Article Text

Abstract
AIM To determine whether neurological deficits are associated with structural anomalies of the brain in very low birthweight (VLBW) infants with subsequent learning disorders but without cerebral palsy, or whether other factors, such as poor early growth, are responsible.
METHODS Eighty seven VLBW infants and eight term controls who had been examined at school between the ages of 12 and 13 years, had cranial magnetic resonance imaging (MRI) scans at 15–17 years of age.
RESULTS Thirty seven (42.5%) of the VLBW children had abnormalities reported on their scans (two porencephaly, 28 periventricular leucomalacia, 24 ventricular dilatation, and 15 thinning of the corpus callosum). No significant differences in intelligence quotient, motor clumsiness, or frequency of attention deficit / hyperactivity disorder were observed between those children with MRI lesions and those with normal scans. Quantitative measurements showed the VLBW infants had smaller brains, and a relatively smaller corpus callosum compared with controls. No association between brain measurements and school performance was observed among the VLBW infants.
CONCLUSIONS The difficulties experienced by VLBW children at school are unlikely to be the result of perinatal brain injury, but they might to be attributable to the effects of poor postnatal growth.
- very low birthweight
- learning disorder
- MRI
- periventricular leucomalacia
Statistics from Altmetric.com
The survival of very preterm infants has improved considerably in recent years, leading to an increased interest in their subsequent intellectual and functional development. Although 10–15% of survivors weighing less than 1500 g at birth have a major physical disability identified in the preschool period, most are initially perceived as normal and enter mainstream schools.1 Studies of these children have, however, shown that as many as 35% experience learning difficulties in one or more subjects, and that these difficulties are predicted by the presence of minor motor clumsiness at an earlier age.2 This clumsiness has been ascribed by some to a maturational delay, but by others to early cerebral injury. Longitudinal studies of children with motor clumsiness tend to show improvement with time, although problems persist.3Associated problems such as specific learning disabilities, attentional, and behavioural disorders become more prominent.
Early attempts to correlate brain imaging, such as cranial ultrasonography, with subsequent outcome in VLBW infants were successful for major impairments such as cerebral palsy, but not as good for minor clumsiness and learning disorders.4 5 This could be due in part to the limitations of early ultrasound scanning, or possibly the action of other early environmental factors on the child as s/he develops. More recent ultrasound studies have shown some association with more minor disorders.6
In recent years magnetic resonance imaging (MRI) has shown that it can define cerebral anatomy with a precision not previously available, and with minimal invasiveness. Such scans can identify minor structural changes related to cerebral atrophy or delayed myelination of tracts secondary to perinatal or later insults.7 Although most MRI studies on young children have concentrated on lesions and myelination defects which predict cerebral palsy and visual defects, less severe outcomes have also been studied. In children with sickle cell disease the presence of minor infarcts detected on MRI correlated well with poorer performance on the Movement ABC, a test of motor impairment.8 Differences in the sizes of the corpus callosum and of the caudate nuclei have been seen in children with attention deficit or learning disorders, but born at term.9-14 The corpus callosum is very vulnerable in sick VLBW infants, and is often the site of cystic leucomalacia or atrophy, particularly posteriorly. The role of the corpus callosum is thought to relate to interhemispheric function and coordination, allowing the two cerebral hemispheres to share learning and memory. The posterior corpus callosum has a role in visual discrimination. Its fibres comprise 11% of the supratentorial brain tissue. The caudate nuclei receive inputs from cortical regions implicated in executive functioning and attentional tasks. Damage to the structure or myelination of either may result in minor motor dysfunction, attention deficit, or learning disability.
This study was designed to test the hypothesis that poor learning, attention deficit, and minor motor deficits in VLBW infants at school were related to evidence for perinatal brain injury on cerebral MRI scans.
