Article Text

Abstract
BACKGROUND/AIMS To evaluate prevalence, aetiology, prognosis, and associated neurological and ophthalmological problems in children with cortical visual impairment (CVI).
METHODS The records of 7200 outpatients seen in the paediatric ophthalmology practice over the past 15 years were reviewed in order to compile data concerning CVI. In addition, the authors devised and applied a system for grading visual recovery in order to assess prognosis.
RESULTS CVI occurred in 2.4% of all patients examined. The four most common causes of CVI were perinatal hypoxia (22%), cerebral vascular accident (14%), meningitis (12%), and acquired hypoxia (10%). Most children with CVI had associated neurological abnormalities. The most common were seizures (53%), cerebral palsy (26%) hemiparesis (12%), and hypotonia (5%). Associated ophthalmological problems were esotropia (19%), exotropia (18%), optic nerve atrophy (16%), ocular motor apraxia (15%), nystagmus (11%), and retinal disease (3%). On average, CVI patients improved by two levels as measured by the authors’ scale.
CONCLUSION The majority of children with CVI showed at least some recovery. In this group of children, CVI is often accompanied by additional ophthalmological problems and is nearly always associated with other, serious neurological abnormalities.
- cortical visual impairment
- epidemiology
- children
Statistics from Altmetric.com
Cortical visual impairment (CVI) has emerged as the leading cause of low vision in children in developed countries.1-3 Over the past 10 years, researchers have endeavoured to elucidate incidence, prevalence, aetiology, prognosis, and associated neurological and ophthalmological problems in CVI.4-7 These studies have been performed in various regions of the world, but there is a paucity of data on the epidemiology of CVI in the United States.
We therefore undertook the review of a large paediatric ophthalmology referral practice to determine the occurrence of CVI within this population. We determined the frequencies of various aetiologies of CVI and recorded neurological and ophthalmological problems association with CVI, particularly since other studies of CVI often excluded children with ophthalmological abnormalities.8-12
Our final aim was to assess visual improvement among our cohort of CVI patients. To that end, we devised a method for grading thefunctional visual perception of our CVI patients. In those patients who returned for follow up visits, we calculated the amount of improvement between visits.
Materials and methods
We reviewed the records of approximately 7200 patients who were seen from 1979 to 1994 in a large paediatric ophthalmology referral practice (WVG, CSH). At the time of the patient’s appointment, the diagnosis of “CVI” was based upon (1) vision loss in the absence of signs of anterior visual pathway disease, or (2) vision loss greatly exceeding that which would be expected, given the findings of an ocular examination. Children with nystagmus underwent an electroretinogram (ERG), and we carefully excluded all children where poor visual function could be entirely attributed to non-cortical deficits.
Evaluation of these files revealed 170 cases of CVI. Data were subsequently derived in a number of areas.
AETIOLOGY AND ASSOCIATED NEUROLOGICAL DEFICITS
The aetiology and neurological assessments were based on the historical and physical findings, as well as laboratory tests. In most cases abnormal neurological findings were obvious. However, the diagnosis of seizure and hearing loss required historical (for example, chart review) corroboration and/or verification with other healthcare providers. In cases of in utero drug exposure, the aetiology was initially presumed to be cocaine exposure, and the diagnosis of cocaine exposure was corroborated by other neurological findings known to occur in conjunction with this drug’s toxicity (small size for gestational age, prematurity, central nervous system infarction).13
ASSOCIATED OPHTHALMOLOGICAL DEFICITS
Assessment of ophthalmological problems was made by the members of this team (WVG, CSH) at the time of each patient’s appointment.
Many patients reported multiple aetiologies, neurological problems, or ophthalmological deficits. We counted each of these responses separately even though this meant counting the same patient many times. We then calculated the percentage of our population that had multiple entries for aetiology, and associated neurological and ophthalmological abnormalities.
