Article Text

Abstract
Background The long-term prognosis of Henoch-Schönlein Purpura (HSP) is predominantly determined by the extent of renal involvement. There is no consensus as to whether treatment with prednisolone at presentation can prevent or ameliorate the progression of nephropathy in HSP.
Methods Children under 18 years of age with new-onset HSP were randomly assigned to receive prednisolone or placebo for 14 days. The primary outcomes were (a) the presence of proteinuria at 12 months (defined as urine protein : creatinine ratio (UP : UC) >20 mg/mmol) and (b) the need for additional treatment (defined as the presence of hypertension requiring treatment or renal biopsy anomalies or the need for treatment of renal disease) during the 12 month study period.
Results 352 children were randomised. Of those patients with laboratory UP : UC results available at 12 months, 18/123 (15%) patients on prednisolone and 13/124 (10%) patients on placebo had UP : UC >20 mg/mmol. There was no significant difference in the proportion of patients with UP : UC >20 mg/mmol at 12 months between the treatment groups (OR (prednisolone/placebo)=1.46, 95% CI 0.68 to 3.14, n=247), even after adjusting for baseline proteinuria and medications known to affect proteinuria (adjusted OR=1.29, 95% CI 0.58 to 2.82, n=247). Similarly, there was no significant difference in the time needed for additional treatment between the two groups (hazard ratio (HR) (prednisolone/placebo)=0.53, 95% CI 0.18 to 1.59, n=323).
Conclusions This is the largest trial of the role of steroids in children with HSP. We found no evidence to suggest that early treatment with prednisolone reduces the prevalence of proteinuria 12 months after disease onset in children with HSP.
Trial registration Number ISRCTN71445600
- Nephrology
- General Paediatrics
Statistics from Altmetric.com
What is already known on this topic
-
The long-term prognosis of Henoch-Schönlein Purpura (HSP) is predominantly determined by the extent of renal involvement.
-
There has been a long debate over the role of steroids in the prevention and management of HSP nephritis.
What this study adds
-
Our data do not support the routine use of prednisolone in early Henoch-Schönlein Purpura (HSP).
-
Further multicentre studies are required to assess the subgroup that develops more severe established HSP nephritis.
Introduction
Henoch-Schönlein Purpura (HSP) is the commonest small vessel vasculitis of childhood with an estimated incidence of 14–20.4/100 000.1 ,2
Renal involvement in HSP affects 20%–70% of patients2–,4 and ranges in severity from microscopic haematuria with or without proteinuria to a nephritic/nephrotic pattern with associated renal failure. In the majority of patients the outcome is excellent, with the incidence of severe long-term morbidity/mortality being less than 5%.2–,4 The presence of severe renal involvement early in the course of the disease is more likely to be associated with a poor outcome but these patients may make a complete recovery and clinical presentation is not reliable at predicting outcome.5
There has been a long debate over the role of steroids in the prevention and management of HSP nephritis (HSPN), since they were first described in the treatment of HSPN in the early 1950s. The highest quality evidence available prior to the start of our study was reported by Mollica et al6 in 1992. In this prospective trial, children with HSP with no renal involvement at presentation who received prednisone had significantly less proteinuria 12 months after initial presentation than those who did not receive prednisone. Although of great interest, the study was not randomised, placebo-controlled or blinded.
The rationale for undertaking the present study was to provide evidence to confirm or refute the benefit of early treatment with prednisolone on the development or progression of renal disease in children with HSP. The study hypothesis was that prednisolone would reduce the prevalence of proteinuria at 12 months after initial presentation.
Methods
Trial design
This was a multi-centre, blinded, parallel group, randomised (centre-stratified, allocation ratio 1 : 1) and placebo-controlled trial.
Patient enrolment
Children under 18 years of age presenting to one of the 24 participating secondary care centres in England and Wales with a diagnosis of HSP (HSP), based on the American College of Rheumatology criteria7 were eligible to participate in the study. Multicentre Research Ethics Committee approval was granted prior to commencing the study. Signed informed consent was obtained from the parents of all participating children.
Children were excluded from the study if they:
-
were already receiving steroid/immunosuppressive therapy;
-
were receiving ACE inhibitors;
-
had pre-existing renal disease (excluding urinary tract infections);
-
had pre-existing hypertension;
-
had evidence of immunodeficiency/systemic infection;
-
had contraindications or relative contraindications for steroid therapy (epilepsy, diabetes mellitus, glaucoma or peptic ulceration);
-
had had the characteristic purpuric rash for more than 7 days.
