Article Text

Abstract
Background Information on variation in the recording of child maltreatment in administrative healthcare data can help to improve recognition and ensure that services are able to respond appropriately.
Objective To examine variation in the recording of child maltreatment and related diagnoses.
Design Cross-sectional analyses of administrative healthcare records (Hospital Episode Statistics).
Setting and participants Acute injury admissions to the National Health Service in England of children under 5 years of age (1997–2009).
Outcome measure Annual incidence of admission for injury recorded by International Classifications of Diseases 10 codes for maltreatment syndrome (child abuse or neglect) or maltreatment-related features (assault, undetermined cause or adverse social circumstances). Proportion of all admissions for injury coded for maltreatment syndrome or maltreatment-related features.
Results From 1997 to 2009, the annual incidence of injury admissions coded for maltreatment syndrome declined in infants and in 1–3-year-old children while admissions coded for maltreatment-related features increased in all age groups. The combined incidence of these categories remained stable. Overall, 2.6% of injury admissions in infants, and 0.4–0.6% in older age groups, had maltreatment syndrome recorded. This prevalence more than doubled when maltreatment-related codes were added (6.4% in infants, 1.5–2.1% in older age groups).
Conclusion Despite a shift from maltreatment syndrome to codes for maltreatment-related features, the overall burden has remained stable. In combination, the cluster of codes related to maltreatment identify children likely to meet thresholds for suspecting or considering maltreatment and taking further action, as recommended in recent National Institute of Health and Clinical Excellence guidance, and indicate a considerable burden to which hospitals should respond.
Statistics from Altmetric.com
Introduction
Systems to support recognition of and response to child maltreatment are a cornerstone of policy.1,–,3 Healthcare administrative data offer a readily available system that could be used to monitor management of maltreatment, but a recent systematic review of 38 studies using International Classifications of Diseases (ICD) concluded that child maltreatment was under-reported in healthcare databases and death registrations.4 These findings are likely to apply to the UK, although only two of the 38 studies in the review were carried out in the UK and both were small studies done in the 1990s.5 6 To address the problem of under-recording, the review proposed the development of new codes for ‘possible’ maltreatment or cases ‘under review’ in order to reflect clinical uncertainty and the lengthy investigations that are sometimes required.
What is already known on this topic
▶ Maltreatment is under-recorded in healthcare records in developed countries.
▶ National Institute of Health and Clinical Excellence guidance recommends investigation or follow-up of children in whom health professionals suspect or consider maltreatment.
What this study adds
▶ The combined incidence of admissions with codes for maltreatment syndrome and maltreatment-related features remained stable or increased marginally, while maltreatment syndrome declined.
▶ Monitoring should be based on a range of codes reflecting maltreatment-related features.
▶ Clinicians should consider or suspect child maltreatment in a significant minority of injury admissions.
Clinical guidance published by the UK National Institute of Health and Clinical Excellence (NICE) in July 2009 on “when to suspect child maltreatment” marks a further step towards official recognition of the inherent uncertainty in recognising child maltreatment. The guidelines link alerting features to thresholds for suspecting or considering child maltreatment.3 These features (eg, physical signs of abuse, lack of a suitable explanation, adverse or inappropriate behaviour, appearance, or parent–child interaction) cover a broad range of presentations that, at the very least, warrant further consideration of maltreatment through discussion with other professionals or follow-up. Information on the number of children likely to be affected by such alert features is important to ensure that healthcare services have the resources to respond as recommended by NICE.
