Article Text

Abstract
Background: 214 orthoptists’ infants have been followed for up to 15 years, relating neonatal misalignment (NMs) and first convergence onset to later childhood ocular abnormalities. NMs are shown in a companion paper to reflect the onset of first convergence, but if frequent or absent may predict a higher risk of refractive error and esodeviation.
Methods: In a prospective postal survey, orthoptist mothers observed their own infants during the first months of life and regularly reported ocular behaviour and alignment, visual development, and any subsequent ocular abnormalities.
Results: Later strabismus and refractive error were less common in infants who showed NMs occasionally compared with those who never or frequently did. There was a significant linear trend for fewer ocular abnormalities to be found in children with more frequent NMs (p<0.001). Hypermetropes were later to show first convergence than emmetropes or myopes (p = 0.006)
Conclusions: NMs usually reflect an emerging and normally developing vergence system. This study suggests that delayed onset of convergence (and lack of NMs) is associated with later defects, especially hyperopia. Possible causal relations are discussed.
- development
- esotropia
- infants
- refractive error
- vergence
Statistics from Altmetric.com
Infants’ eyes are generally considered to be grossly aligned from birth, if careful allowance is made for the large angle lambda* of infancy.1–6 In the first weeks of life, occasional misalignments are often noticed by parents, but until the studies described below, have only been noted in passing in the literature,7–11 or have been discounted as mistaken observations.12 Until the publication of the author’s study of 1993,4 there appeared to be no studies reporting the detailed nature of these misalignments.
I have coined the term “neonatal misalignments” (NMs) to describe these fleeting, large angle, mainly convergent, ocular deviations that occur in normal infants in the first months of life. Although a few of these misalignments do persist beyond the immediate neonatal period, they are always most common in the first month of life and, in visually normal infants, dramatically reduce in frequency and duration by the second month, hence the adoption of the term “neonatal.”
The study from which the data in this paper were drawn began over 15 years ago. A group of orthoptists observed their own infants in the first weeks of life and then periodically reported details of their subsequent visual status into later childhood. Initial findings were published in 19934 and further long term follow up form data for a companion paper to this one.13 NMs were found to be common in the first weeks of life, but very variable in frequency between infants. They appear to reflect the very early exercise of the vergence system in infants. In the first month of life, it is not possible to distinguish between frequently misaligned infants who will stop squinting† and develop normal alignment and binocular single vision, and those who will develop infantile esotropia.
In 1993 there were no data to show that NMs might have any predictive value in terms of later binocular vision or refractive error, but it seemed an interesting field to explore. The study group was too small, however, to provide sufficient statistical power to detect small effects. Therefore a separate, longitudinal, cohort study of 1150 children (to be referred to as “the cohort study”) was carried out to look for such effects in a larger group of infants of lay parents.14 Infants were registered at 8–12 weeks of age as “never,” “occasionally,” or “frequently” (>15% of waking hours) squinting in the first weeks of life. The same children were then traced from preschool orthoptist vision screening records at 4 years of age. The study found subtle consequences of falling at the tails of the frequency distribution of NMs. There was a small but significant association of frequent NMs in the first 8 weeks of life with later hypermetropia and myopia, as well as with clinically significant esotropia or esophoria at 4 years of age. Never showing NMs was significantly associated with later astigmatism.
In view of the findings of this larger cohort study,14 the original orthoptists infants’ data have been re-examined to look for any subtle and long term effects in the more closely observed, and now larger and older, group. This paper reports ocular abnormalities that have developed in these children (“the orthoptists’ infants”), relating them to their neonatal data. It also compares the orthoptists’ infants study with the larger cohort study. It reports findings not expected at the outset of the study, but which have emerged over the long follow up period. The data from the orthoptist mothers are likely to give a very reliable estimate of neonatal alignment, since orthoptists are specifically trained to spot intermittent deviations and to differentiate true from pseudo-strabismus.
METHODS
Neonatal data collection is described in detail in the companion paper and in Horwood.4 Briefly, orthoptist mothers filled in a questionnaire about their infants’ ocular behaviour at regular intervals (1 and 2 weeks, 1–6, and 12 months). They reported the nature and frequency of periods of misalignment, as well as performing basic orthoptic tests of fixation, smooth pursuit, convergence, and alignment. Convergence was defined as the ability to converge appropriately to an approaching target. This was similar to the “first vergence” assessed by Thorn et al,3,15 and did not specify a specific near point or quality of movement. The target was whatever the mothers found most successful, generally the mother’s face.
