Article Text

Abstract
Objective Because pharmacokinetic data are limited, continuous infusions of vancomycin in neonates are administered using different dosing regimens. The aim of this work was to evaluate the results of vancomycin therapeutic drug monitoring (TDM) under three different dosing regimens and to optimise vancomycin therapy.
Methods Vancomycin TDM concentrations were noted and compared prospectively in three hospitals. Population pharmacokinetic analysis was performed to optimise dosing using NONMEM software. Patient-tailored optimised dosing regimens were evaluated in a prospective study.
Results Two hundred and seven serum vancomycin concentrations from 116 neonates were analysed. Only 48 neonates (41%) had serum vancomycin concentrations within the therapeutic range of 15–25 mg/l using a current dosing regimen. Concentrations ranged from 5.1 to 61.5 mg/l. Loading doses were required to decrease the risk of sub-therapeutic levels during early treatment. An optimised dosing regimen, taking into account birth weight, current weight, postnatal age and serum creatinine, was developed based on a one-compartment pharmacokinetic model. A prospective validation study in 58 neonates demonstrated a higher percentage of neonates (70.7%, n=41) reaching the therapeutic range and early dosage adaptation (6–12 h post-dose) using an optimised dosing regimen.
Conclusions A patient-tailored optimised dosing regimen should be used routinely to individualise vancomycin continuous infusion therapy in neonates.
- Pharmacology
- Infectious Diseases
- Monitoring
- Pharmacokinetics
Statistics from Altmetric.com
What is already known on this topic
-
There is considerable inter-individual variation in the pharmacokinetics of vancomycin in neonates.
-
Pharmacokinetic data on vancomycin administered as a continuous infusion in neonates is limited.
What this study adds
-
Less than half the neonates had serum vancomycin concentrations within the therapeutic range with a current dosing regimen.
-
A loading dose of vancomycin is needed in neonates.
-
A new dosing regimen for the continuous infusion of vancomycin was developed and validated in neonates.
Introduction
After nearly 50 years of widespread clinical use, vancomycin remains the main antibiotic prescribed for the treatment of late-onset sepsis caused by coagulase-negative Staphylococci and methicillin-resistant Staphylococcus aureus (MRSA) in neonatal intensive care units (NICUs).1
The pharmacokinetics of vancomycin has shown wide inter-individual variability, particularly in neonates. Innovative strategies, such as modelling and a simulation approach, were initiated to individualise dosing of vancomcyin administered by intermittent infusion based on identified covariates (eg, weight, age, serum creatinine, etc).2 However, significant unexplained variability persisted and dosing adjustment based on therapeutic drug monitoring (TDM) is still mandatory to maximise the likelihood of achieving the desired therapeutic goal.1
Continuous infusion of vancomycin is an alternative option, but has been mainly studied in adults.3 ,4 Target concentrations were obtained more rapidly and there was less variability in the daily dose, although no difference in efficacy was demonstrated. Continuous instead of intermittent infusion is now used more frequently in neonates, although data are still limited.5–7 Different dosing regimens, with or without a loading dose and adaptation for weight, age and/or renal function, have been proposed. However, based on our experience, TDM remains mandatory to reach the target concentration of 15–25 mg/l and vancomycin dosage must be adjusted in most cases. As TDM is not standardised and has not been evaluated, the objectives of the present work are to evaluate the likelihood of achieving the target concentration with different dosing regimens, and to optimise vancomycin therapy in neonates.
Patients and methods
Neonates receiving vancomycin as a continuous infusion in one of three NICUs (Port Royal, Henri Mondor and Robert Debré Hospitals) between November 2010 and June 2011 were enrolled in the study.
The following information was prospectively collected: postmenstrual age (PMA; the sum of gestational age at birth and postmenstrual age), postnatal age (PNA), weight, patent ductus arteriosus (PDA), intrauterine growth restriction (IUGR), sepsis, ventilation, concurrent medication (such as inotrope, aminoglycoside or ibuprofen), vancomycin formulation, details of vancomycin administration, and serum creatinine. Patients with incomplete information were excluded. The study was conducted in accordance with the Declaration of Helsinki. The ethics committee (CPP, Comité de Protection des Personnes, Hôpital Saint Louis, île-de-France IV, Paris) agreed that this research project, which was based on monitoring, was exempt from obtaining informed consent.
