Article Text

Abstract
Background and objective To provide an overview of drug use in outpatient children in France, a population-based study using a national reimbursement claims database representative of 90% of the French population was conducted.
Design Cross-sectional study performed between January and December 2011 using the EGB database (Echantillon Généraliste de Bénéficiaires), a 1/97th sample of the national healthcare insurance system beneficiaries. Drug use in children <18 years old was estimated through reimbursements for prescribed drugs excluding vaccines. Prevalences of use were calculated for different levels of the Anatomical Therapeutic Chemical classification by considering as users children who had at least one reimbursement during the study period.
Results In 2011, 133 800 children were included in the study. The overall prevalence of drug use was 84% and the median number of different drugs per child was 5. Drug use was greatest in children aged <2 years. The most widely used drugs were paracetamol, systemic anti-infectives, nasal corticosteroids and decongestants, and anti-histamines. 21% children <2 years received domperidone.
Conclusions There is widespread use of medicines that are unlikely to be effective and may have significant toxicity in French children. Irrational use of medicines appears to be greatest in children aged 5 years and under.
- Pharmacology
- Epidemiology
- General Paediatrics
Statistics from Altmetric.com
What is already known on this topic?
Studies that have assessed prescription drug use behaviour in children have been conducted in only a few countries in Europe and in North America.
Antibiotic use varies considerably between countries.
What this study adds?
The prevalence of drug use in French children was high at all ages, and particularly for those aged <2 years.
Half the children received anti-infective agents.
Many medicines were used inappropriately.
Introduction
Children are often excluded from clinical trials and knowledge about efficacy and safety of drugs used in this population is scarce. Doses are often extrapolated from adult data and there is a lack of paediatric formulations, resulting in common unlicensed/off-label prescription.1 ,2 Data about the extent and patterns of drug use in children are therefore critical. Two literature reviews reveal the dearth of studies evaluating general drug use in children.3 ,4 Studies that have assessed prescription drug use in children have mainly been conducted in a few European countries (Italy, Netherlands, UK, Denmark) and in North America,5–21 and most focused on a limited number of drugs, mostly antibiotics14 ,15 and psychotropic drugs,16–18 or on a specific age group (preschool17 ,19 and schoolchildren,20 or adolescents21). Moreover, some of these studies were limited by the small sample size, or lack of representativeness as many were performed at the regional level.8–13
To our knowledge, an overall picture of prescription drug use in children in France is not available. To address this, a population-based study using a national reimbursement claims database representative of 90% of the French population was conducted.
Methods
Data source
In France, the main national healthcare insurance system universally covers approximately 90% of the whole population, independently of socioeconomic status. This study used the EGB database (Echantillon Généraliste de Bénéficiaires), which is a representative sample of the population covered by the main national healthcare insurance system; the EGB is obtained by 1/97th random sampling with stratification on age and sex.22 ,23
The EGB contains anonymous data on the sociodemographic characteristics of beneficiaries and on community claims for reimbursement of drugs (when approved for reimbursement by the health authorities). The overwhelming majority of drugs available in France is reimbursed irrespective of treatment indication or duration. When such a drug is prescribed then dispensed in a pharmacy it is automatically refunded to the beneficiary and recorded in the database. Diagnoses or indications for prescribing are not collected in the EGB, nor data on drugs that must be prescribed but are not reimbursed (eg, most third generation oral contraceptives) or on over-the-counter (OTC) dispensing. OTC drugs can be purchased without prescription but some of them, such as paracetamol (acetaminophen) or ibuprofen, can also be prescribed and in that case reimbursed and captured in the EGB.
Study design and population
A cross-sectional study was conducted between 1 January and 31 December 2011, and included all children aged <18 years on 1 January 2011 or when they were included in the EGB during the study period (including newborns). Children were excluded at the date of death or at the age of 18 years. Age was assessed on 1 January 2011 and stratified into four groups: 0–23 months, 2–5 years, 6–12 years, 13–17 years.
