Article Text

Abstract
Objectives To estimate the incidence of clinically diagnosed congenital adrenal hyperplasia (CAH), clinical features and age at first presentation. To assess the potential benefit of newborn screening for CAH.
Design Active surveillance through the British Paediatric Surveillance Unit of all children aged under 16 years with newly diagnosed CAH, undertaken prospectively between August 2007 and August 2009. Twelve laboratories testing for CAH reported new diagnoses between August 2007 and January 2009. Reporting clinicians completed clinical questionnaires.
Setting England, Wales and Scotland.
Results 144 children with CAH were reported, of whom 132 (92%) had 21-hydroxylase deficiency. Thirty-six (25%) children were Asian and 62 (43%; 95% CI 35% to 51%) were boys. Incidence of new diagnoses in children ≤16 years was 0.60 (95% CI 0.50 to 0.71) per 100 000. Eighty-six (59%; 36 boys) children were diagnosed in the first year of life (estimated birth prevalence 5.48 (95% CI 4.42 to 6.81) per 100 000), most (77; 89%) of whom presented in the first month of life. Virilised genitalia were found in three-quarters of girls. Twenty-seven newborns first presented with salt-wasting crises, of whom 18 (67%; 16 boys) presented on or after 14 days of age.
Conclusions Approximately one child in every 18 000 born in Great Britain has CAH. Similar numbers of boys and girls present clinically in the first year of life, but boys present with more severe manifestations, such as salt-wasting crises. Around 70% of newborns who first present with salt-wasting crisis would be detected earlier through newborn screening.
Statistics from Altmetric.com
Background
Congenital adrenal hyperplasia (CAH) is the most common adrenal disorder in childhood affecting an estimated 1 in 10 000–20 000 live births. It is due to a group of recessively inherited enzyme deficiencies which affect cortisol production, characterised by decreased cortisol and aldosterone and excessive androgen production. The most common form of CAH is due to an absolute or relative deficiency in the activity of the enzyme 21-hydroxylase (CYP21A2) deficiency.
The salt-wasting form of CAH, affecting 66–75% of children with CYP21A2,1 2 may lead to a potentially life-threatening crisis within the newborn period. Boys are at an increased risk because, in comparison with girls, they are unlikely to be diagnosed as a consequence of genital virilisation. For girls, there may be difficulty at birth in assigning sex due to ambiguous genitalia and this can cause significant distress to families as has been demonstrated in the debate about prenatal treatment.3 In older children, untreated or unrecognised CAH may result in premature pubarche, accelerated bone maturation and potential fertility problems.4 5
What is already known on this topic
▶ Congenital adrenal hyperplasia is the most common adrenal disorder in childhood.
▶ Clinical presentation may include female genital virilisation and incorrect sex assignment, salt-wasting crisis, premature pubarche or accelerated growth.
▶ Incidence of congenital adrenal hyperplasia in the UK is uncertain and the ratio of girls to boys detected clinically may be changing due to greater awareness of the condition.
What this study adds
▶ Each year in Great Britain, around 70 children under 16 years of age are newly diagnosed with congenital adrenal hyperplasia.
▶ In the first month of life, most girls (77%) present with genital virilisation, while most boys (73%) present with salt-wasting crises.
▶ The timing of first clinical presentation suggests that almost 70% of babies presenting with salt-wasting crises could benefit from presymptomatic detection.
Early detection of CAH has the potential to benefit two specific groups: children who present neonatally with salt-wasting crises and those with simple virilising CAH who present with premature pubarche or accelerated growth. In contrast to other countries, the UK newborn screening programme, based on dried blood spots, does not currently include CAH. In 2003, based on evidence from two systematic reviews, the National Screening Committee concluded that screening should not be offered.6,–,8 This reflected uncertainty regarding disease burden as well as the false positive rate associated with the existing dissociation-enhanced lanthanide fluorescence immunoassay (DELFIA)screening test based on the biomarker 17-hydroxyprogesterone (17-OHP).
Contemporary information about the frequency and clinical presentation of CAH in the UK is lacking. Estimates of birth prevalence from previous UK studies of clinically presenting CAH vary from 1 in 6200 to 1 in 25 000.9,–,12 However, these are based in particular regions, involve small sample sizes and use varying definitions of CAH.