Dosing regimen and sampling
Vancomycin (Sandoz, Levallois-Perret or Mylan, Saint-priest, France) was administered as a continuous infusion. The initial empirical dosing regimens were different in the three centres (table 1): two of them used a loading dose (10–15 mg/kg) and infusion rates ranged from 15 to 35 mg/kg/day. Vancomycin concentrations were monitored according to local clinical practice and dosing was modified to maintain a target concentration of between 15 and 25 mg/l at steady-state.
Dosing regimens in the three hospitals
Assay of serum vancomycin
The serum vancomycin trough concentrations were determined by immunoturbidimetric assay (hospital 2) and fluorescence polarisation immunoassay (hospitals 1 and 3). Both methods used a Cobas Integra system (Roche Diagnostics, Meylan, France). The lower limit of quantifications and coefficients of variation were 2 mg/l and <9.5% for the immunoturbidimetric assay, and 0.74 mg/l and <3.3% for fluorescence polarisation immunoassays, respectively.
Pharmacokinetic modelling
Pharmacokinetic analysis was carried out using the non-linear mixed-effects modelling programme NONMEM VI (V2.0; Icon Development Solutions, Ellicott City, MD, USA). The first order conditional estimation method with the interaction option was used to estimate pharmacokinetic parameters and their variability.
Covariate analysis followed a forward and backward selection process. Model validation was based on graphical and statistical criteria, including goodness-of-fit plots, bootstrapping, visual predictive checks (VPC) and normalised prediction distribution errors (NPDE). The detailed process of covariate analysis and model validation is described in the online supplemental file.
Dosing optimisation
The parameter estimates obtained from the model were used for vancomycin dosing optimisation. Initially, the concentration–time profiles of currently used and optimised dosing were predicted and compared in three typical neonates (preterm, median of the population and term). A hundred simulated trials were then performed using NONMEM. The simulation cohort consisted of the 116 neonates obtained from the original dataset, whose demographic characteristics were representative of patients in a neonatal clinical setting. A concentration of 20 mg/l was selected as the target for the purposes of this evaluation.
Clinical validation
The clinical feasibility and utility of a patient-tailored optimised dosing regimen with vancomycin continuous infusion was tested in a prospective validation study. In practice, personalised dosing was calculated with an Excel calculator which was developed using the pharmacokinetic parameters of the vancomycin model. The target concentration (mg/l) and patient information provided by the physician including birth weight (g), current weight (g), PNA (day) and serum creatinine concentration (µmol/l), were used to determine the personalised dose. The first TDM sample was taken 6–12 h after starting treatment. If the concentration did not fall within the desired therapeutic range of 15–25 mg/l, the dosage was adjusted as follows: adjusted dose (mg per 24 h)=last maintenance dose×(target concentration/last TDM vancomycin concentration).
Results
Concentrations of vancomycin delivered by continuous infusion were monitored in 116 neonates (59 boys and 57 girls) in the present study (table 2). A total of 207 samples were analysed including 116 first TDM measurements.