We used administrative healthcare data for the National Health Service (NHS) in England (http://www.hesonline.nhs.uk) to determine trends in the incidence of hospital admission for injury related to maltreatment in children under 5 years old. We used codes for maltreatment syndrome and for features related to maltreatment to identify children who would warrant consideration or suspicion of maltreatment as defined by the NICE guidance.3 In subgroup analyses, we compared severe injury admissions in Hospital Episode Statistics (HES) with equivalent admissions recorded in the Trauma Audit and Research Network (TARN; https://www.tarn.ac.uk/). Both systems use hard copy NHS records to allocate codes, but coders and coding instructions differ.7 8
Methods
The study examined acute injury admissions of children aged between 1 week and 5 years old to NHS hospitals in England. Data were available from April 1997 to February 2009, and are grouped in financial years, April to March. Acute hospital admissions were defined by linked consultant episodes of inpatient care and included day cases.8 Each episode of care can have up to 20 diagnostic codes, although 90% of episodes had four or less codes recorded. An admission was considered to be for injury if any diagnostic code was recorded for injury, poisoning or other consequences of external cause, specified in sections S or T (chapter XIX) of the ICD-10.9
We used the alert features listed in the NICE guidance and expert opinion elicited during stakeholder meetings for the project to select codes that would be expected to trigger consideration or suspicion of child maltreatment. Causes of injury were classified according to a hierarchy of codes reflecting a diminishing likelihood of maltreatment (table 1 and online table 1). None provide definitive evidence of maltreatment. We separately analysed codes for maltreatment syndromes (ICD-10 T74, Y06 and Y07) and grouped those related to maltreatment as assault, undetermined cause and adverse social circumstances (online table 1). Examples of clinical cases are given in the box in the online appendix.
Acute injury admissions to NHS hospitals in England from 1997 to 2009 (source: Hospital Episode Statistics†)
We calculated the proportions of injury admissions in an exclusive descending hierarchy of injury categories: maltreatment syndrome (including neglect or abandonment, physical, sexual and/or psychological abuse), codes related to maltreatment (assault, undetermined cause, adverse social circumstances), ingestions, accidents, injuries coded for co-morbidity or complications and admissions with no explanation (online table 1). We analysed all types of injuries and the following types of injury that are strongly associated with child maltreatment in preschool children10: (a) fractures (ICD-10 codes S02, S12, S22, S32, S42, S52, S62, S72, S82, S92, T02, T10 and T14.2); (b) head injuries (ICD-10 codes S00 to S09) and (c) subcategories of head injury in a hierarchy related to the risk of maltreatment (intracranial injury (code S06); skull fracture but no intracranial injury (codes S02.0, S02.1 and S02.7); fractures of facial bones (S02.2, S02.3, S02.4, S02.5, S02.6, S02.8, S02.9) and other head injuries).
We conducted subgroup analyses of the HES database to determine the extent of under- or over-reporting of maltreatment. These analyses compared severe injury admissions in HES with equivalent admissions included in the TARN trauma registry for the period (1997–2006). TARN is a collaborative research group based at the University of Manchester that independently collects and analyses clinical data for severe injury admissions from 109 (60%) trauma-receiving hospitals in England and Wales. Contribution to TARN is voluntary and hospitals represent a range of teaching, general, urban and rural services.11 12 We used an algorithm developed by TARN to extract admissions from HES that met the same severity criteria as the admissions included in TARN. These criteria include admission for more than 72 h, admission to intensive care or high dependency care for any duration, inter-hospital transfer, or death within 93 days.7 Separate teams of coders enter data for HES and for TARN. For both databases, coders are trained to scan hard copy hospital notes and record all available diagnoses using ICD-10 codes. The process of data abstraction and coding for maltreatment is similar except that TARN coders record any mention of suspected child abuse or assault. From 2002, HES coders were instructed to code only probable or definite diagnoses recorded in the hospital notes, but not diagnoses that were suspected or possible.13
Analyses
Annual incidence rates were calculated by dividing the number of admissions coded for maltreatment syndrome or any maltreatment-related features by age-specific population estimates for each calendar year. The population denominators were based on mid-year population estimates obtained from the UK Office of National Statistics website for each age group, taking into account births, deaths and migration.14 15 We adjusted the population estimate for the 11-month data collection period for 2008–2009. Time trends in the annual incidence of maltreatment syndrome, and maltreatment-related codes (undetermined cause and adverse social circumstances), were examined for linear trend using Poisson regression. Assault was excluded from these trend analyses of separate categories due to small numbers.