Methods
A cohort of 137 VLBW infants attending mainstream schools was studied in detail up to the age of 13 years.3 They had been followed up prospectively from birth, with formal examinations at school at 6 and 13 years. Detailed information was available on health and growth status, and the perinatal period. IQ was measured (Wechsler Intelligence Scale for Children III) and motor disability assessed using the Movement ABC. Learning difficulties were assessed using the Suffolk Reading Scale, the Basic Mathematics Test, and the SPAR spelling test. Teacher and student questionaries were also used. Psychiatric assessments were also performed for anxiety, fears, depression, antisocial behaviour and self esteem. Parents and teachers also completed Rutter A and B questionaries with Connor’s Hyperactivity Scale. A Child and Adolescent Psychiatric Assessment (CAPA) interview was conducted with the parent and child.14 Visual function studies of acuity, stereopsis, and contrast sensitivity were done. All these data are available on a computed database, together with extensive demographic and medical data, and have been reported in detail before.3 15 Only the IQ scores, Movement ABC scores, and the presence of attention deficit at 13 years were used in this study. Attention deficit included attention deficit disorder, hyperactivity disorder, or attention deficit/hyperactivity disorder diagnosed from the CAPA interviews. The disorders were required to be sufficient to cause functional impairment at school or socially. The Movement ABC scores were originally scored out of a total of 40, but were recalculated to facilitate comparison with similar test results performed at 6 and 8 years which were scored out of 16.
Those children living within an hour’s journey from Liverpool were invited by letter to attend for an MRI scan. Full explanations of the purpose and nature of the study were given. The subjects were between 15 and 17 years of age at the time of MRI scan. They were not paid, but travel expenses were met in full. No sedation was used. MRI brain scans were performed using a 0.5 Tesla Philips Gyroscan T5-NT scanner (Philips Medical Systems, Best, Netherlands).
The following sequences were used on all subjects: sagittal T1 weighted spin echo (TR=387, TE=20); axial T1 weighted spin echo (TR=475, TE=25); axial fluid attenuated inversion recovery (FLAIR) (TR=6000, TE=150, T1=2000); coronal T1 weighted gradient echo, volume acquisition (TR=200, TE=30, TI=13, flip angle=30); coronal T2 weighted fast spin echo (TR=3000, TE=120).
Images were viewed as film copy and on an Easivision workstation, and were reported by a paediatric radiologist (LA) who was experienced in paediatric neuroimaging, and unaware of the clinical status of the individual subjects and of the educational and psychometric test results.
Scans were reported as showing evidence of thinning of the corpus callosum (fig 1), ventricular enlargement (fig 2), periventricular leucomalacia (fig 2), porencephaly, (fig 3) or none of these. Periventricular leucomalacia was recognised by a characteristic triad of abnormalities; abnormally high signal within the periventricular white matter on T2-weighted and FLAIR images, loss of periventricular white matter, particularly in the periatrial regions, and compensatory focal ventricular enlargement adjacent to regions of abnormal signal intensity.16 Porencephaly was recognised as a well defined cavity within the brain substance, communicating with the lateral ventricle and containing fluid identical with that of cerebrospinal fluid.

Sagittal T1 weighted spin echo MR images of the brain (TR = 387 ms, TE = 20 ms): (A) normal corpus callosum; (B) noticeable thinning of corpus callosum, particularly in middle section.