Baseline characteristics of 116 neonates in the original population pharmacokinetic study
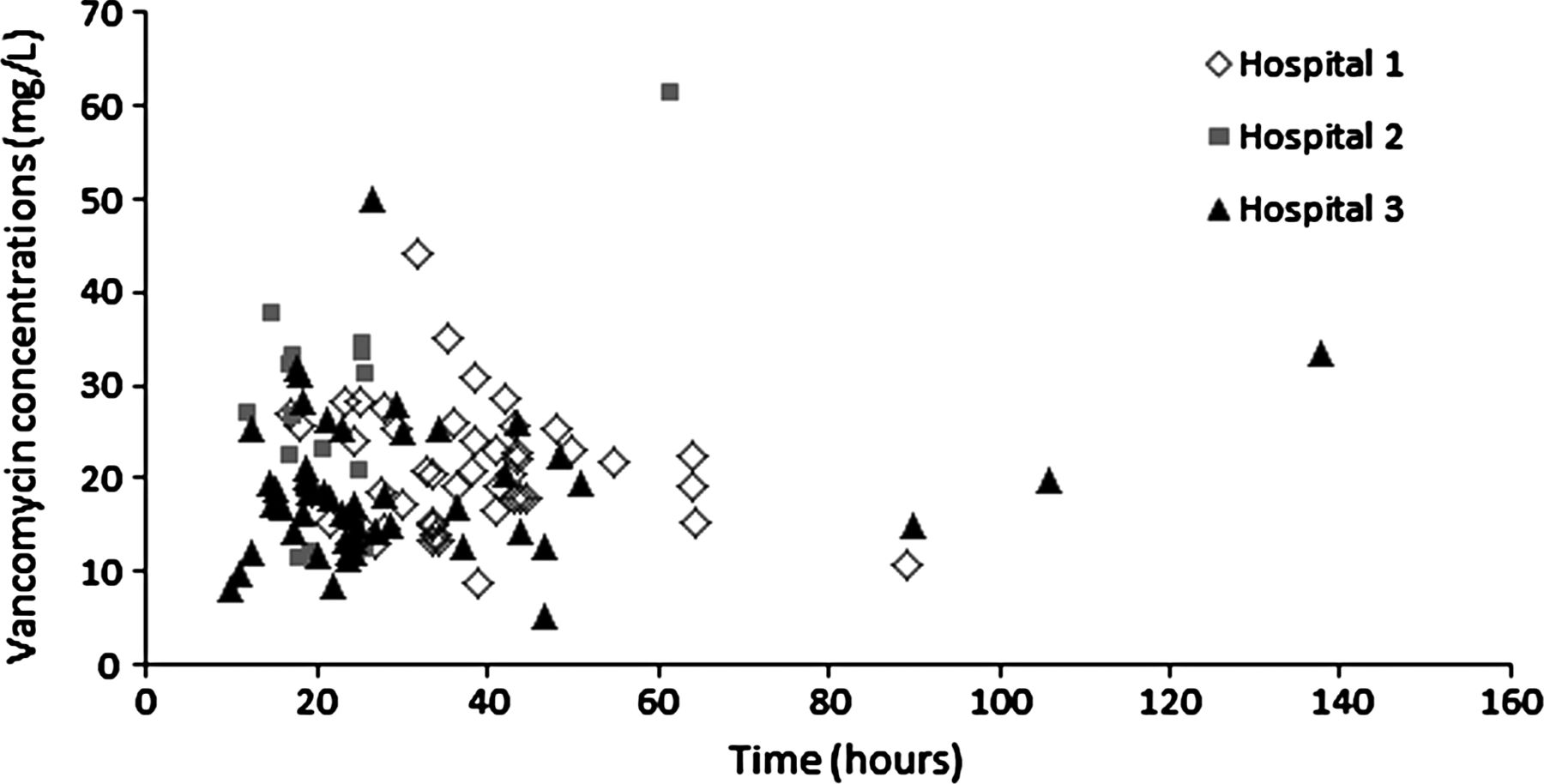
The concentration profiles of 116 first vancomycin TDM measurements under three dosing regimens are presented in figure 1. Blood samples were drawn at a median of 26.8 h (range 9.8–137.8 h) after initiation of treatment. The concentrations ranged from 5.1 to 61.5 mg/l. Only 48 neonates (41.4%) were within the therapeutic range of 15–25 mg/l, 35 had a low (<15 mg/l, n=30) or very low (<10 mg/l, n=5) serum vancomycin concentration and 33 had a high serum vancomycin concentration (>20 mg/l). Low concentrations were mainly observed with dosing regimen 3 (DR3), in which a loading dose was not used, while high concentrations were observed with DR2 using a uniform weight-based dosing regimen with a loading dose. After TDM adjustment, the percentage of neonates with extremely low (<10 mg/l) and high (>25 mg/l) measured concentrations decreased from 4% (n=5) to 1% (n=1) and from 28% (n=32) to 21% (n=24), respectively.

{kind=link}
Vancomycin first therapeutic drug monitoring concentrations (n=116).
Online supplementary figure S1 shows the correlation between first vancomycin TDM concentrations and PMA, weight and serum creatinine concentration in the three hospitals. Greater variability in vancomycin concentrations was seen in very preterm neonates. Vancomycin concentrations increased with increasing serum creatinine concentrations for the three dosing regimens and decreased with increasing PMA and weight (DR2 and DR3).