We used a funnel plot to determine the variation between hospitals in recording of any maltreatment (maltreatment syndrome and maltreatment-related codes combined). These analyses were restricted to hospitals with more than 100 injury admissions during the 12-year study period and compared the proportion of all injury admissions with any code related to maltreatment. We compared each hospital against 2 SDs of the overall mean, using the Wilson method to derive the funnel limits.16 We estimated the prevalence rates adjusted for the child's age and quintiles of the multiple deprivation index based on postcode at admission,17 by multiplying the ratio between the observed and expected prevalence by the national prevalence of maltreatment-related injury. The expected prevalence was estimated using logistic regression.18
Results
Acute injury admissions accounted for 4.6% of all hospital admissions in infants, 11.2% for children aged 1–3 years and 12% for children aged 3–5 years. Between 1997 and 2009, the annual incidence of acute admission for injury increased marginally for infants (from 12.1/1000 to 13.5/1000 children/year) but declined slightly in older children (1–3 years: from 17.8/1000 to 16.0/1000; 3–5 years: from 12.1/1000 to 11.7/1000 children/year).
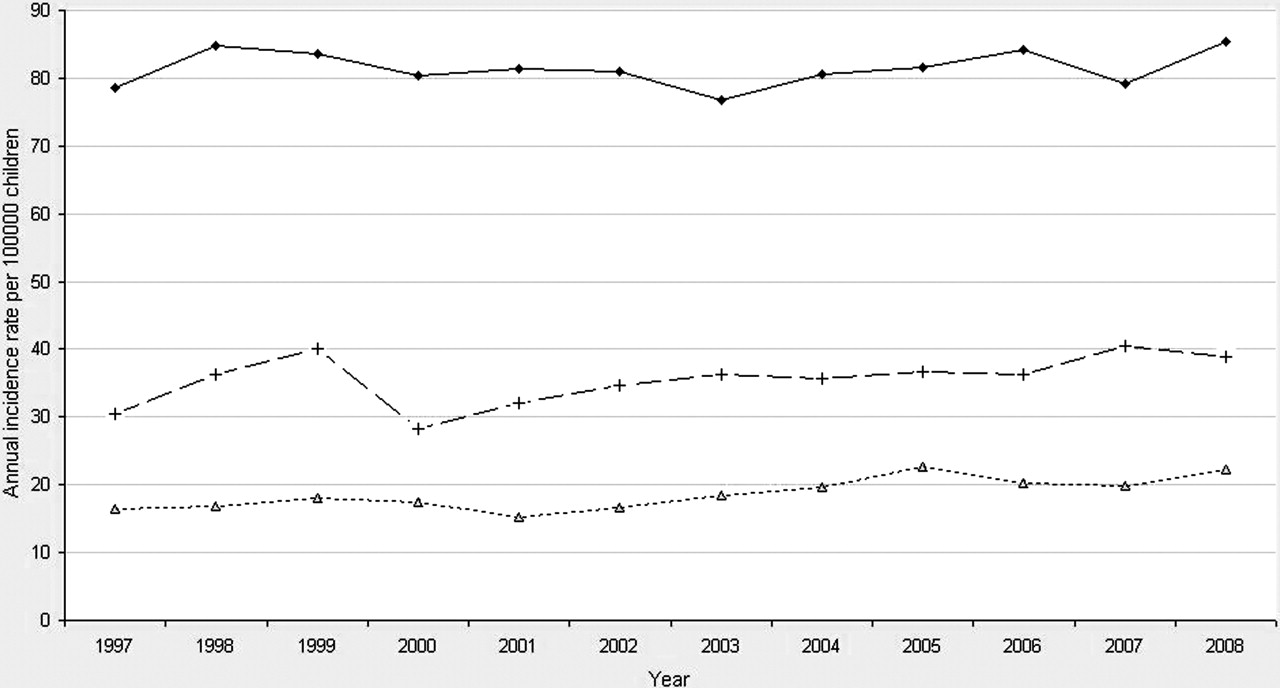
Accidents accounted for 60–70% of all acute injury admissions (table 1). A small proportion of admissions (5–6%) had no code for cause of injury (table 1). The annual incidence of admissions with codes for maltreatment syndrome declined significantly over time in infants (p<0.0001) and in children aged 1–3 years (p<0.0001), but not in children aged 3–5 years (p=0.088; figure 1). In contrast, the incidence of acute injury admissions coded for maltreatment-related features (mainly undetermined cause and adverse social circumstances) increased significantly in all age groups and by 2008 outnumbered codes for maltreatment syndrome (p<0.0001; figure 1). The very low annual incidence of assault (0.03–0.09/1000) did not change appreciably over time. Between 1997 and 2009, the annual incidence of all maltreatment-specific and maltreatment-related admissions combined remained constant for infants (0.81/1000 infants on average) but increased in the older age groups (1–3 years: from 0.30/1000 to 0.39/1000; 3–5 years: from 0.16/1000 to 0.22/1000; p<0.0001; figure 2).

Annual incidence rates per 100 000 children of acute injury admissions with codes for maltreatment syndrome (solid line), undetermined cause (dashed line) and adverse social circumstances (dotted line). Data for assault not shown. (A) Infants. (B) Children aged 1 to less than 3 years. (C) Children aged 3 to less than 5 years. Source: Hospital Episode Statistics.