Intervention
Children were randomly assigned to receive either prednisolone at a dose of 2 mg/kg/day (max 80 mg) for 7 days, followed by 1 mg/kg/day for 7 days (max 40 mg) or placebo for 14 days. The trial drug was started within 7 days of the onset of the rash. Parents were instructed to dissolve tablets in 10–20 mL water and administer via a syringe or cup.
Definition of outcomes
There were three primary outcomes for this study: (a) proteinuria at 12 months (defined as urine protein : creatinine ratio (UP : UC) >20 mg/mmol), (b) the need for additional treatment and (c) the association of polymorphisms of the ACE gene with proteinuria at 12 months (to be reported separately). The need for additional treatment was defined as the occurrence of any of three component events (hypertension, renal biopsy anomaly and need for treatment of renal disease) in the 12-month study period. The presence of hypertension was identified from treatment with antihypertensive medication (patient notes were checked to confirm whether this was prescribed specifically to treat hypertension). Additional treatment for renal disease was identified from additional (non-trial) steroid therapy or ACE inhibitor medication prescribed for reasons other than hypertension.
The secondary outcome was the presence of symptoms of possible trial medication- induced toxicity; defined as the reporting of hypertension, abdominal pain, nausea and/or vomiting or adverse events before the end of the 4-week visit. As these symptoms are features of HSP as well as steroid toxicity, they were included if the clinician (who was blind to treatment allocation) deemed them probably or definitely due to the trial medication.
Sample size
A sample size calculation was performed prior to commencement of the study. It was estimated that 320 patients (160 per group) would be sufficient to test the hypothesis that the proportion of patients with UP : UC >20 mg/mmol at 12 months would differ between patients given prednisolone and those given placebo. This estimate was based on anticipated proportions of 0.05 and 0.15 in the prednisolone and placebo groups, respectively, and a two-tailed, χ2 test, using 80% power and 5% significance level. Allowing for a dropout rate of up to 15%, the study aimed to recruit 378 patients (189 per group).
Randomisation
Centre-stratified block randomisation was used to allocate patients to treatment groups (allocation ratio: 1 : 1). A computerised random number generator was used to generate the random allocation sequences. Randomisation lists for each centre were sent to the pharmacy at St Mary's Hospital, Penarth, in order to ensure that concealment of allocations was maintained. Trial medications (active and placebo) appeared identical and were supplied by GlaxoSmithKline and were dispensed into bottles to provide a total dose of 1150 mg soluble medication (230×5 mg tablets) per bottle.
Patients, parents, paediatricians and all investigators were blind to treatment allocation. Statisticians were blinded until after recruitment had finished and the trial database closed.
Clinical and study follow-up
Clinical assessments took place at randomisation, 4 weeks, 3 months and 12 months. At each visit there was documentation of clinical characteristics, adverse events and dipstick urinalysis for the presence of blood and protein. Quantitative analysis of UP : UC ratio was undertaken at randomisation, at 12 months and when indicated by the presence of proteinuria on dipstick. Blood pressure checks and urinalysis were undertaken weekly in primary care until the week 4 assessment. Blood was taken for serum electrolytes, creatinine and albumin at the time of presentation, and thereafter, as clinically indicated. Patients were referred for consideration of renal biopsy if they had deterioration of kidney function, acute nephrosis or persistence (>4 weeks) of nephrotic range proteinuria, defined as UP : UC >200 mg/mmol.
Statistical methods
Prior to analysis, acceptable time windows for the visits were defined. Data collected outside an acceptable time window for a particular visit were not included in any analyses relating to that specific visit, but were made available for other non-visit specific analyses. Patients who did not attend the 12-month visit were sent a letter asking them to provide a 12-month urine sample. Data from any such samples were included in the UP : UC analyses at 12 months, provided they were collected within the 9–18 month window. Hence it should be noted that, for some analyses, the denominators used may be greater than the number attending that visit.
Comparisons were made between consenting patients and eligible non-consenting patients with respect to available demographic variables. χ2 or Fisher's exact tests were used for categorical variables and t tests or Wilcoxon rank sum tests for continuous variables, as appropriate.