We investigated, prospectively, all new diagnoses of CAH in children under the age of 16 years in England, Wales and Scotland to estimate the incidence of clinically diagnosed CAH. Specifically, we examined sex and age-specific incidence of diagnosis, clinical features and time to presentation of those presenting clinically within the first month of life in order to assess the potential benefit of presymptomatic detection of CAH.
Methods
Active surveillance of newly diagnosed CAH was undertaken through the British Paediatric Surveillance Unit (BPSU)13 for 25 months (August 2007 to August 2009) in Great Britain (England, Wales and Scotland).
CAH was listed on the BPSU ‘orange card’ and sent out each month to participating paediatricians. Paediatricians were asked to notify any child under the age of 16 years who presented in the preceding month with clinical features of CAH and elevated 17-OHP (box 1). Study investigators sent paediatricians a questionnaire about each child notified.
Box 1 British Paediatric Surveillance Unit case definition
To maximise case ascertainment, children with CAH were also notified from August 2007 to January 2009 through a laboratory surveillance scheme comprising 12 UK laboratories which measure 17-OHP in children (Cambridge, Leeds, Liverpool, London,5 Manchester, Scotland, Southampton, Wales). Where possible, laboratory reports were matched to reports through the BPSU. When no match could be found among the BPSU reported cases, paediatricians caring for the laboratory-notified child were asked to complete the clinical questionnaire.
Date of birth, hospital number, sex and first half of current postcode were collected in order to identify duplicate case reporting. Clinical details requested were the date of first clinical presentation, symptoms and signs at presentation, including the Prader score for female virilisation,14 details of clinical management and diagnostic test results.
All notified children were reviewed by an expert diagnostic review panel (CK, PH) and categorised as ‘definite’ or ‘not’ CAH based on karyotype, presence or absence of salt-wasting, virilisation, and biochemical and molecular genetic test results.
We defined sex according to karyotype, except where sex was unambiguous and karyotyping not performed, when clinician-reported sex was used. Paediatricians reported ethnicity using UK Census 2001 categories15 grouped as white, black, Asian, mixed or other. CAH subtype was determined from the clinical information provided. The reason for clinical presentation was defined as the earliest presenting symptom precipitating investigation and diagnosis. The day of first clinical presentation was calculated by counting day of birth as day zero.
To calculate the incidence of diagnosis, the number of children confirmed as having CAH reported between September 2007 and August 2009 inclusive, were determined. Denominator data were obtained from the Office for National Statistics (ONS) mid-year population estimates for 2007 and 2008.
We grouped children into age-bands to calculate age-specific incidence and cumulative incidence of diagnosis (or risk of CAH diagnosis) for children up to 16 years of age with corresponding 95% CI.16 Standardised rate ratios were calculated for incidence of new diagnoses by country using the indirect method.17
Current UK newborn screening standards expect bloodspot samples to be taken 5 days after birth and screening results to be reported to clinical teams by day 14 of life.18 The proportion of children presenting in the first month of life who remained undiagnosed at day 14 were examined using Kaplan–Meier survival estimates, and the log-rank test used to test for differences between groups.19
Statistical and descriptive analyses were performed using StataSE11 (StataCorp). Ethical approval was obtained from Thames Valley Multi-centre Research Ethics Committee (07/MRE12/25) and the Patient Information Advisory Group (PIAG/BPSU 1-05(FT4)/2007).
Results
Case ascertainment
Paediatricians notified 275 possible CAH diagnoses to the BPSU during 25 months of surveillance and returned 260 questionnaires to the study investigators (95% response rate). Following review, 103 notifications were excluded because CAH was diagnosed before the surveillance period (n=12), the child was notified in error (n=28) or there were duplicate notifications (n=63). Questionnaires for the remaining 157 children were reviewed by the expert panel: 13 were deemed not to have CAH and 144 children concluded to have CAH (figure 1). These included eight children first identified through the laboratory surveillance scheme.

Flow diagram of case notifications to the study. BPSU, British Paediatric Surveillance Unit; CAH, congenital adrenal hyperplasia; DRP, Diagnostic Review Panel; FU, follow-up.
Among 144 children with CAH, the following subtypes were represented: CYP21A2 (n=132), 11-beta-hydroxylase (CYP11B1) deficiency (n=7), 3β-hydroxysteroid dehydrogenase (3β-HSD) deficiency (n=2) and steroidogenic acute regulatory protein (StAR)defect (n=1). For two children, insufficient clinical information was provided to allow determination of CAH subtype.