At 3.5 and 5 years of age, details of binocular vision and acuity development of all children remaining in the study were collected. In 2000 a final questionnaire was sent to as many parents of children over 6 years of age as could be traced. All children reported here have been followed for at least 6 years, and some for up to 15 years.
Any referable abnormalities were reported in detail. The same criteria for abnormality used in the larger cohort study14 were adopted so that the studies could be compared. “Ocular abnormality” included all heterotropias, esophorias >6 Δ base out, exophorias >8 Δ base out if symptom producing or >12 Δ base out if non-symptom producing, motility disturbances and the prescription of spectacles over plus or minus 1.00DS/DC.
χ2 Tests were used to analyse the significance of incidence of abnormalities between groups. Where expected cell counts were less than five, the normal χ2 test is unreliable, so Fisher’s exact test was used. t Tests, analysis of variance (ANOVA) with Tukey’s post hoc tests were used for linear data.
RESULTS
Of the 215 infants who were observed until 3 months of age, 98 were still in the study at 3.5 years and 66 at 6.0 years. Thirteen additional children who had been lost to follow up between 1 and 5 years responded to reminders at 6 years (none had ocular abnormalities). Eighteen children are now over 10 years of age. Abnormalities reported are illustrated in Table 1. Longer follow up is unlikely to produce more abnormalities, except for the case of later onset acquired myopia, as few emerge over the age of 6 years.
Diagnoses of children with referable abnormalities. Cells not mutually exclusive
Sixteen children have proved sufficiently hypermetropic to require spectacles; 10 are myopic and 12 have a heterotropia or significant heterophoria.
Abnormality related to first vergence
Children who went on to develop a refractive error or strabismus were highly significantly more likely to be late to converge (mean age of first convergence: “normals” 3.5 weeks, “abnormals” 6.6 weeks, t = 3.01, p = 0.002). When broken down by abnormality, one way ANOVA results were highly significant (F5=4.36, p=0.0008). Tukey’s post hoc testing showed that it was the hypermetropes who were significantly later to converge (8.3 weeks) (p=0.006) in comparison with the normals (3.9 weeks) or myopes (3.2 weeks) (Fig 1).
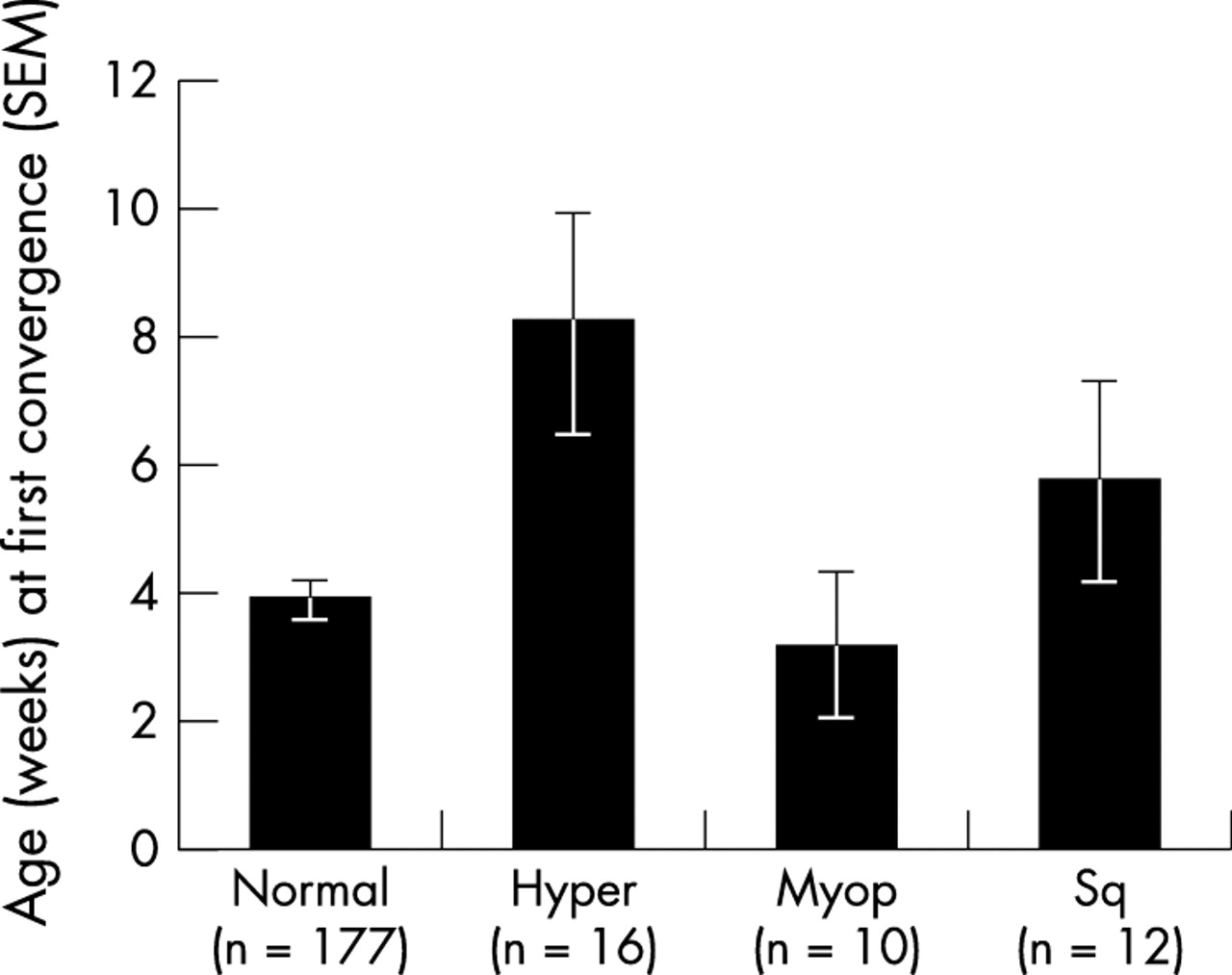
Age at first convergence broken down by ocular abnormality. Hyper = hyperopia; myop = myopia; sq = strabismus.
Because these infants were not refracted in infancy it is not possible to tell if the refractive errors were present at birth or developed later. Later true strabismus was not statistically associated with age at first convergence (5.7 weeks) (p=0.71). The small numbers of strabismic children made it impossible to investigate whether possible significant differences existed between eso/exo, accommodative/non-accommodative, or constant /intermittent deviations.