Logistic regression was used to compare UP : UC>20 mg/mmol between the treatment groups. Binary variables indicating baseline UP : UC >20 mg/mmol and the use of antihypertensive drugs known to affect proteinuria levels (enalapril and losartan) were included in an adjusted analysis. Patients with missing UP : UC data at 12 months were excluded. If baseline UP : UC was missing, dipstick data were used where available; if not, then random numbers were used to assign baseline UP : UC >20 mg/mmol status in accordance with the proportion of baseline UP : UC >20 mg/mmol for those with non-missing data. Interactions between variables were examined and retained if significant at the 5% significance level.
The need for additional treatment was analysed as a time to event outcome (time in days from randomisation to starting relevant additional medication or undergoing renal biopsy, whichever was earlier). Patients not requiring additional treatment were treated as censored observations, with analysis times calculated as the time from randomisation to last follow-up (providing follow-up was at least 2 weeks). A Cox proportional hazards model was used to compare treatment groups.
The numbers of patients experiencing symptoms of possible trial medication-induced toxicity are described by treatment group for patients who attended the 4 week visit or reported any adverse events before the end of the 4- week visit. The numbers of patients experiencing adverse events (at any time during the study period) are described by treatment group, along with the perceived relationship to trial therapy. No formal statistical comparisons were made between the groups due to low event rates.
All analyses were performed on an intention to treat basis. Continuous data are summarised using means and SDs or medians and interquartile ranges as appropriate. Categorical variables are presented as numbers and percentages. Results of statistical models are presented as effect sizes with 95% CIs. It was not possible to adjust for centre due to the small numbers of patients at many of the centres. Two-sided tests and a 5% significance level were used throughout. No adjustments were made for multiple testing. Analyses were performed using Stata V.11.0.8 The results of the trial are reported in accordance with the Consolidated Standards of Reporting Trials statement 2010 guidelines.9 ,10
Results
Participants