Incidence of newly diagnosed CAH
The incidence of new diagnoses of CAH in children under the age of 16 years was estimated to be 0.60 (95% CI 0.50 to 0.71) per 100 000 in Great Britain. Incidence did not vary significantly by country (table 1).
Annual incidence of newly diagnosed CAH in children aged under 16 years in UK
Sex and ethnicity
Although fewer boys (62; 43%) than girls (82; 57%) were diagnosed, this was not statistically significant (95% CI of the percentage of boys: 35% to 51%). Children of Asian ethnicity comprised 36/144 (25%) of all children with CAH and 24/86 (28%) of children notified in the first year of life.15 Ninety-six (66%) children were white, two (1%) black, seven (5%) of mixed or ‘other’ ethnicity, while three (2%) had no details recorded.
Age-specific and cumulative incidence of diagnosis up to 16 years of age
Age-specific rates were calculated by sex and age group. Estimates of annual cumulative incidence of CAH diagnosis up to but not including 16 years of age in Great Britain were calculated by sex. The incidence of diagnosis of CAH was highest in the first year of life; 5.48 (95% CI 4.42 to 6.81) children in 100 000 or 1 in 18 248 (table 2).
Annual age-specific incidence of diagnosis of CAH per 100 000 by sex
Clinical features and reason for presentation
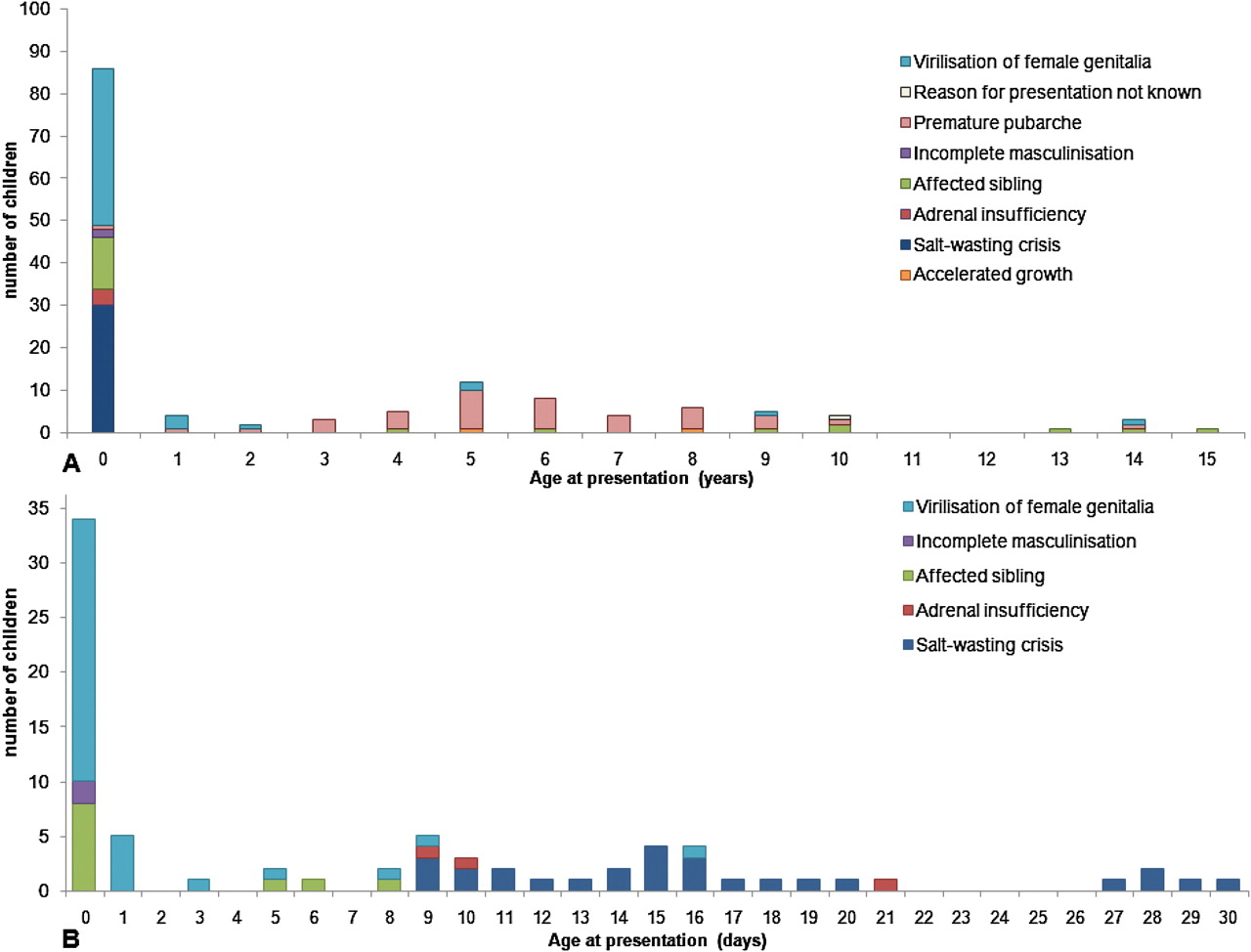
One of three clinical features usually precipitated investigation and diagnosis: virilisation of the female genitalia, premature pubarche or salt-wasting crises (figure 2A). Genital virilisation was present in over three-quarters of girls and salt-wasting crises were reported in a quarter of all children.