LEVEL OF VISION
We assessed each patient’s functional vision using the following nomenclature: level 1 if the patient could only perceive light at the time of examination;level 2 if the patient could occasionally visually fixate on large objects, faces, or movement in the environment, as noted in the patient’s chart;level 3 if visual function was highly variable, but with at least some moments of good visual fixation as indicated by (1) the ability to see small objects (such as pennies or stickers), or (2) could reliably visually fixate a face;level 4 if a patient could reliably fixate on small targets and/or with visual acuity that could be measured in the range of 20/400 to 20/200; level 5 if there was good, reliable visual fixation and/or with visual acuity (at least with both eyes open), measured not better than 20/50 at the time of examination;level 6 if there was a completely normal sensory visual examination. These criteria are summarised in Table1.
Initial level of vision for the study population (n=170)
We implemented this system as a method of quantifyingfunctional vision. The assessment of vision in levels 5 and 6 included visual acuity measurement, but we included a behavioural component in the rating scale to account for the possibility of good acuity but poor cognition/verbal skills. The initial level of vision was ranked for each of the 170 CVI patients. For those patients that returned for follow up, we noted level of vision at his or her last visit. We then calculated visual improvement as expressed in levels of improvement.
PATIENT AGE
Each patient’s age was recorded in years.
HOMONYMOUS HEMIANOPSIA
We recorded the occurrence of homonymous hemianopsia in CVI patients.
Results
Review of the patient records revealed 170 cases of CVI, 2.4% of all patients seen. From these 170 patients, we were able to construct a profile for the CVI patients. The average patient age was 3 years. Initially, the average level of vision was 2.1 as measured by our scale. Thirty eight patients (22.4%) had homonymous hemianopsia in addition to CVI.
Ninety six patients returned for further evaluation (56.5% of the study population). Among those who returned, the average length of follow up was 5.9 years, with a range of 3 months to 15 years. The average change in vision was 0.9 levels as measured by our scale.