Abnormality related to NMs
In the previously published cohort study,14 frequency of NM had been divided into “never”, “occasional”(<15% of waking hours), and “often” (>15% of waking hours). If the same broad categorisation is made in this group, the proportions of defects were very similar in pattern to the cohort study with a smaller percentage of defects in the “occasional” group than either the “often” or “never” groups. Despite the similarity between these two independent groups, χ2 analysis looking for a relation between neonatal frequency group and later diagnosis, however, did not reach significance, mainly because of lack of power. (For example, if the incidence of prescribed spectacles is considered, χ2 (Fisher’s exact test) = 3.93, df 2, p=0.14.) In order to detect a small effect with a power of 0.8 a sample size of 964 would have been necessary. Such numbers were obtained in the cohort study14 (n=1150), but were not available for this unplanned retrospective analysis. There were insufficient orthoptists’ infants available in the United Kingdom and Australia where recruitment took place.
The strength of this study, however, is that much finer distinction in frequency of misalignment was possible between categories of NMs (Fig 2). It was therefore possible to determine the effect of progressively more time spent misaligned on later abnormalities. Intuitively, it might be predicted that there would be a positive relation between NM frequency and later abnormality. However, except for constant misalignment (see Discussion), there is a significant linear trend towards fewer ocular abnormalities in the children who showed more NMs (r2=0.78, p<0.001). Occasional NMs have also been shown to be associated with earlier emergence of first vergence.13

{kind=link}
{kind=link}
Percentage of abnormalities found by neonatal frequency category. Unshaded column denotes small numbers and equivocal responses excluded from analysis (see Discussion).
Two infants destined to develop true infantile esotropias were indistinguishable from the subsequently normal children in the first 2 months and did not have constant deviations in the neonatal period (see companion paper).13
DISCUSSION
The data presented suggest that occasional misalignments are associated with the lowest incidence of later refractive and motility problems. Never, or only very rarely, being misaligned, and being late to converge (reported here), as well as showing very frequent NMs (reported in the cohort study14), appear to carry more risk than the middle range of NM frequency. The larger numbers enabled the cohort study to identify the association between very frequent NMs and later refractive error and esodeviation. This study was able to make fine distinctions between groups of occasional NMs and thus to find the trend at the lower end of the NM spectrum that would have been missed in the cohort study because of methodological differences.