Figure 1 shows the flow of participants through the study. Between January 2001 and January 2005, 460 children with HSP were assessed for trial eligibility. There was no evidence to suggest any differences between eligible patients who declined to take part (n=82) and randomised patients (n=352) in terms of age (p=0.54), gender (p=0.28) or ethnic origin (p=0.73).
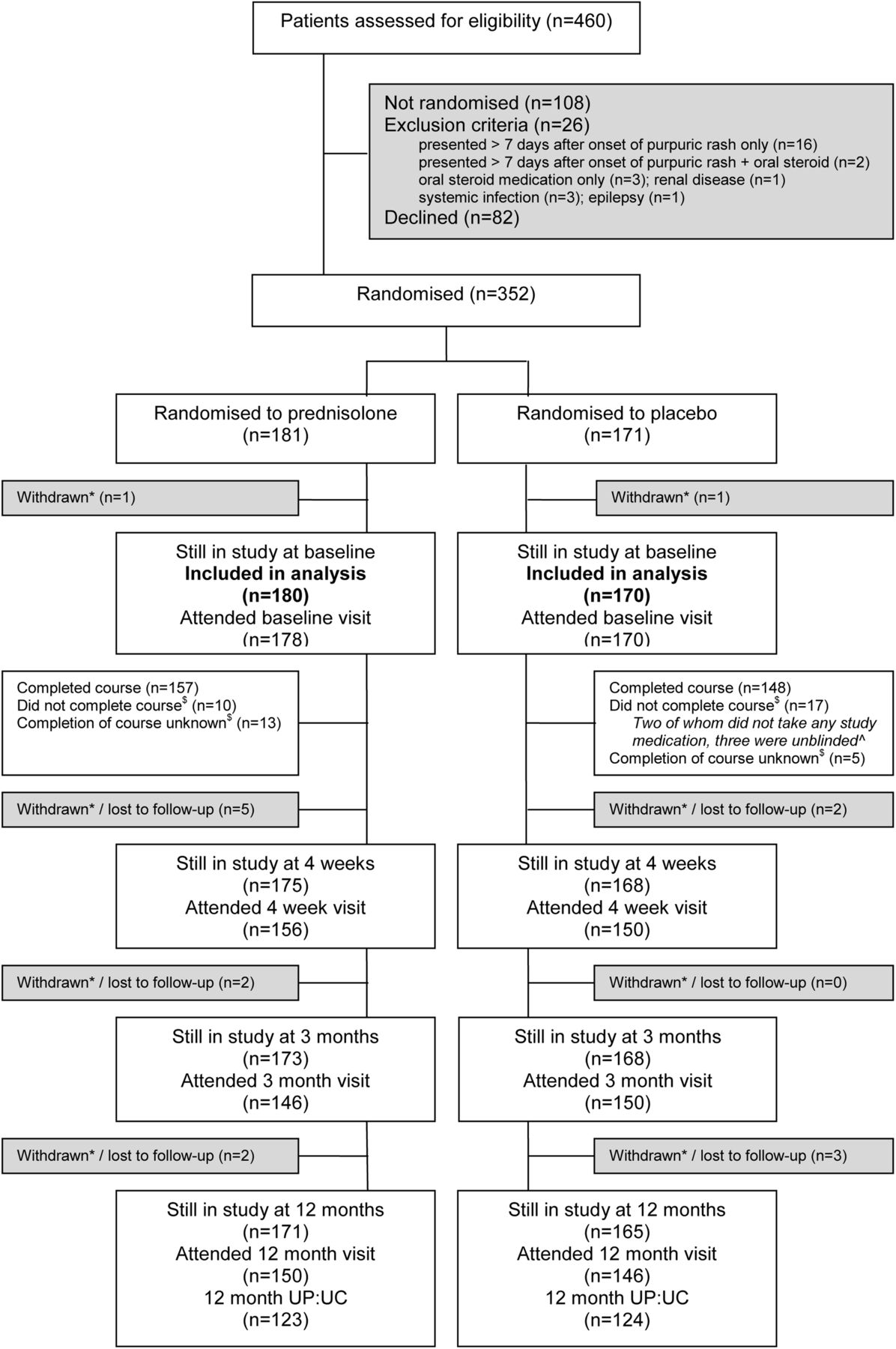

Flow chart showing recruitment, randomisation and follow-up of patients.
Two patients (one per group) withdrew shortly after randomisation without providing baseline information or taking any study medication and were excluded from the analysis. 296 children attended the 12 month visit.
Twenty-seven patients did not complete the full course of study medication (10 prednisolone, 17 placebo). Three patients on placebo, who did not complete the full course of study medication, were unblinded. For a further 18 patients (13 prednisolone, 5 placebo) completion of course of study medication was unknown.
Baseline characteristics are detailed in table 1; dipstick urine data at each visit are detailed in table 2. Haematuria and proteinuria on dipstick were seen more frequently in patients on prednisolone than those on placebo, both at randomisation and at subsequent visits. Baseline UP : UC >20 mg/mmol was more common in patients on prednisolone (19%(26/135)) compared with those on placebo (8%(12/142)).
Baseline clinical characteristics
Dipstick urine by visit
Primary outcome measures
Urine protein : creatinine
At 12 months, UP : UC results were available for 123/171 (72%) patients on prednisolone and 124/165 (75%) patients on placebo. 18 out of 123 (15%) patients on prednisolone and 13/124 (10%) patients on placebo had UP : UC >20 mg/mmol. There was no significant difference in the proportion of patients with UP : UC >20 mg/mmol at 12 months between the treatment groups (OR(prednisolone/placebo)=1.46, 95% CI 0.68 to 3.14, p=0.33, n=247), even after adjusting for baseline proteinuria and the use of antihypertensive drugs known to affect proteinuria levels (adjusted OR=1.29, 95% CI 0.58 to 2.82, n=247). UP : UC baseline values were missing for 40 patients; dipstick values were used for 36 of these patients and imputed values for the remaining four patients. Of the 31 patients with UP : UC >20 mg/mmol at 12 months, only nine (29%) had UP : UC >20 mg/mmol at baseline (figure 2). 1 out of 123 (1%) patients on prednisolone and 0/124 patients on placebo had nephrotic range proteinuria (UP : UC >200 mg/mmol) at 12 months.

{kind=link}
{kind=link}
{kind=link}
Urine protein : creatinine ratio measurements at baseline and 12 months.