Annual incidence rates per 100 000 children of acute injury admissions with all codes for maltreatment-related features in infants (solid line), children aged 1 to less than 3 years (dashed line) and children aged 3 to less than 5 years (dotted line). Source: Hospital Episode Statistics.
The proportion of acute injury admissions with codes for maltreatment syndrome was higher in infants (2.6%) than for older children (1–3 years: 0.6%; 3–5 years: 0.4%; table 1). By 2008–2009, admissions with any code for maltreatment syndrome or maltreatment-related features accounted for 6.3% of all injury admissions of infants, and 2.2% and 1.6%, respectively, of all injury admissions in children aged 1–3 years and 3–5 years.
The type of head injury was strongly predictive of maltreatment syndrome in infants but not in older children. For example, in infants, codes for maltreatment syndrome were recorded eight times more frequently for intracranial injury (13.7%) than for head injuries without skull fracture or intracranial injury (1.7%; table 1). Almost two-thirds (61.4%) of admissions for intracranial injury in infants occurred in children under 6 months of age and 18.9% of these had codes recorded for maltreatment syndrome (results not shown). However, the overall number of admissions giving rise to consideration or suspicion of maltreatment, whether defined by codes for maltreatment syndrome or for maltreatment-related features, was much higher in children with head injuries without skull fracture or intracranial injury than for those with intracranial injury (table 1).
Admissions were more likely to contain codes for maltreatment syndrome if a paediatrician was one of the specialists recorded as being responsible for care (3.25% of infants and 1.13% of older children) compared with no record of a paediatrician being responsible (0.7% infants and 0.06% of older children). There was no record of a paediatric consultant being responsible for care in 23.7% of all acute injury admissions in infants, or in 47.2% and 63.7% of the 1–3 year and 3–5 year age groups, respectively, but it is not known whether this reflects lack of paediatric scrutiny or coding practices.
The proportion of all acute injury admissions with any codes for maltreatment syndrome or maltreatment-related features varied from 0% to 9.9% across 217 hospitals (figure 3). These codes were strongly associated with deprivation and were recorded more than twice as often for children living in the most deprived quintile compared with the least deprived (OR 2.60; 95% CI 2.43 to 2.77). In 75 hospitals, the deprivation-adjusted prevalence of all maltreatment codes combined was significantly lower than the mean prevalence for all hospitals at a two-sided 0.05 level of significance, indicating possible under-recording given the expected national variation (figure 3).