Data analysis
Drug use (excluding vaccines) was described according to the Anatomical Therapeutic Chemical (ATC) classification. The overall prevalence of drug use was calculated by dividing the number of children with at least one drug reimbursement during the study period by the number of children included in the study. Subsequently, prevalence of use of a specific drug class (first and second ATC levels) or drug (fifth ATC level) were calculated and the 95% CIs when relevant. The median number of different drugs per child was calculated. All parameters were further stratified by gender and age. The prevalence of drug use was compared between genders and age groups using the χ2 test; the numbers of different drugs per child were compared between genders using the Wilcoxon test and between age groups using the Kruskal-Wallis test.
In accordance with French regulations, the National Institute of Health and Medical Research was informed of the study and, ethics committee approval was not required for this observational study.
Results
Study population
In 2011, 133 800 children aged <18 years were included in the study. Among them, 5876 (4%) were born during the year. The mean (SD) duration of presence in the EGB during 2011 was 357.5 days (39.4); the median (IQR) duration was 365 days (365–365). The median age of the study population was 8 years (3–13). The male/female sex-ratio was 1.05 overall and varied from 1.04 to 1.06 according to age.
Overall drug use
In 2011, 111 936 children had at least one drug reimbursement; the prevalence of drug use was 84%. The highest prevalence was 97% in children aged <2 years and declined with increasing age (p<0.0001; table 1). Stratifying according to gender and age, a similar dynamic was found among boys and girls, although for adolescent girls drug use was higher than among boys (79% vs 72%; p<0.0001). The median number of different drugs per child was five (2–9) overall and in both genders. It was highest in those aged <2 years (n=9) and decreased with age (p<0.0001; table 1).