Among the study population (n=170), 154 CVI patients had known aetiologies. This represented 90.6% of the study population. Sixteen CVI patients had idiopathic onset of CVI (9.4% of the study population). Some patients reported multiple aetiologies (21 patients or 12.4%).
The most common aetiology for CVI within this population was perinatal hypoxia (22.4% of our 170 cases). Cerebral vascular accident accounted for 14.1% and meningitis/encephalitis for 12.4%. Next in frequency were acquired hypoxia (10.0%), hydrocephalus (9.4%), and prematurity (7.7%). Other less common aetiologies included intracranial cyst, 5.3%; head trauma, 4.1%; seizures, 4.1%, and brain tumour, 2.9%. In utero drug exposure (cocaine in particular) was thought to to be aetiological in 1.8% of cases. In 9.4% of cases we could not determine an aetiology for CVI. These results are summarised in Table2.
Aetiologies associated with CVI patients in the study population (n=170)
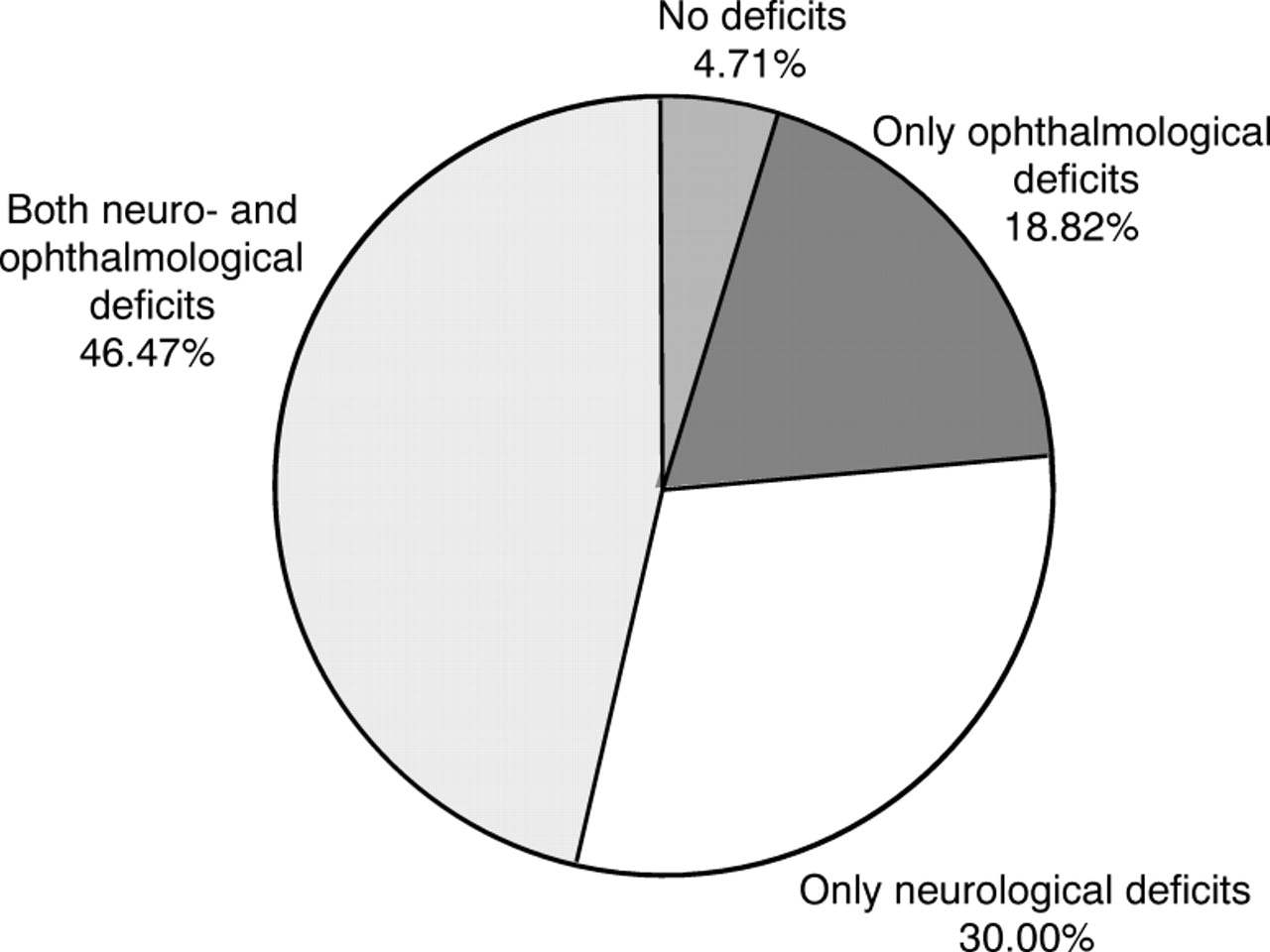
Most of our CVI patients suffered neurological and/or ophthalmological deficits. Thirty two patients had ophthalmological deficits alone (18.8%), 51 patients had neurological deficits alone (30.0%), and 79 patients had both neuro- and ophthalmological deficits (46.5%). Only eight patients (4.7%) had no associated neuro- or ophthalmological deficits (see Fig 1).

Deficits associated with CVI patients within the study population (n=170).
Seventy five per cent (n=128) of our patients had at least one associated neurological abnormality. Within this group, 50.8% (n=65) had one neurological deficit, 40.6% (n=52) had two neurological deficits, and 8.6% (n=11) had three neurological deficits.
The most common neurological deficit was seizures, with a rate of 52.9%. Most children took one or more anticonvulsants. However, other neurological problems (cerebral palsy at 25.9%, microcephaly at 15.3% hemiparesis at 11.8%, and hypotonia at 5.3%) which were initially considered separate findings, could be considered types of cerebral palsy. When all these disorders are considered together under the general heading “cerebral palsy”, the rate of cerebral palsy increases to 58.2%. The most common associated neurological deficit therefore would be best characterised as static, usually involving a perinatal brain injury.