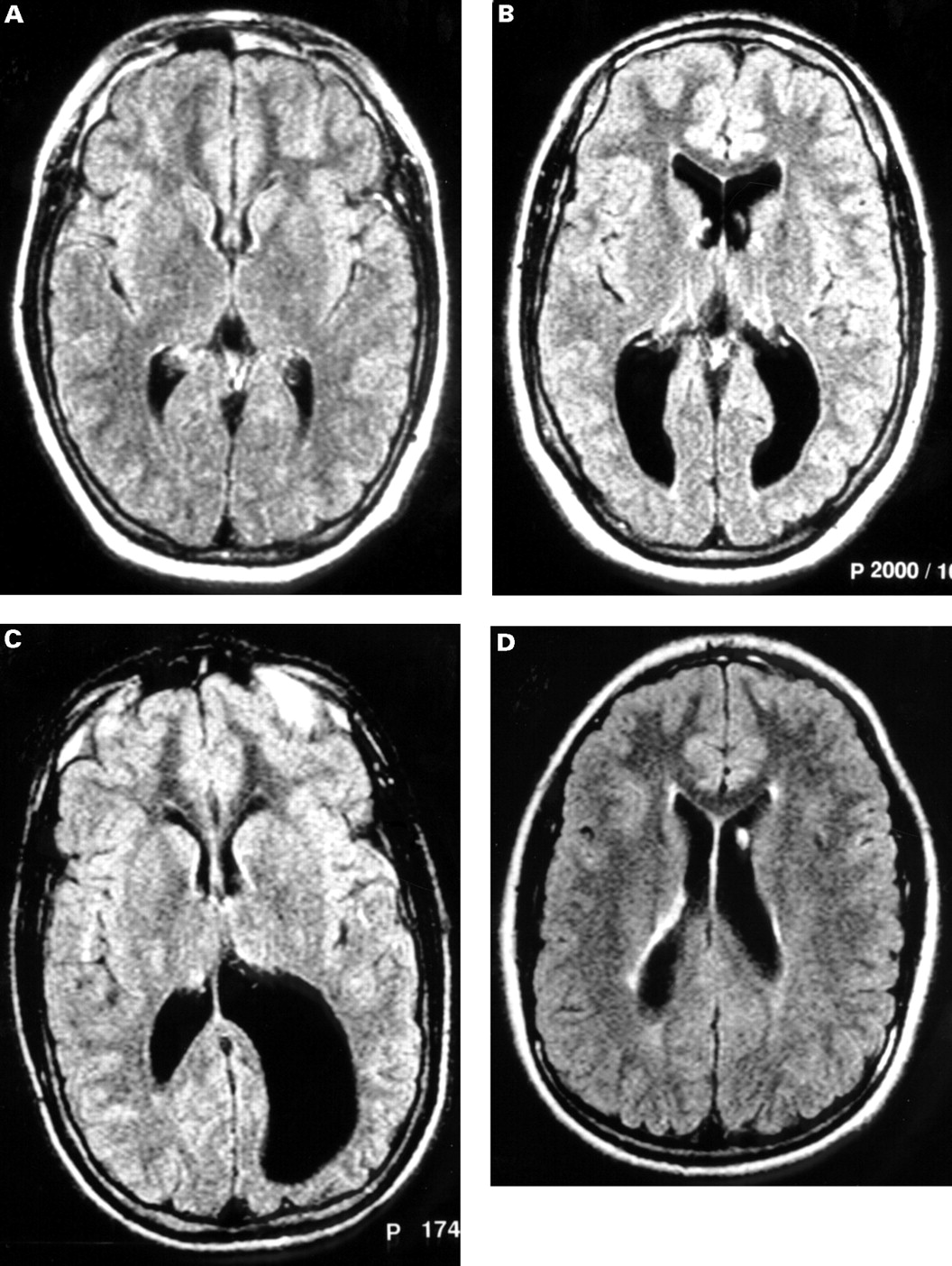
Axial fluid attenuated inversion recovery magnetic resonance images of the brain (TR= 6000 ms, TI = 20000 ms): (A) normal; (B) ventricular dilatation with loss of periventricular white matter; (C) asymmetrical dilatation of the occipital horn of the left lateral ventricle, with loss of periventricular white matter; (D) high signal within the periventricular white matter, indicating periventricular leucomalacia.

{kind=link}
{kind=link}
{kind=link}
(A) Coronal T1 weighted gradient echo MR image (TR = 200 ms, TE = 30 ms, TI = 13 ms, Flip angle of 30 degrees; (B) coronal T2 weighted fast spin echo MR image (TR = 30000 ms, TE = 120 ms). Porencephalic cyst formation adjacent to the frontal horn of the left lateral ventricle.
Measurements were made of the overall length of the corpus callosum, the cross sectional areas of the sagittal, left and right transverse and coronal sections of the brain, the cross sectional area of the corpus callosum (entire and as anterior, middle, and posterior parts), and the transverse and coronal mid cross sectional areas of the right and left caudate nuclei. The cross sectional area of the corpus callosum as a percentage of the sagittal sectional area of the brain, and the transverse and axial areas of the right and left caudate nuclei as a percentage of the transverse and axial sectional areas of the respective cerebral hemispheres, were also calculated.