Need for additional treatment
164 out of 180 (91%) patients on prednisolone and 159/170 (94%) patients on placebo were included in the analysis of time to need for additional treatment. Fourteen patients (five prednisolone and nine placebo) required additional treatment (table 3). Renal biopsy was indicated in 1/164 (1%) patients on prednisolone and 4/159 (3%) patients on placebo, and confirmed the presence of mesangial IgA deposition and mesangial proliferation in all five patients. One patient on prednisolone had evidence of extracellular crescent formation in 7% of glomeruli. There were too few events to estimate median times to need for additional treatment. The estimated occurrence rates at 12 months were 3% (95% CI 1% to 7%) in the prednisolone group and 6% (95% CI 3% to 11%) in the placebo group. There was no significant difference between the two groups (HR (prednisolone/placebo)=0.53, 95% CI 0.18 to 1.59, n=323).
Timing of events for the 14 patients experiencing ‘need for additional treatment’
Secondary outcome and adverse events
Trial medication induced toxicity (hypertension/gastro-intestinal upset)
158 out of 175 (90%) patients on prednisolone and 152/168 (90%) patients on placebo attended the 4 week study visit and/or provided information on adverse events for this period. Of these patients, 2/158(1%) patients on prednisolone and 1/152(1%) patients on placebo experienced symptoms of possible trial medication induced toxicity. None of the patients with symptoms of toxicity experienced hypertension.
Adverse events
27 out of 180 (15%) patients on prednisolone and 23/170 (14%) patients on placebo experienced at least one adverse event. The frequency and percentage of all individual adverse events in the 12 month study period are given in table 4.
Adverse events
Discussion
This study of 352 unselected children with HSP demonstrated no benefit of prednisolone over placebo in reducing the risk of proteinuria 12 months after the onset of HSP.
The strength of this study is that it is the largest prospective, randomised, placebo-controlled trial of the role of steroids in HSP in the literature to date, and therefore, provides the best evidence available to evaluate this treatment. In an earlier study of 168 patients conducted by Mollica in 1992,6 patients were alternately allocated to receive prednisone (1 mg/kg/day 2 weeks) or no treatment. This study reported a beneficial effect of prednisone in reducing the incidence of nephropathy 2–6 weeks after recovery from the acute phase of the disease (χ2=13.02, p<0.001). This study was not randomised, placebo-controlled or blinded and did not justify its sample size. Such methodological failings have been shown to be associated with biased results in favour of the intervention.11 ,12
Our results are in line with those of two other smaller prospective randomised controlled trials (RCTs). In the first,13 40 patients with HSP were randomised to receive prednisolone 2 mg/kg for 1 week followed by a weaning dose over the second week. Although almost certainly underpowered, the authors reported no difference in the incidence of renal involvement at 1 year. In the most recent RCT prior to ours, 171 patients were assigned to receive prednisolone 1 mg/kg/day for 2 weeks followed by a weaning dose over 2 weeks (a similar total dose to our study), or placebo and followed for 6 months.14 Ronkainen and colleagues concluded that prednisolone did not prevent the development of nephritis, but reported that in patients who developed nephritis within the first month of the illness, patients on prednisolone achieved a more rapid resolution of renal disease than patients on placebo. This effect was most apparent in children over 6 years of age with renal symptoms at onset; however, this was a limited group of only 21 patients (10 on prednisolone, 11 on placebo). The group also defined renal disease as proteinuria based on protein concentration and/or haematuria. UP concentration is less reliable at identifying significant urinary protein loss than UP : UC ratio.15 Long-term outlook is related to proteinuria rather than haematuria alone and it is unclear whether this study demonstrated any benefit of steroid use in terms of more rapid reduction of proteinuria. This cohort of patients was re-evaluated 8 years after the initial presentation and the results confirmed the lack of benefit of early routine use of steroids in preventing nephropathy.16
The limitation of our study is that we did not meet our sample size target of 320 patients. We recruited 352 children, 296 (84%) of whom completed the study. The number of patients declining randomisation was higher than expected (82/460(18%)). We offered patients a non-randomisation follow-up arm, which may have influenced this, and funding was not available to extend the study. Although the dropout rate, in terms of those attending the 12-month visit, was 16% (56/352), which was very close to the estimated dropout rate of 15%, only 70% (247/352) of those randomised had the primary outcome measure recorded at 12 months (equivalent to a 30% dropout rate). These figures might have been improved with the appointment of more than one trial coordinator.
We recorded basic demographic data on eligible patients who declined to take part in the study, to ascertain whether there were any differences between those who consented and those who did not. We found no evidence of volunteer bias. We are also confident that our sample is representative of the general population of children with HSP, based on clinical features at presentation. There is no reason to suggest that our results cannot be generalised to the HSP population as a whole.
