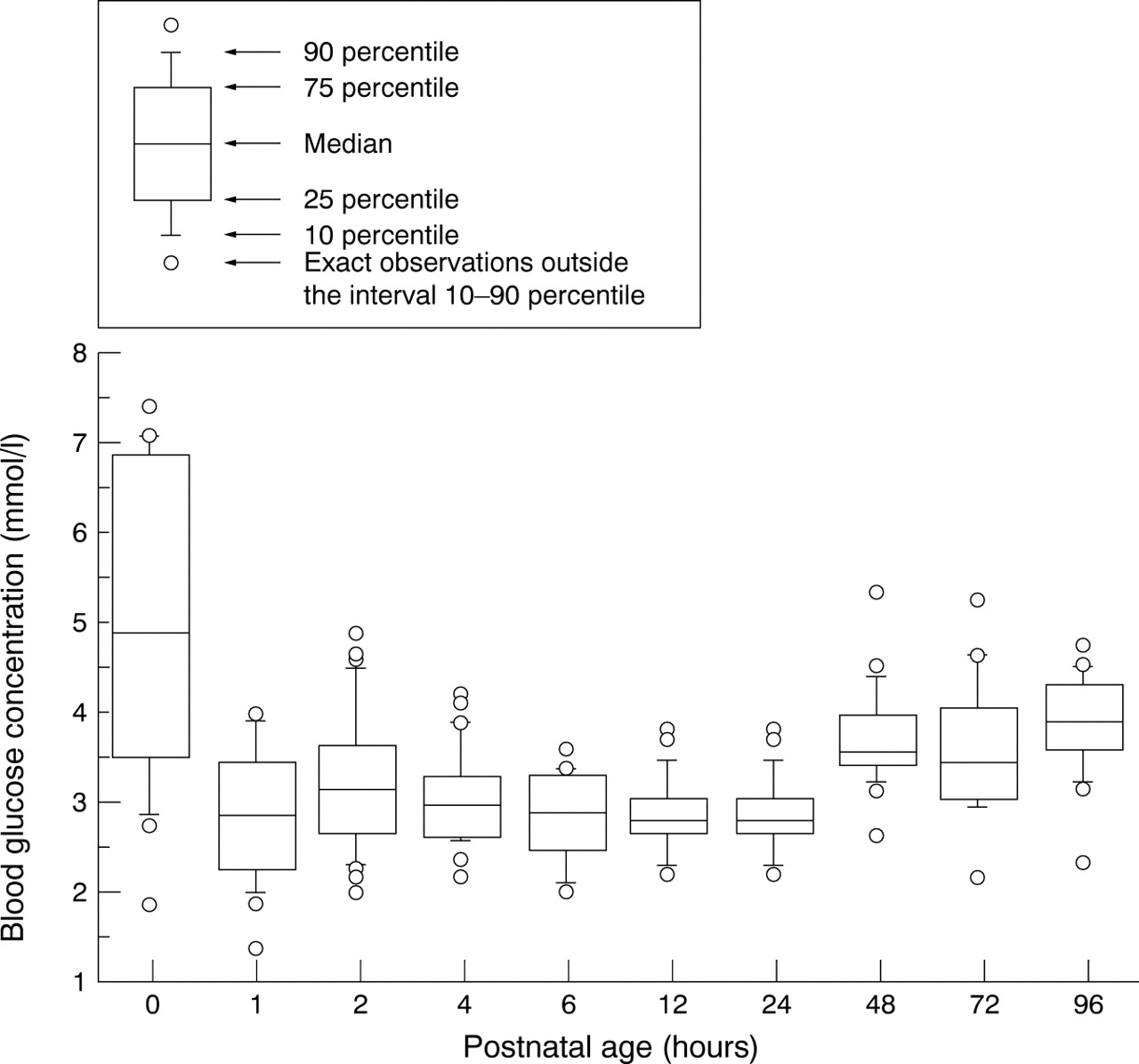
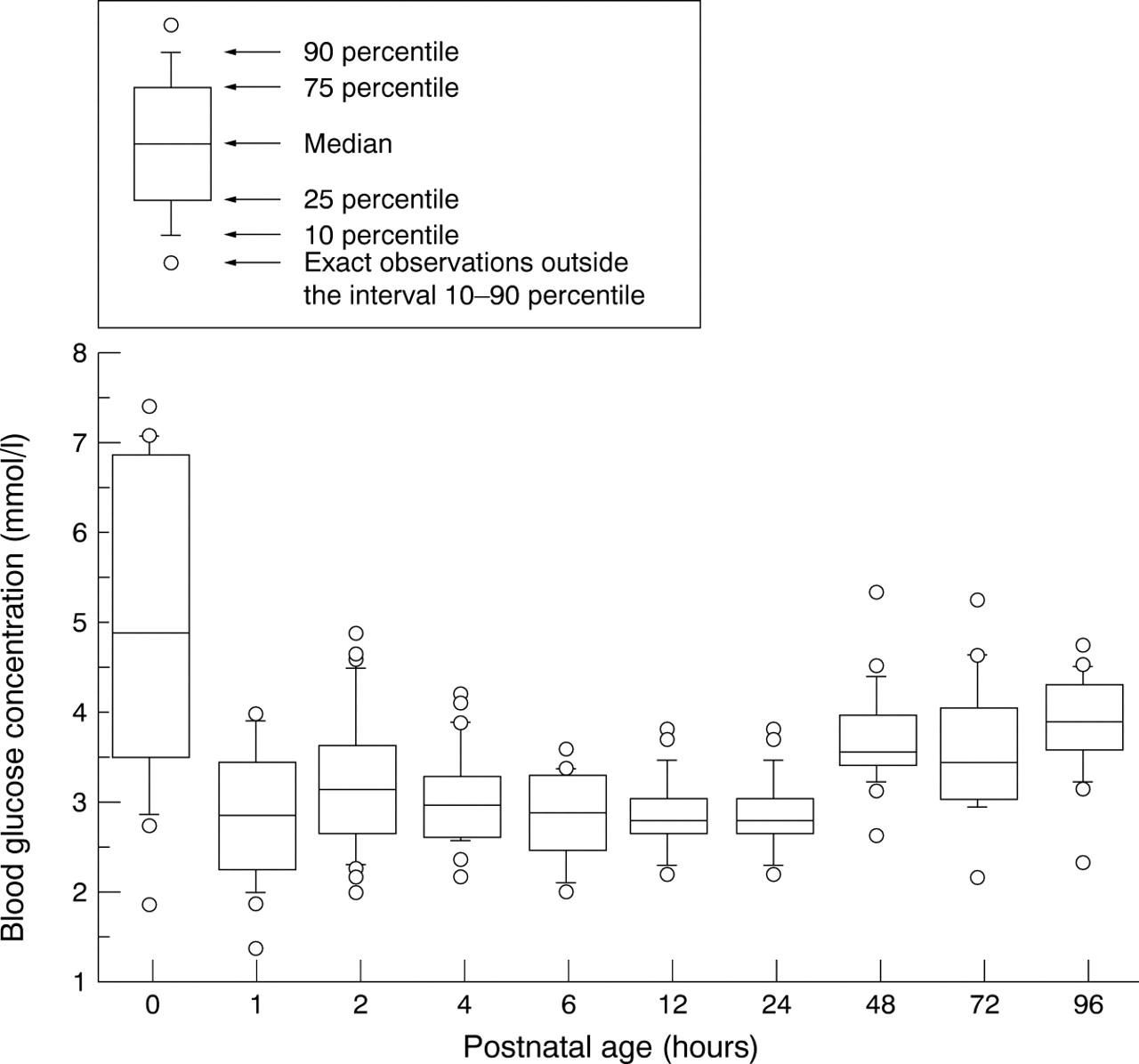
A total of 223 blood samples were taken at different times after delivery. The number of samples taken for each time point varied between 18 and 27. Figure 1 shows the variation in blood glucose concentration at each time point.