The study was approved by the Regional Paediatric Research Ethics Committee.
Results
One hundred and ten children from the original cohort who lived within an hour’s journey time of the MRI centre were invited to take part in the study: 96 replied and 87 were eventually scanned. Reasons for not being scanned in those who replied included four refusals, one pregnancy, one technical failure and two who failed to attend. Twenty six of the original control children were also approached, and eight of these agreed to be scanned. A high proportion of the subjects wore dental braces, which, in some instances, interfered with the scan quality.
The 87 index children had been born at a mean gestational age of 28.6 (1.7) weeks (range 24–35 weeks) and had a mean birthweight of 1103 (203) g (range 630–1500 g). Seventeen were twins and nine were below the 10th percentile of weight for gestational age. Forty one had received antenatal steroids and eight had shown fetal distress intrapartum. There were 47 girls and 40 boys; 57 received respiratory support from 1 to 88 days; 19 had ultrasound scan evidence of periventricular haemorrhage, which in four involved the brain parenchyma, and two subsequently had minor cystic leucomalacia. Twenty two had a positive blood culture and seven frank convulsions in the neonatal period. All the control subjects (four boys and four girls) had been born at term and had had a normal perinatal period.
Thirty seven (42.5%) of the index children had one or more abnormalities reported on their scans. Twenty eight had periventricular leucomalacia of some degree, 24 had ventricular dilatation (usually asymmetrically), 15 had thinning of the corpus callosum (mainly posterior part). Two had porencephaly, but also had other abnormalities, and were not considered separately. None of the control children had any abnormalities on MRI scanning. Attention deficit/hyperactivity disorder had been observed in 19 of the scanned index children. This was similarly distributed between those with MRI abnormalities and those without. Movement ABC scores and full scale IQ scores had similar medians and ranges in those with MRI changes or none (table 1). None of the controls had ADHD, high Movement ABC scores, or low IQ scores.
The linear and cross sectional area measurements were significantly smaller in the brains of index children than in the controls (table 2). The cross sectional area of the corpus callosum was significantly smaller in index children when corrected for the smaller brain area overall (CCPCT), although the cross sectional areas of the right and left caudate nuclei were not, when treated in the same way (table 2). The ratios of right to left caudate cross sectional areas were similar in cases and controls. When all these measurements were compared in index children with and without ADHD, with a Movement ABC above and below 4, and an IQ above and below 88, no significant differences were seen for any of these measurements or ratios.
Discussion
Longer term follow up studies of infants born prematurely, but free of major neuromotor or sensory impairments, have almost invariably shown that a proportion of these children have behavioural and learning difficulties at school age.2 3 17 18 These difficulties have often been shown to occur in the presence of minor motor clumsiness or dyspraxia. The reasons for this high prevalence of problems have not been adequately explained. Social factors, poor nutrition or growth, and perinatal brain injury have all been suggested.
In the previous reports of our studies with this cohort of infants,2 3 19 class mate controls were used, who were a good match on several socioeconomic variables, yet the index children as a group performed substantially less well than the control group. Evidence for perinatal brain injury among the preterm children was clear in that 42.5% of them had MRI signs of periventricular leucomalacia, ventricular dilatation, or thinning of the corpus callosum. This figure is similar to that seen in children with overt cerebral palsy.7 However, the lack of a correlation between MRI appearances and IQ, motor coordination scores, and attention deficit/hyperactivity disorder seems to imply that another factor is more important in determining the high prevalence of these difficulties. Olsen et al 20found that 32% of a cohort of 8 year olds born prematurely had MRI evidence for periventricular leucomalacia, but that it occurred with equal frequency in those with minor motor dysfunction and in those considered to be clinically normal.