It is noteworthy that more patients on prednisolone had evidence of nephritis at baseline, both in terms of UP : UC and haematuria and proteinuria on dipstick, compared with patients on placebo. However, the analyses were adjusted for baseline UP : UC and the use of antihypertensive drugs known to affect proteinuria levels (enalapril and losartan) administered at any time during the 12 month study period; there was still no benefit of prednisolone after adjusting for these factors.
Our second primary outcome was the need for additional treatment, which could have masked the benefit of steroids. Five patients on prednisolone and nine patients on placebo required additional treatment during the study period. When examining all the results of our study, there is some suggestion of a trend towards more severe disease in the placebo group; however, none of the differences were statistically significant.
It is possible that we did not find a statistically significant difference between the treatment groups as we had insufficient statistical power due to not quite meeting the target sample size. However, a meta-analysis by Weiss et al in 2007,17 published before our study data, were available, but including the studies by Mollica, Huber and Ronkainen,6 ,13 ,14 concluded that steroids did reduce the risk of developing persistent renal disease. This conclusion was subsequently changed in a systematic review in 200918 that included preliminary data from our study together with those included in the Weiss paper. The authors concluded that there was no evidence of benefit of early short-term steroids in the prevention or treatment of HSPN 6–12 months following presentation. We consider that our study was pivotal in reaching this conclusion.
In summary, we have shown no beneficial effect of routine steroids in unselected cases of HSP. We cannot, however, draw any conclusion about those with established significant renal disease. Further multicentre studies are required to assess the subgroup that develops more severe established HSPN. Our data do not support the routine use of prednisolone in early HSP.
Acknowledgments
We would like to thank the Wales Office for Research and Development (WORD) for providing the funding for this study, GlaxoSmithKline for supplying prednisolone and placebo medication and Dr Chris Rogers (Research and Development Support Unit, North Bristol NHS Trust) for providing statistical input during the early stages of this study.
References
Footnotes
-
Collaborators Dr David Tuthill, Llandough Hospital, Cardiff, Dr Lynne Millar-Jones, Royal Glamorgan Hospital, Ynys Maerdy, Dr Ian Bowler, Royal Gwent Hospital, Newport, Dr Tom Williams, Nevill Hall Hospital, Abergavenny, Dr Mike Maguire, Prince Charles Hospital, Merthyr Tydfil, Dr Katherine Wooding, Princess of Wales Hospital, Bridgend, Dr Michelle James-Ellison, Singleton Hospital, Swansea, Dr Gustav vas Falcoa, Withybush Hospital, Haverfordwest, Dr Gwynneth Owen, West Wales General Hospital, Carmarthen, Dr John Williams, Bronglais Hospital, Aberystwyth, Dr Tom Yuille, Glan Clwyd Hospital, Rhyl, Dr Brendan Harrington, Wrexham Maelor Hospital, Wrexham, Dr Helen Price, Princess Margaret Hospital, Swindon, Dr Michelle Hamilton-Ayres, Cheltenham General Hospital, Dr Simon Meyrick, Hereford County Hospital, Dr John Brice, Royal Shrewsbury Hospital, Dr Philip Wylie, Dorset County Hospital, Dorchester, Dr Robert Jones, Derriford Hospital, Plymouth, Dr Corrinne Hayes, Royal Devon and Exeter Hospital, Exeter, Dr Nicki Gilbertson, Royal Cornwall Hospital, Truro, Dr Charles Godden, Royal Surrey Hospital, Guildford, Dr Theo Fenton, Mayday Hospital, Croydon, Dr Nick Webb, Manchester Royal Children's Hospital.
-
Contributors JD, GS and JT were responsible for trial design, application for funding, appointment of trial coordinator and manuscript preparation. KP and KB have undertaken the statistical analyses. AL-E was the trial coordinator.
-
Funding Wales Office for Research and Development.
-
Competing interests A GlaxoSmithKline supplied prednisolone and placebo for the submitted work. Jane Tizard receives dividends with shares from GlaxoSmithKline. There have been no other financial relationships with any organisations that might have an interest in the submitted work in the previous three years and no other relationships or activities that could appear to have influenced the submitted work.
-
Ethics approval Multicentre Research Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.