Pharmacokinetic modelling and model evaluation
Pharmacokinetic data fitted a one-compartment model with first order absorption and elimination. The systematic covariate analysis identified current bodyweight as the significant covariate implemented on volume of distribution (V), and birth weight, PNA and serum creatinine concentrations on clearance (CL). The model was validated by goodness-of-fit plots, bootstrapping, VPC and NPDE (see online supplementary figure S2). Detailed results of covariate analysis and model validation are described in the online supplemental file. The final population pharmacokinetic parameters are given in table 3.
Population pharmacokinetic parameters of vancomycin and bootstrap results (n=500)
Dosing optimisation
According to the final population pharmacokinetic parameters, optimised dosing was calculated as follow:
where V and CL are calculated using the equations developed from the model:


where current weight and birth weight is in g, PNA is in days and target concentration is in mg/l.
Concentration–time profiles of vancomycin for the three typical neonates following the three different dosing regimens currently used and the optimised dosing regimen were predicted on the basis of the final pharmacokinetic model (see online supplementary figure S3A). The currently used dosing regimens showed either increased vancomycin concentrations in preterm neonates, or low concentrations in term babies. These predicted results were in agreement with observed TDM results. Target concentrations are achieved in all three patients using the model-based optimised dosing regimen. Concentration–time profiles of vancomycin in 100 simulated clinical trials using an optimised dosing regimen are shown in online supplementary figure S3B. The simulated median concentration was close to 20 mg/l.
TDM sampling time
The median (range) first TDM sampling times in the three hospitals were 35.3 h (17.0–89.3 h), 19.5 h (12.0–61.7 h) and 23.8 h (9.8–137.8 h), respectively. Vancomycin concentrations were also simulated at 3 h, 12 h and 24 h after infusion began for the three currently used dosing regimens and the optimised dosing regimen. The percentage of simulated concentrations >25 mg/l and <15 mg/l are shown in online supplementary figure S4, which was in agreement with the simulation results in typical neonates and the observed results. The current dosing regimens showed a higher percentage of patients outside the target concentrations. With the optimised dosing regimen, a higher percentage of patients within the target concentrations was achieved. TDM, however, was still required due to large inter-individual variation.
Clinical validation
A total of 58 neonates participated in the clinical validation study (table 4). The target concentration was set to 20 mg/l for calculation of individual dosing. After receiving personalised doses, 41 neonates (70.7%) had concentrations within the desired therapeutic range of 15–25 mg/l. The mean of 58 first TDM concentrations was 20 mg/l (10th−90th percentiles: 12.8–26.5 mg/l). Nine neonates (15.5%) had concentrations <15 mg/l and eight (13.8%) concentrations >25 mg/l. After dosing adjustment, all neonates achieved the desired therapeutic range, except for three neonates who did not follow the protocol. In addition, the obtained concentrations did not show any significant correlation with covariates used to develop the dosing regimen (birth weight, current weight, PNA and serum creatinine).
Baseline characteristics of 58 neonates in the clinical validation study
Discussion
Vancomycin can be administered as either an intermittent or a continuous infusion. Continuous infusion has been mainly studied in critically ill adults and is recommended for two reasons: (1) it is the best way both to maintain serum concentrations above the targeted minimum inhibitory concentration (MIC) and to optimise efficacy, given the time-dependent effects of this antibiotic on bacterial kill rates; and (2) it makes monitoring of drug concentrations and dosage adjustment easier.8 When a continuous infusion was used, the target concentrations were obtained faster, resulting in fewer plateau concentrations measured during monitoring, less variability in the daily infused dose and reduced cost compared to intermittent infusion, although no difference in efficacy was revealed.3 ,4 Continuous infusion also has the potential benefit of decreasing the risk of adverse reactions, including nephrotoxicity.9
In the present study, the TDM results following different proposed dosing regimens with continuous infusion vancomycin were compared in neonates. Vancomycin's half-life is usually 3–10 h in neonates, depending on individual developmental and clinical characteristics.1 ,6 However, preterm neonates might need 30–50 h to reach therapeutic concentrations, which delay is too long for treating neonatal sepsis and obtaining early bactericidal efficacy. To overcome this problem, the loading dose strategy was recommended, which allows the therapeutic range to be reached more rapidly. Our results clearly support this approach, as the percentage of patients with low concentrations (<15 mg/l) was higher in hospital 3, where the loading dose strategy was not used. Given the variable and long half-life, the loading dose strategy may decrease the risk of sub-therapeutic levels during early treatment.