When index children and controls were examined together at 12 years, both height and head circumference were significantly correlated with IQ and ABC scores, in that poorer growth was associated with poorer scores.21 Quantitative methods applied to these MRI scans showed that the index population had smaller brains than term controls, and that the corpus callosum was significantly smaller as a percentage of brain size. Nevertheless, no significant differences were seen in the quantitative measurements when these were compared between cases with or without ADHD, motor clumsiness, or lower IQ. The absence of association between learning difficulties and measurable differences in brain MRI scans in these preterm infants differs from reported experience with term infants.9-14 This may indicate differing aetiologies for learning and minor motor problems in these two groups. For instance, in term infants the usual right/left caudate predominance is reported to be lost in ADHD, but in our cases it remained unchanged.10 Reduction in the cross sectional area of the corpus callosum in term infants has been reported in term infants with learning difficulties,9 14 but although we observed a smaller corpus callosum in the preterm infants, this did not relate to learning or motor problems. More subtle deficits undetected by MRI may be responsible for poorer performance in these children.
The period between birth and term is one of relative malnutrition for many very preterm infants, because of acute and chronic illness and poor feed tolerance. Many fall below the third percentile by term, which is the time of maximum brain growth velocity in infants, and when vulnerability is at its highest. Improvement in nutrition at this critical period may contribute to improved school performance and growth in this high risk population.
Acknowledgments
This study was supported by the Medical Research Council (Grant Number G9615155).
The data concerning qualitative MRI in this paper were presented at the Spring Meeting of The Royal College of Paediatrics and Child Health in York, 1998.
We thank Mrs G Hughes and Mrs D Garlick, Mrs J Glynn, and Mrs H Tyrer at the MRI Unit, Royal Liverpool Children’s Hospital (Alder Hey) for their skill and patience in performing the MRI scans, and the parents and children who gave their time to help in this study.
References
Commentary
Long term follow up studies of very preterm infants without cerebral palsy show a high incidence of certain patterns of cognitive impairment. Ultrasound studies have suggested that there is an association between white matter echodensities and ventricular enlargement and subsequent cognitive impairments.1-1 Cooke and Abernethy’s study, of a group of children who were born prematurely and attending mainstream schools, take these investigations further. They show MRI evidence of periventricular leucomalacia in 42.5% of the children, but no association between PVL and attention deficit disorder, low IQ, or minor motor impairment.
The authors suggest that inadequate nutrition, not hypoxia–ischaemia, may be the basis of these subsequent problems. We should also consider the effects of potentially toxic drugs such as steroids, the cessation of maternal hormones and maternal trophic factors, chronic hypoxia, abnormal environmental stimuli, and sepsis. Very preterm infants may be exposed to many or all of these factors between birth and term, a period during which there is a considerable increase in brain size and in maturation of cortical folding.
Recent studies have shown a high incidence of antenatal infection in preterm delivery, which may also lead to changes consistent with PVL—so-called “perinatal teloleucoencephalopathy”—in the developing white matter.1-2 These abnormalities reflect a more diffuse and milder abnormality than that found in PVL, but may not necessarily share the same aetiology.
Subsequent clinical impairment may result from early abnormalities in the developing brain that are difficult to detect on imaging studies performed in childhood, even with the use of quantification, as in Cooke’s and Abernethy’s study. Very preterm infants can now be serially imaged, and detail within the developing white matter, such as the presence of migrating cells, identified.1-3 1-4 In a cohort of very preterm infants subtle abnormalities within the white matter have been detected on early MRI.1-5 These changes were not typical of classic PVL, but were often associated with the development of ventricular dilatation and widening of the extra cerebral space, suggestive of brain atrophy. Interestingly, in Cooke’s and Abernethy’s study, the preterm children had significantly smaller brains than the controls.
The study was unable to confirm previous MRI findings in children born at term with attention deficit disorder, such as changes in caudate size. With current technology, there may be no neuroimaging correlate for specific learning difficulties in children who are born preterm. It would be convenient if these cognitive disorders were simply related to measurable structural abnormalities within the cortex, such as delayed folding or reduced surface area. The reality, however, is that the brain is not simply the sum of its structures. These are richly interconnected, and the quantity of connections is difficult to measure—the quality even more so.
For the time being, we remain in a situation where we are seeking not only the aetiology of the “lesion,” but also trying to locate the “lesion” itself.