{kind=link}
{kind=link}
{kind=link}
Funnel plot showing variation in the combined prevalence of any codes related to maltreatment recorded by NHS trusts, adjusted for age and deprivation. The horizontal line represents the mean prevalence (2.75%) and its 95% confidence limits. Denominators are all acute injury admissions per trust. Thirty-five per cent of NHS trusts fall below the lower control limit.
Table 2 shows the number of severe injury admissions recorded in the TARN trauma registry and similarly severe admissions recorded in HES between 1997 and 2006. The proportion of injury admissions with maltreatment syndrome or assault codes was approximately 20% lower in HES than in TARN (8.5% in TARN; 6.9% in HES). This level of under-recording in HES persisted throughout the period from 1997 to 2006 (data not shown). The prevalence of maltreatment syndrome or assault codes was highest for infants with head injury (39.4% in TARN; table 2). Overall, the combined prevalence of admissions with any codes for maltreatment syndrome or maltreatment-related features among severe injury admissions was slightly higher in HES than in TARN (table 2).
Prevalence of codes for maltreatment syndrome and maltreatment-related features in severe injury admissions in the TARN trauma registry and in HES between 1997 and 2006, inclusive
Discussion
The annual incidence of injury admissions coded for maltreatment syndrome declined in infants and in 1–3 year olds, while admissions coded for maltreatment-related features increased in all age groups. The combined incidence of these categories remained stable and represents 1.5–6.4% of all acute injury admissions in children under 5 years old. There was wide variation between hospitals in recording of maltreatment-specific and maltreatment-related codes, which was not explained by age, deprivation indices or case load. Compared with a national trauma registry, maltreatment-specific codes or assault were recorded less frequently in HES.
These analyses are based on a standardised approach to data recording, which made it possible to assess variation across NHS hospitals in England over several years. A weakness of the study is the lack of information on the extent to which codes specifically for maltreatment syndrome or for maltreatment-related features reflect real clinical concern or action by healthcare professionals. Obtaining such information would require hard copy record review or clinical follow-up, which might in itself alter clinicians' actions. This problem would be avoided if health and social care data were linked to create anonymised data for analyses. Such data could provide powerful insights into the health problems faced by maltreated children seen by social care,19 20 and into the pathways from health into social care.21,–,23 Without follow-up data, our inferences about the sources of such variation need to be cautious as recording of maltreatment in HES reflects processes at three levels: recognition by clinicians, recording in hospital notes and the quality of information capture by hospital coders and their approach to coding.
The evidence of under-recording of maltreatment syndrome in HES is consistent with previous findings that clinicians record or report only a minority of the child maltreatment cases that they recognise.4 23,–,25 Reasons include uncertainty about the diagnosis, inadequate clinical knowledge or inexperience, clinician–family interactions, concerns about the capacity of services to respond and fears that recording maltreatment will do more harm than good.24,–,28 However, large discrepancies between our results for England and the USA suggest that under-recording is only part of the problem.
Compared with studies based on hospital discharge codes in the USA, the prevalence of maltreatment recorded for acute injury admissions in England was unexpectedly low. For example, Chang et al29 reported that 11.1% of infants and 2.4% of children aged 1 or 2 years old admitted to an urban paediatric trauma centre had maltreatment recorded. More recently, Leventhal et al30 reported an incidence rate of admissions for fractures attributable to abuse of 36.1/100 000 infants (95% CI 31.0 to 41.2) in 2003 (defined by codes for maltreatment syndrome or assault), which is more than twice the corresponding rate for 2003 in HES (13.4/100 000 infants; 95% CI 10.4 to 16.4; analyses restricted to admissions for >1 day and codes for maltreatment syndrome or assault; cross mapping of ICD-9 to ICD-10 codes is available from the authors). The rate in HES for all codes related to maltreatment was only slightly higher, 18.9/100 000 (15.4 to 22.5). One explanation is that the incidence of maltreatment is lower in the UK than in the USA, but previous reviews of international comparisons suggest that any differences are unlikely to be of this magnitude.31 32 Other explanations include poorer recognition or higher thresholds for coding maltreatment in the UK. In addition, data for the USA may reflect a higher threshold for admission or may underestimate the denominator population. Further research is required to determine the true prevalence of injury admissions in England for which clinicians should consider or suspect maltreatment. However, these comparisons suggest that our findings represent a lower estimate.