Overall drug use according to age
Drug use according to anatomical (first ATC level) and therapeutic (second ATC level) classes
Among the most commonly used anatomical classes, the nervous system class was the most prevalent (67%), mainly analgesics (65%; table 2). The respiratory system class ranked at the second position (58%) and most of the respiratory therapeutic classes had a high prevalence of use: nasal preparations (45%), antihistamines (31%), cough and cold preparations (21%) and drugs for obstructive airway diseases (14%). The third and fourth most frequently used anatomical classes were anti-infectives for systemic use (50%) and alimentary tract and metabolism (50%). A quarter (25%) of children had at least one reimbursement of systemic hormonal preparations, mainly corticosteroids for systemic use (24%).
Prevalence of drug use according to anatomical (first ATC level) and therapeutic (second ATC level) classes and age (per 100 children)
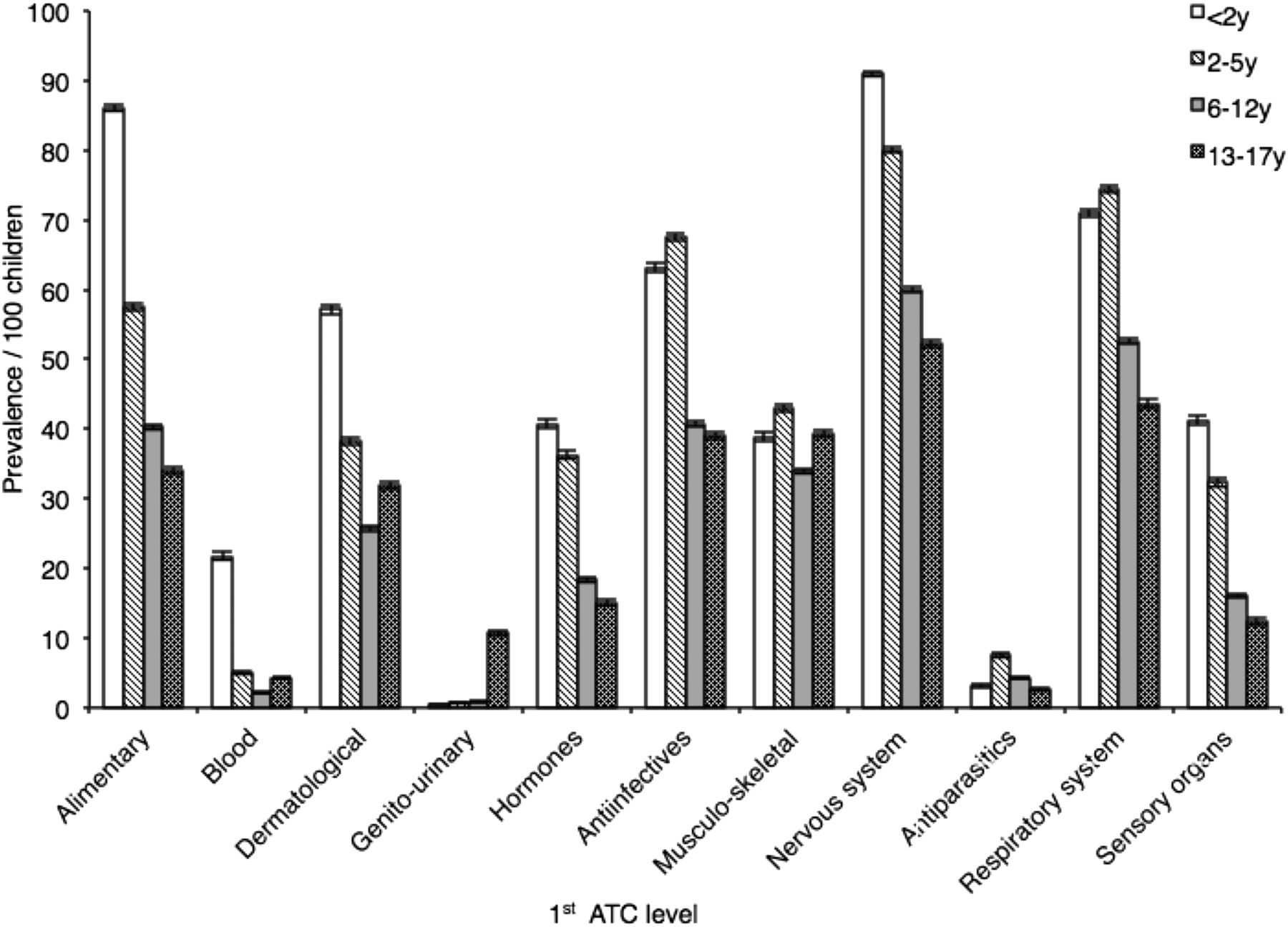
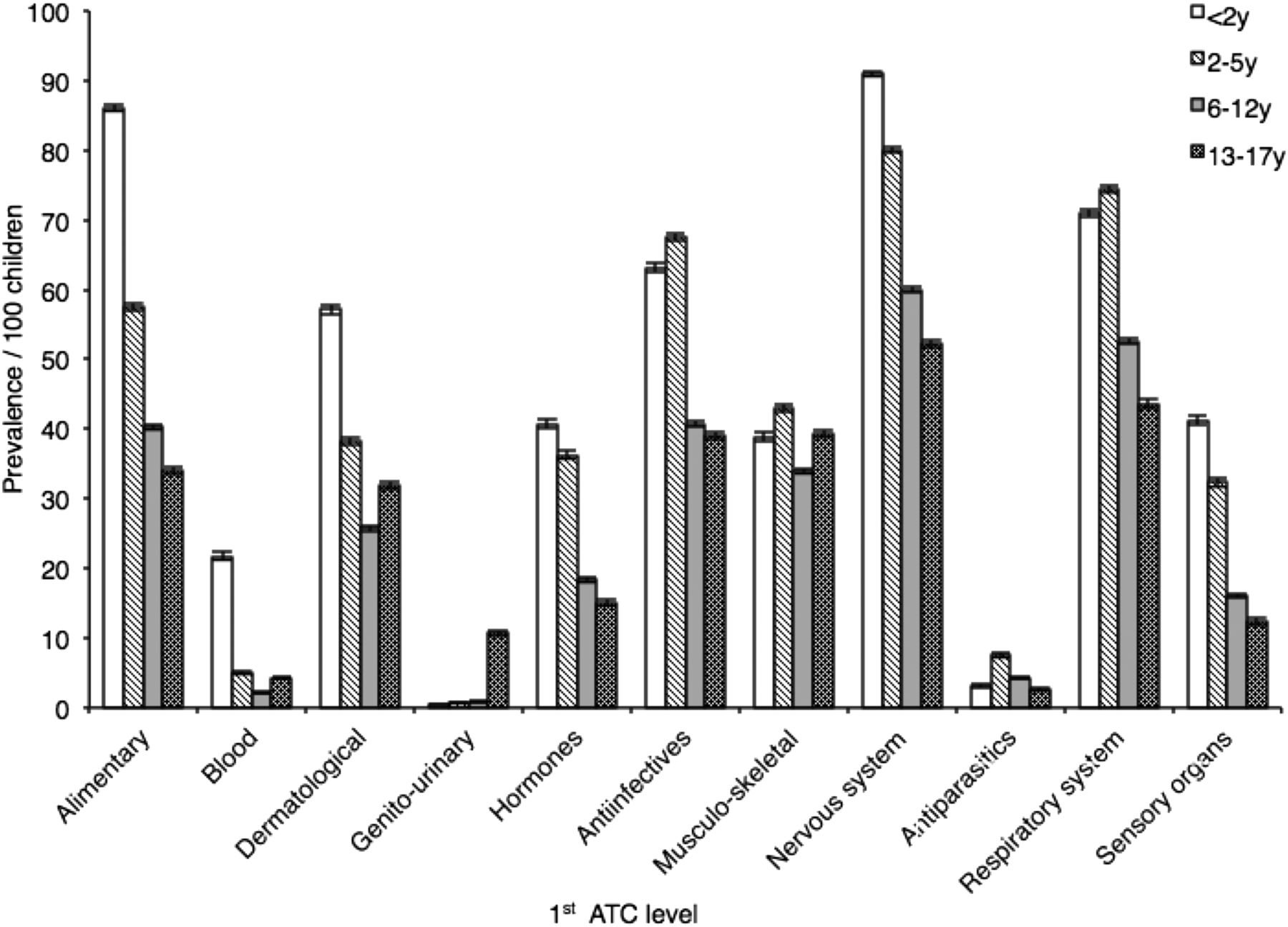
Drugs in the genitourinary system and sex hormones were more commonly used by girls than boys (6% vs 0.4%; p<0.0001), and there were no relevant differences for other drug classes. Except for the musculoskeletal system whose prevalence of use was in the same range across age groups and for the genitourinary system whose prevalence of use was higher among adolescents, the prevalence of drug use was always higher in younger children (figure 1).
{kind=link}