{kind=link}
Blood glucose concentration in healthy, breast fed, term infants of appropriate size for gestational age, during the first 96 hours of life. The first determination of blood glucose (zero hours) is arteriovenous and the others are capillary.
The median blood glucose concentration in the infants was 3.1 mmol/l (range 1.4–5.3). The median glucose concentration in the umbilical cord was 4.9 mmol/l (range 1.9–7.4).
The two lowest concentrations were found one hour after delivery (1.4 and 1.9 mmol/l), but the glucose concentration at this time was not significantly lower than at any other time point in the study. The two infants with a low blood glucose concentration one hour after delivery had no apparent symptoms.
Blood glucose concentrations within the first 24 hours of delivery were significantly (p < 0.001) lower (median = 3.0 mmol/l; range 1.4–4.9) than those after 24 hours (median = 3.4 mmol/l; range 2.1–5.3).
The median blood glucose concentration in the boys was 3.1 mmol/l (range 1.4–5.2) and in the girls 3.1 mmol/l (range 1.9–5.3). Vaginally delivered infants also had a median blood glucose concentration of 3.1 mmol/l (range 1.4–5.3), and those delivered by caesarean section had a median concentration of 3.2 mmol/l (range 2.0–5.2). In infants born to smokers and non-smokers, the median blood glucose concentrations were 3.2 mmol/l (range 2.0–5.2) and 3.1 mmol/l (range 1.4–5.3) respectively.
We found no significant differences in blood glucose concentration between boys and girls, between infants born to smokers and non-smokers, between infants delivered vaginally and by caesarean section, or between infants delivered without analgesia and those delivered with epidural or spinal analgesia (n = 55).
Our results showed no further correlation between blood glucose concentration and gestational age, umbilical cord pH, or Apgar score.
If we included only the values for the first 4 hours, this did not alter the results.
Discussion
Large differences in the incidence of low blood glucose concentrations in healthy term infants have been found in different studies (table 2). The aim of the present study was to determine blood glucose levels in healthy, breast fed, term infants of appropriate size for gestational age. The two lowest blood glucose concentrations, 1.4 and 1.9 mmol/l, were found one hour after delivery, but the blood glucose concentration at this time was not significantly lower than at any other time point during the study. Blood glucose concentrations within the first 24 hours of life were significantly lower than during the following days. None of the infants had clinical signs of hypoglycaemia. We found very few infants with low blood glucose concentration and this low incidence may be because breast feeding was started immediately after birth (within the first hour) or blood glucose concentrations were not measured before a feed. In other studies7-11, blood glucose concentrations were determined before a feed after the 4th hour of life.
Incidence of healthy term infants with a blood glucose concentration below certain cut offs in different studies
In the present study, all infants were breast fed. Heck and Erenberg8 found lower blood glucose concentrations in formula fed infants than in breast fed infants. The authors described it as a possible slight “rebound” hypoglycaemic effect as the intake of milk was greatest during formula feeding.
Some authors have hypothesised that a high incidence of low blood glucose concentration is to some extent caused by conduction analgesia,10 related to maternal infusion of glucose during delivery7 or even dependent on the method of delivery—that is, vaginal or by caesarean section.7 In this study, we found that there was no correlation between conduction analgesia and the development of low blood glucose concentration, and we found no statistically significant difference in incidence of low blood glucose concentration in infants delivered vaginally or by caesarean section. In contrast with Cole and Peevy,10 we found no significant differences between blood glucose concentration in male and female infants, and, in accordance with the same authors,10 we found no differences in blood glucose concentration between infants of smokers and non-smokers.
From this study, we conclude that the occurrence of low blood glucose concentrations in healthy, breast fed, term infants of appropriate size for gestational age is very rare, and screening in these infants is not indicated.