The shift from codes for maltreatment syndrome to codes for maltreatment-related features may be due to several factors. First, instructions to HES coders in 2002 to record only probable or definite diagnoses, not suspected cases, would likely have contributed to the decline.13 Second, two high profile court cases against paediatricians alleging maltreatment may have encouraged replacement of references to maltreatment in hospital notes with documentation of concerns about adverse social circumstances or undetermined cause.33,–,35 Third, growing awareness of the need to safeguard vulnerable children following publication of government policy in Working together to safeguard children in 1999,36 and the 2004 Children Act, may have contributed to the overall increase in recording of adverse social circumstances.2 37
Clinical and policy implications
One implication of our findings for service providers is that a significant minority of children admitted with injury have features that would be expected to alert clinicians to consider or suspect child maltreatment and take further action. The wide variation in the prevalence of this minority may reflect suboptimal recognition in some hospitals. To respond to the needs of children who may have been subjected to maltreatment, hospital services should be aware that our results for injury admissions provide a minimum estimate of hospital contacts requiring a response. Children at risk of maltreatment will also be identified among non-injury admissions, and much more frequently, among children attending the accident and emergency department and outpatient clinics. To enable healthcare services to respond, hospitals need adequate resources in terms of experienced paediatricians, community liaison nurses and social workers linked to hospital teams.38 Community health services need sufficient professionals, such as health visitors, school nurses and general practitioners, to respond to inquiries, follow up children in whom maltreatment is considered or suspected, and implement supportive or protective interventions. For many of the children for whom clinicians consider or suspect maltreatment, healthcare has a role as the initiator and monitor of early interventions as burgeoning referrals to social care services will mean that only extreme cases command attention.39
The implications of our findings for coders and policy makers are that codes for maltreatment-related features may be more acceptable to clinicians than insistence on specific codes for maltreatment syndrome. In combination, these codes could be used to monitor the impact of policy initiatives such as the NICE guidance. However, for international comparisons of the burden and trends in maltreatment, new ICD codes need to be devised as recommended by Scott et al.4 These need to reflect the uncertainty and protracted deliberations inherent in investigating possible maltreatment, and take into account the overwhelming evidence that clinicians are reluctant to specify maltreatment, which education alone will not change.40 In the UK, HES coders should also record referral to children's social care services as this reflects a high level of concern and would provide a measure for auditing action. With these improvements, hospital administrative data have the potential to provide clinicians and policy makers with valuable insights into the burden and cumulative record of admissions related to maltreatment and to help clinicians to identify children who require experienced paediatric assessment, interventions and follow-up within healthcare, and/or social care support.
Acknowledgments
The authors are grateful to Brent Taylor, David Low, Rosalyn Proops, Ben Lloyd and Ian Maconochie, who contributed to the project through stakeholder meetings and commented on drafts of this report. Susan Charman advised on data management for HES, and Omar Bouamra and Tom Jenks provided data for TARN.
References
Supplementary materials
Web Only Data adc.2009.180216
Files in this Data Supplement:
Footnotes
-
Funding The study was funded by the Medical Directorate of the Department of Health for England. This work was undertaken at Great Ormond Street Hospital/University College London, Institute of Child Health which received a proportion of funding from the Department of Health's National Institute of Health Research (‘Biomedical Research Centres’ funding). The Medical Research Council provides funds for the MRC Centre of Epidemiology for Child Health.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.