This retrospective analysis was not anticipated at the outset of the study in 1987 and was only carried out to look for any evidence of the trends identified by the larger cohort group in 2001. It suffers from lack of statistical power because of small numbers but the pattern of data is similar. This group of orthoptists’ infants benefited from much closer and more expert observation in the neonatal period, and longer follow up, than the cohort group. The cohort study only asked for a broad classification into “occasional” or “never” NMs, while the orthoptists were asked to put NM frequency into one of eight categories.
There appears to be a breakdown of the trend for fewer abnormalities in more frequently misaligned infants in Figure 2, which suggests that constant misalignment carries a 50% risk of abnormality. However, the data from these two infants were excluded as unreliable. Both were reported to have very small constant exodeviations, while the other 213 infants reported up to 3 months of age all had large eso or variable eso/exo deviations. As discussed by Thorn et al,3 when a cover test is impossible, it is not possible to accurately identify small exodeviations in neonates by corneal reflections because of the misleading pseudo-exotropic effects of angle lambda. Thorn et al3 and Hainline et al5 suggest that this may be the reason for the high incidence of apparent exotropia found in neonates by the group from Indianapolis.9,10 Angle lambda may be especially misleading for professionals trained to use corneal reflections as a tool. The constant, pseudo-exotropic effect would not apply in all the other neonates who were reported to have large, intermittent, overwhelmingly eso or variable eso/exo deviations. One of these apparently exotropic infants was subsequently found to have a micro-esotropia and anisometropic amblyopia, which, while not an impossible progression, seems unlikely. Even if these infants are not excluded from the analysis, it makes no appreciable difference to the significance of the results.
There is a higher percentage of ocular abnormalities in this group of orthoptists’ children than in the cohort study (18.6% of the original 215, compared with 5.9% in the cohort group14). Orthoptists may enter the profession because of a family experience of attending an orthoptist as children and so may provide a higher risk sample. Parents of children with ocular abnormalities were less likely to drop out of the study than those with visually normal children—for example, 37% of those who remained in the study at 5 years (before any reminders) showed abnormalities. The results may also reflect additional zeal of orthoptists in looking for subtle abnormalities in their children—for example, non-symptom producing exophorias, microtropias, ocular movement abnormalities, or convergence weakness. (Only those severe enough to be clinically significant were included in the analysis.) Such subtle abnormalities could have been missed in other cross sectional studies using a screening battery of tests. The inclusion of some older children with acquired myopia found during the long follow up may have also contributed to the larger percentage of problems.
The unrepresentativeness of the sample may make it impossible to make inferences about the incidence of abnormalities in the population as a whole, but does not detract from its usefulness in relation to NM behaviour. Despite a higher percentage of abnormalities than was found in the larger cohort study, the distribution of different types of abnormality is remarkably similar. Even if orthoptists’ infants do represent a higher risk group, it is still possible to study the relation of later abnormality, especially refractive error, to NM behaviour.
The cohort study reported that more infants had never squinted (44.8% in comparison with only 26.8% of the orthoptists group), while more were reported to squint fleetingly. This is not necessarily surprising because 88% of the cohort study parents had needed to be reminded to fill in and return forms. They would have been relying on a more distant memory of events at a sleep deprived time of their lives. At the time that the NMs were occurring, the lay parents may not have been specifically looking for them. Fleeting NMs might have been unnoticed or forgotten. The orthoptists, however, were reporting contemporaneously and may have had a professional interest in spotting fleeting misalignments.
NMs rarely prove to be true strabismus. The Pediatric Eye Disease Investigator Group16,17 has reported that 27% of all esotropias referred to paediatric ophthalmologists before 20 weeks resolve (average age at initial examination 97 days), especially if aged under 10 weeks and intermittent. This study of orthoptists would suggest that for most infants, intermittent misalignments are normal unless they are seen to worsen in the second month of life (for discussion see Horwood13). If parents notice a deviation worsening, or if they have been told that neonatal squinting is abnormal, they may seek professional advice, but many parents see eyes being “squinty” or “unfocused” as normal neonatal behaviour. Current national babycare advice reassures parents that this is the case.18 At present it is not possible to predict whether a frequently misaligned infant under 1 month of age will straighten or develop infantile esotropia, but data from this study published in the companion paper13 suggest that even quite frequent neonatal misalignments usually resolve.