Other less common abnormalities were hearing loss (1.8%), CN VII palsy (1.8%), and developmental regression (1.2%). One case each of amblyopia, ataxia, choreoathetosis, macrocephaly, and poor motor coordination were recorded; as a group, these associations made up 2.9% of the study population (see Table 3).
Neurological deficits associated with CVI patients
The number of associated ocular deficits was also evaluated. In all, 111 of the CVI patients (65.3%) suffered from at least one ophthalmological deficit. From among this population of patients with ophthalmological deficits, 63.1% had one ophthalmological deficit, 32.4% had two ophthalmological deficits, and 4.5% had three ophthalmological deficits.
Esotropia occurred in 18.8% of the 170 CVI cases and exotropia in 18.2%. Ocular motor apraxia, or gaze palsy, occurred in 15.3%; nystagmus occurred in 11.2%. Moderate optic nerve atrophy was present in 9.4%, and severe optic nerve atrophy in 7.1%; therefore, optic nerve atrophy affected 16.5% of the CVI population as a whole. Refractive errors (>+3.00 D or <−3.00 D sphere) were seen in 8.2% of CVI patients. Among the 170 children with CVI, 2.9% also had retinal disease. One case each of CN VI palsy and poor colour vision were reported, together accounting for 1.2% of the CVI population. Table 4 illustrates these findings.
Ophthalmological deficits associated with CVI patients
Forty three per cent of patients in the study population (n=170) had vision in the level one range; 28% had vision in the level two range; 13% had vision in the level three range, 11% had vision in the level four range, and 5% had vision in the level five range. No patients had vision in the level six range initially (see Table 1).
Because we were only able to analyse follow up data for a portion of our study population, we wanted to be sure that our follow up population was representative of the study population as a whole. Therefore, we compared the initial level of vision for the entire CVI study population (n=170) against the initial level of vision in the subset of patients that returned for follow up (n=96). More follow up patients had initial vision in the level one (44.78%v 42.9%), two (28.1%v 27.7%), and three (14.6 %v 13.5%) ranges; fewer of the follow up patients were in the level four (8.33% v11.2%) and five (4.2% v 4.7%) ranges. Therefore, the follow up patients were only slightly more visually impaired than the study population as a whole.
Within the follow up population (n=96), we recorded the final level of vision. Twenty seven per cent were rated level two, 22% were rated level three, 18% were rated level one, 18% were rated level four, 14% were rated level five, and 2% were rated level six.
Regardless of initial level of vision, 40% of the follow up population improved by one level of vision, 38% showed no improvement, 14% improved by two levels. More rarely, 5% improved by three levels, 1% improved by four levels, and 1% improved by five levels of vision (see Table 5).
Change in vision among CVI patients who returned for follow up
Overall, 60.4% of the follow up population (n=96) displayed an improvement in vision, 37.5% showed no change, and 2.1% experienced a decline in vision. Figure 2 expresses this information.

{kind=link}
{kind=link}
Overall vision outcomes for follow up population (n=96).
There was no correlation between aetiology of CVI and prognosis, but children who were diagnosed before age 3 averaged greater than one full level of improvement. Those who were more than 3 years old when they were first diagnosed averaged less than 0.5 levels of improvement.
Fewer than 16% of children with CVI ultimately attained level 5 or 6. Dramatic recoveries (greater than two levels) nearly always occurred within 6 months of injury.
Discussion
Cortical visual impairment (CVI) has emerged as the leading cause of low vision in children in developed countries.1-3 This is undoubtedly the result primarily of advances in perinatal care. The majority of children with CVI develop their problem as a result of perinatal hypoxia and ischaemia,1 5 an insult which historically had a higher mortality.7 14 Similarly, other advances in medical treatment and support have allowed children with CVI caused by meningitis, encephalitis, and head trauma to survive.1 15 Advances in perinatal care and improved survival rates of premature babies are partly responsible for the pre-eminence of CVI as a cause of low vision in children.1 14 16 In addition, advances in the management of retinopathy of prematurity and congenital cataracts have caused these conditions to drop in prevalence.1 The net effect is that a greater percentage of visually impaired children now suffer CVI.