Prevalence of drug use according to anatomical classes (first ATC (Anatomical Therapeutic Chemical) level) and to age (per 100 children). For each anatomical class and each age group, the bar represents the prevalence of drug use (number of children with at least one drug reimbursement during the study period divided by the number of children included in the study), with 95% CI (error bars).
Most frequently used drugs
In the most commonly used anatomical class (nervous system), the most common individual drug was paracetamol followed by a local anaesthetic combination (lidocaine/prilocaine; table 3). Regardless of age, paracetamol was the most frequently used drug followed by ibuprofen. Among respiratory drugs, certain nasal preparations ranked among the most commonly used drugs: the corticosteroid tixocortol was the most prevalent, in particular among the youngest (48%); the sympathomimetic tuaminoheptane was common after 2 years of age, and the prevalence was the highest among those aged 2–5 years (18%); the antiseptic tenoic acid was also common, especially among the youngest (32%). Among antihistamines, those used for cough were particularly prevalent in children aged 2–5 years, especially oxomemazine (25%). Similarly, cough and cold preparations were frequently used in children aged 2–5 years, in particular the antitussive helicidine (24%). Salbutamol was the most commonly used antiasthmatic especially in the youngest (18%). Concerning antibiotics, the most frequently used was amoxicillin independently of age; cefpodoxime and coamoxiclav were also prevalent before 6 years of age (between 22% and 33%). No other individual antibiotic had a prevalence of use ≥10% overall and according to age. Besides cholecalciferol (19%), domperidone (12%) and phloroglucinol (11%) accounted for most of the gastrointestinal drugs used. Betamethasone (13%) and prednisolone (13%) were the most commonly used systemic corticosteroids.