So how could NMs, which occur maximally in the first month of life, before good acuity, cortical binocularity or active accommodation are found, predict later abnormality? NMs are usually found in normal infants and disappear, but being at the tails of the frequency distribution seems to carry an increased risk.
If NMs reflect the early exercise of vergence (as suggested in the companion paper13) then both absence, or excess, of NMs could reflect an abnormal vergence system. Occasional NMs may well be a function of an immature and healthily functioning vergence system that misjudges alignment occasionally, but rapidly corrects itself with no long term consequences. The possibility that absent and excessive NM would be associated with ocular abnormality was hypothesised at the outset of the cohort study in 1994,14 and has been supported by the combined data from the two studies. A delay in these vergence attempts (reflected by the later onset of first vergence found in hypermetropes here) could also be a significant indicator of abnormality. But what is the mechanism? Is there a causal link? Does defective vergence cause later problems, or do refractive error and primary esodeviation cause defective vergence?
Primary refractive error could result in blur, reducing the stimulus to accurate vergence (that is, refractive error causes excessive or absent NMs). Refractive errors in infancy are very common,19 but low acuity in the first weeks of life because of visual pathway limitations suggests that only very extreme refractive blur, which is rare, would cause sufficient additional image degradation to interfere with vergence control.
True strabismus does not appear to precede first vergence development. Although frequent NMs may occasionally be a precursor of true strabismus, as in the case of the two frequently, but not constantly, squinting infants who went on to develop infantile esotropia, the typical patterns of strabismus found in older infants have not been found in the neonatal period either with this study or by others.20 Cortical binocularity21 and the potential for suppression22 are also not thought to be present at this stage. It therefore seems unlikely that refractive error and strabismus in the first weeks of life cause NMs or the vergence anomalies they could represent.
If causality were in the opposite direction, it is easy to see how defective vergence could lead directly to strabismus. But how defective vergence becomes associated with refractive error, especially hypermetropia as the data presented here suggest, is less intuitively obvious. The most promising explanation is that a primary defect in vergence initially causes the extremes of the NM spectrum. Although CA/C linkages are not thought to be present in the first weeks, they do appear to be influential in slightly older infants, where monocular accommodation has been found to be significantly worse than binocular in some infants.23,24 Once vergence becomes linked to accommodation, defective vergence could then lead to poor accommodation. The subsequent frequent blur could then cause failure of emmetropisation. In other words, what initially causes NM goes on to influence refractive error and strabismus. This group was not refracted in infancy and so cannot clarify the presence or direction of any causality. Objective data from our laboratory exploring this hypothesis are in preparation.
A third possibility is that another factor—for example, genetic predisposition or a subtle neurological deficit, causes both the NMs and the later problems. Only studies that measure simultaneous refractive error, accommodation, and vergence over the first weeks of life can answer the question of which, if any, is the primary defect. From a theoretical standpoint, however, NMs may provide a useful research tool by which to explore the emergence of vergence, accommodation, and refractive error.
Occasional NMs in an infant under 4 months appear to be a reflection of an emerging vergence system. If vergence develops early, infants are initially likely to spend more of their waking hours misaligned than those who demonstrate convergence later.13 Unless the misalignments are very frequent and worsening after the first month, they are less likely to go on to have a later abnormality than those who either squint more than 15% of the time or those who are truly never seen to be misaligned. These tails of the NM distribution may constitute at-risk groups that could be targeted for closer observation.
REFERENCES
Footnotes
-
↵* Angle lambda is the angle between the pupillary axis and the line of sight formed at the centre of the pupil. A positive angle lambda causes the corneal reflection to be nasal to the pupil centre. The terms angle alpha or angle kappa are often used synonymously and are almost identical.
-
↵† “Squinting” and “NMs” denote ocular misalignment that may be unilateral or bilateral and may or may not be pathological. At this age it is not possible to differentiate those infants who will progress to show pathological strabismus from those who will subsequently develop normal binocular vision.
Linked Articles
- BJO at a glance