Our analysis indicates that the vast majority of CVI patients have a known aetiology and that perinatal hypoxia/ischaemia is the most common cause. Meningitis/encephalitis and head trauma were also aetiological in our population, as has been reported elsewhere.1 15 We found that cerebral vascular accident, acquired hypoxia, and prematurity were aetiological in a few cases (Table 2).
In addition to perinatal hypoxia/ischaemia, congenital brain anomalies (intracranial cysts, microcephaly, hydrocephalus) were aetiological. Head trauma may cause transient CVI in some patients; however, our patients suffered from chronic CVI, partly due to the referral nature of the practice. Head trauma accounted for 4.1% of our CVI cases; some of these cases involved non-accidental trauma.
Meningitis and/or encephalitis accounted for 12.4% of CVI cases, indicating that these conditions can pose problems for short and long term visual function in children. Most of these children suffered a severe form of infection, with a history of sepsis, loss of consciousness and seizures at the time of initial infectious insult, followed by residual cognitive defects (for example, mental retardation, personality change). Our findings are consistent with those of others17 and emphasise the very serious problem of CVI in children with meningitis.
The finding that in utero drug exposure was linked to CVI is a new one. While a constellation of problems is seen in children who have been exposed to drugs prenatally,13 to our knowledge no one has examined the connection between CVI and prenatal exposure to drugs.
Of the 170 CVI cases we examined, 9.4% of CVI cases were idiopathic. The retrospective design of this study may be partially responsible for this finding, since there was no avenue of inquiry available to elucidate the aetiology in unclear cases. However, this finding also indicates the need for further research into mechanisms causing CVI.
The vast majority of our CVI patients had associated neuro- or ophthalmological deficits. In fact, only 4.7% of our patients had no associated deficits. This finding emphasises that CVI rarely occurs in isolation and that treatment strategies must take associated deficits into account.
A substantial number (75.3%) of children diagnosed with CVI show associated neurological deficits, many of which require ongoing management and some of which may actually interfere with visual functioning (for example, seizures, anticonvulsant therapy). The frequent occurrence (52.9%) of seizures in CVI patients is noteworthy. Seizures may interfere with cortical function, and may cause transient cortical visual impairment.1 Some children within our study population have chronic and frequently recurring seizures which could interfere with visual function. In addition, the use of anticonvulsants can occasionally interfere with visual function; changing or moderating dosages of these medicines may improve vision.1 It is possible that the use of anticonvulsants impeded some of our patients’ vision, thereby lowering our assessment of initial level of vision and visual outcome.
Our study revealed a large number of CVI patients who were afflicted with cerebral palsy, hemiparesis, hypotonia, or microcephaly (Table 3). Studies among populations afflicted with cerebral palsy have noted the occurrence of CVI.18 Clinicians should be cognizant of the special needs of children with cerebral palsy who may also suffer CVI.
Wong, in a study performed in Hong Kong, reported that 100% of congenital and 88% of acquired cases of CVI in her study had associated neurological abnormalities; cerebral palsy was present in many of these patients.4 Rogers reported that all CVI patients within his population had at least one additional pathology; cerebral palsy was frequently reported (53%).7Hydrocephalus, hearing loss, epilepsy, and learning difficulties were also reported.
A significant number (65.3%) of children within our CVI population have associated ophthalmological problems which may require management and which may affect the evaluation of the severity of CVI (that is, ocular motor apraxia). One may argue that because our patient population derived from an ophthalmology practice the association between ophthalmological problems and CVI might be artificially high. However, it seems unlikely that this association is entirely due to our study population.
Esotropia and exotropia occurred in approximately 37% of our CVI patients. Whether strabismus management affects neurodevelopmental outcome is debated,19 and worthy of future research considerations. Nystagmus, abnormal eye movements (ocular motor apraxia), and optic nerve atrophy also occurred in a high percentage of children with CVI (35% when taken together).