Prevalence of the 15 most frequently used drugs overall in each age group (per 100 children)
Discussion
This population-based study provides the first representative national description of drug use among French children in an outpatient setting. Overall prevalence of use was high, and much greater than that previously observed in other countries in studies performed using reimbursement claims databases, recently (61% in 2006 in Italy,13 55% in 2007 in Canada8) and earlier (60% in the late 1990s in the Netherlands,10 50.6% in Denmark12). However, these results are similar to previous reports in that the highest drug use was found among children aged <2 years. It is also well established that among teenagers there is a notable difference between genders.8 ,11 ,12 This particularly high prevalence of use in France may be related to differences in marketing authorisations (eg, tenoic acid nasal preparations exclusively marketed in France) and reimbursement status (eg, paracetamol and ibuprofen not reimbursed in some countries). This may also be related to French well-known overprescribing habits, that may be common with other European Mediterranean countries.24 ,25
The profile of drugs most commonly prescribed and reimbursed to children in France is consistent with the typical array of diagnoses seen in such subjects. As expected, analgesics and anti-inflammatory drugs, antibiotics, corticosteroids and antiasthmatics were among the most frequently used drugs. These are mostly considered as essential medicines for children,26 and it is possible to compare results to that found in other countries. For example, antibiotics were found here to be used by nearly half of children, which is among the highest prevalence reported in the existing literature: 42% in Canada 14 and 57% in Italy.27 Such high use in paediatric patients seems to be a reflection of antibiotic prescription in the general population which is higher in France than in other European countries.28 For antiasthmatics, the prevalence observed here (14%) was similar to the overall prevalence of use in developed countries (13%),29 but higher than that reported in Northern European countries such as the Netherlands (6%) or Norway (9%). Taken together, these data suggest that even essential medicines may not always be used in a rational manner, as has previously been suggested.30
More worrying is the widespread use of drugs that are unlikely to be effective and associated with safety concerns. For instance, domperidone is currently under review by the European Medicines Agency due to cardiac adverse reactions31 and phloroglucinol, frequently used for the treatment of benign symptoms despite a lack of efficacy data, can induce serious allergic reactions.32 However, the most striking and unexpected result is the frequent use of respiratory drugs, including nasal drops for common cold containing the sympathomimetic tuaminoheptane and the corticosteroid tixocortol, but also cough medications such as the antihistamine oxomemazine and helicidine. Nasal preparations were prescribed and reimbursed to 45% of French children in comparison with less than 5% in Canada8; cough and cold preparations were used by 2.3 per 1000 person-years in three European countries5 while the prevalence of drug use found here was 21%. This high use is all the more worrying as concerns over the efficacy and safety of such drugs in children have been growing over recent decades in the USA and Europe, and the licenses for decongestants, expectorants, antihistamines for cough management and other antitussives have been withdrawn for infants in France33 ,34 as well as in many countries.35 ,36 Indeed, nasal sympathomimetic decongestants were contraindicated in children aged ≤15 years owing to a risk of serious cardiovascular and neurological adverse effects, with frequent off-label/unlicensed use;37 ,38 the antitussive helicidine and cysteine derivative mucolytics were contraindicated in children aged <2 years due to paradoxically increased bronchorrhoea and acute respiratory distress;33 antihistamines for cough management, such as oxomemazine, were contraindicated in children aged <2 years owing to insufficient evidence for efficacy,34 risk of respiratory failure and neurological adverse effects, and a high risk of off-label/unlicensed use.38 ,39 Despite there being no age restriction for use of nasal corticosteroids, safety in younger children may be a concern, in particular as allergic rhinitis is often associated with asthma that may already be treated with inhaled corticosteroids.40
Our results are consistent with widespread off-label use of many medicines. However, this could not be verified from this database. Our results suggest that further research is required to determine why so many medicines are prescribed inappropriately, especially in young children. Additionally, more education on rational prescribing is required.
References
Footnotes
Contributors AB-L: conceptualised and designed the study, interpreted the data, drafted the initial manuscript and approved the final manuscript as submitted. JJ: carried out the analysis, reviewed and revised the manuscript, and approved the final manuscript as submitted. CD-P, RL: coordinated and supervised data collection, critically reviewed the manuscript, and approved the final manuscript as submitted. PR: interpreted the data, critically reviewed the manuscript and approved the final manuscript as submitted. PN: conceptualised and designed the study, interpreted the data, critically reviewed the manuscript and approved the final manuscript as submitted.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Drug therapy