Various studies have shown that a vancomycin AUC0–24/MIC ratio of over 400 best predicts treatment outcomes for invasive MRSA infection in adults,10 and a similar drug level is sought in neonates. Many demographic, biological and clinical covariates have been reported to influence vancomycin pharmacokinetics,2 with weight, age and renal function having the greatest impact.11
As vancomycin is almost exclusively eliminated by the renal route, renal maturation (both anatomical and functional development) has an important influence on vancomycin dosing in neonates.1 ,12 ,13 It has been demonstrated that amikacin clearance is determined better by the combination of birth weight and PNA than PMA alone.14 Vancomycin is also primarily eliminated by the kidneys, and our results showed that clearance depended on the maturation of renal function and was better described by both antenatal (reflected by birth weight) and postnatal (reflected by PNA) parameters, taken into account separately. Renal function, as reflected by serum creatinine concentrations, was significantly and independently correlated with vancomycin clearance in the present study. The influence of residual maternal-derived creatinine seems to be limited in our study. Although eight neonates <3 days old were included, the relationship between vancomcyin clearance normalised by age and weight versus serum creatinine concentrations in these patients was similar to that in patients ≥3 days old (see online supplementary figure S5).
We were unable to demonstrate any significant effect of sepsis, ventilation, PDA, IUGR or concurrent medication.15 ,16 Clearly, their impact on neonatal development and maturation is complex, probably even more so in sick babies, but this study is probably underpowered to demonstrate their effect. Furthermore, their impact was probably limited as the large variability in concentrations was explained in the developed model by the combination of birth weight, current weight, PNA and serum creatinine concentration. Routine TDM could prevent potential toxicity or treatment failure in neonates with severe disease and unstable renal function.
On the basis of the final model, an optimised dosing regimen was developed for all neonatal age groups. The simulated clinical trial demonstrated good predictive performance for the developed models. The proposed personalised dosing regimen was evaluated in a prospective clinical validation study. According to the simulation and clinical practice, the first TDM sample can be taken 6–12 h after starting treatment. The results showed that the percentage of patients achieving the target concentrations of 15–25 mg/l increased to 70.7% using an optimised dosing regimen, compared to 41.4% using a current dosing regimen. The optimised loading dosing regimen, which takes into account birth weight, current weight, PNA and serum creatinine, resulted in a major improvement in individual vancomycin therapy in neonates. However, about 30% of neonates did not reach the target concentrations after the first dose due to residual and unexplained variability. These results suggest that additional clinical and physiological factors influencing variability should be considered and that routine TDM is still required. Indeed, after dosing adjustment based on the first TDM result, all neonates treated according to our protocol had concentrations in the desired target range.
Vancomycin has been on the market for more than 50 years. However, data on efficacy and/or safety are only available from observational studies.17 As our study was primarily a pharmacokinetic study, we did not collect efficacy and safety data on vancomycin continuous infusion. The next step might be to conduct a randomised controlled trial to compare continuous and intermittent administration of vancomycin. The clinical benefit of an optimal dosing regimen, based on a pharmacokinetic/pharmacodynamic endpoint, should also be evaluated.
Conclusion
Based on our population pharmacokinetic model, we evaluated a dosing regimen of vancomycin administered with a loading dose followed by continuous infusion. This prospective validation study demonstrated the good performance of an individualised patient-tailored optimised vancomycin dosing regimen in neonates.
Acknowledgments
We thank Daolun Zhang, Christophe Maritaz, Judith Toure, Michèle Rota and Jean-Claude Duché for assistance with research.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
- Data supplement 2 - Online figures
Footnotes
-
Contributors WZ and EJA had primary responsibility for protocol development, outcome assessment, data analysis and the writing of the manuscript. EL, VB, XD and MF participated in protocol development, patient enrolment and the writing of the manuscript.
-
Funding This work was supported by ‘la Foundation PremUp’ (Professor Danièle Evain Brion, France) and Global Research in Paediatrics—Network of Excellence (GRIP, EU-funded FP7 project, Grant Agreement number 261060).
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.