The presence of nystagmus in 11.1% of CVI cases was surprising since cortical insults themselves usually do not cause nystagmus. In most cases, the nystagmus was presumably caused by concurrent anterior visual pathway disease. Fielder and Evans have speculated that an intact striate cortex is necessary to generate nystagmus.20 Their hypothesis is not contradicted by our findings. It is likely that some intact striate cortex was present in all our CVI patients, since not a single patient was completely blind.
Many children (17%) showed either moderate or severe optic atrophy. The relation of optic atrophy to cortical visual impairment has been investigated.21 The optic nerves are usually resistant to hypoxia/ischaemia in the perinatal period. However, when hypoxia/ischaemia is severe, optic atrophy may occur in conjunction with severe neurological deficits. Clinicians must search carefully for optic atrophy in children with CVI, since recovery of vision will be limited, and prognosis will be poor, if this anterior visual abnormality is present.
We emphasise the importance of measuring refraction in children diagnosed as having CVI. In some cases, optical rehabilitation may be rewarding. In other cases, the diagnosis of high refractive error may lead the clinician to suspect retinal disease or systemic abnormality.
The assessment of patient vision, both initially and upon follow up, was of primary interest to us. Admittedly, our classification system for assessing visual function has shortcomings. The schema is retrospective and provides limited data on visual acuity. Children can be evaluated rapidly using our system but the evaluation depends on in office evaluation and historical data. Unfortunately, alternative tests of vision in this patient population may also have shortcomings, including behavioural and electrophysiological tests.9 10 22-29
Despite the shortcomings of our system, we found it useful in correlating visual function with the need for special vision rehabilitative services. For example, children at level 4 and below should be considered legally blind in the sense that they require special services and consideration. Therefore, they should qualify for special rehabilitative services in most geographic areas. Even children at level 5 who reliably fixate on visual targets and probably have vision of 20/50 may show cognitive visual impairment. Therefore, these children may still require some handicapped and visual services. Only at level 6 were children not in need of special handicap services. These were children who had virtually a completely normal sensory visual examination. Unfortunately, only 2.1% of our follow up population attained level six.
Overall, the majority (60.4%) of the follow up patients showed some improvement, roughly a third (37.5%) experienced no change in vision, and only 2% showed visual decline. Therefore, it is important to be optimistic with CVI patients and their parents, as has been emphasised in a multitude of studies.1 15 30
This study is based on a referral practice. Milder cases of CVI that showed improvement might not have been referred. Consequently, our prognostic findings may be overly pessimistic. Furthermore, when we compared the initial vision of the entire study population against that of the follow up population, we discovered that the follow up population had proportionally more children in the level one to three range. Therefore, the visual outcome for the smaller follow up population may be overly pessimistic. Finally, the average patient age (2.98 years) seems unexpectedly high, considering that the primary aetiology was perinatal hypoxia, perhaps indicating that children were examined in our office some time after the initial development of CVI. Nevertheless, this is the largest collection of clinical findings yet to be reported, and likely reflects the overall population of children with chronic CVI.
Note that the prognosis for recovery is better in children who suffer CVI at a very early age, even though the average age of patients seen was 3 years. Overall, most children with CVI show some vision recovery, irrespective of aetiology. Our vision assessment classification may favour vision evaluation of older children, thereby making it easier for children to show improvement as they age. More likely, neural plasticity allows vision recovery when neurological damage is incurred at an early age.
Despite the likelihood of some recovery of vision, most children with CVI (>90%) remain visually handicapped. Most children with chronic CVI require additional neurological and rehabilitative services, and a surprising number may benefit from specific intervention for ophthalmological abnormalities. The failure of these children to completely recover demonstrates that CVI is a major public health problem, one that warrants future research into diagnosis, prevention, and treatment.
Acknowledgments
Supported by National Eye Institute EY00384–01 (WVG) and by the Pacific Vision Foundation.