(A) Age and reasons for clinical presentation of congenital adrenal hyperplasia (CAH) in children aged under 16 years, (B) Age and reasons for clinical presentation of CAH in the first month of life.
Most children with CAH came to clinical attention in the first year of life (86 (36 boys); 59%). Twelve children (14%; 5 boys) were diagnosed due to an affected sibling, of whom three were diagnosed prenatally. Over three-quarters of those diagnosed in the first year of life presented with virilisation or salt-wasting crisis (38% and 38% respectively). One child died at 4 months of age from causes unrelated to CAH (secondary to respiratory distress at birth).
Children presenting within the first 30 days of life
The majority of children diagnosed before age one year presented during the first month (30 days) of life (77 (33 boys); 89%). Of nine children (3 boys, 6 girls) presenting after 30 days of age, three had a salt-wasting crisis (median age 52 days), two had virilisation, one had adrenal insufficiency, one was investigated following diagnosis in an affected sibling and one had premature pubarche.
For children presenting in the first month of life, the median age at clinical presentation was day of birth (IQR 0–1 days) for girls and 14 days (IQR 9–18 days) for boys. Of those presenting on the day of birth, 91% (31/34; 3 boys) were of the CYP21A1 subtype.
Median age at presentation varied by reason for clinical presentation (table 3). Most girls (34/44; 78%) were suspected to have CAH within the first day of life due to genital virilisation. Difficulties in initial sex assignment were reported for 20 (24%) children, including two boys. Among 27 newborns who presented with a salt-wasting crisis, the earliest salt-wasting crisis was 9 days after birth, and 18 babies (67%; 16 boys and 2 girls) presented on or after day 14 (figure 2B). The probability of being diagnosed on any day during the first month of life is compared for all boys and girls diagnosed before 1 year of age (figure 3). While girls were diagnosed soon after birth, as shown by the initial steep fall in the number of undiagnosed cases, boys were significantly less likely to be diagnosed at any time point (log-rank test; p<0.0001). By day 14, when newborn screening results should be available, only 6% of girls compared with 50% of boys remained undiagnosed.

{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier plot of probability of remaining undiagnosed in children presenting with congenital adrenal hyperplasia in the first month of life by sex. Note: The dotted lines at days 5 and 14 represent the ages at which current NHS screening programme standards state that a newborn screening sample should be taken and reported to clinical management teams, respectively.
Median age and reason for clinical presentation in children presenting in the first month of life (30 days)
Discussion
In Great Britain, approximately 70 children present clinically with CAH each year. On average, one child in every 18 000 born will be diagnosed with CAH in the first year of life, with the majority diagnosed on the first day of life. Similar birth prevalence rates based on clinical detection have been reported in other countries, such as Australia and the USA.20 21 Although 28% of children presenting with CAH under 1 year of age were of Asian origin, only 9% of births in England and Wales are to parents of Asian ethnicity.22
We found the most frequent clinical presentations of CAH in the first year of life were salt-wasting crises and virilisation of female genitalia. The mode and timing of presentation were distinct for each sex, and boys presented with more severe manifestations in infancy, such as salt-wasting crises. In contrast to boys, most girls presented with genital virilisation and were detected within the first day of life. Although there were fewer boys diagnosed, we did not find a significant sex difference as observed in previous studies.9 23 24 However, our data are consistent with a West Midlands study25 which suggested that recognition of affected boys might be improving due to increased clinical awareness of CAH in recent years.
Newborn screening offers the potential to avoid severe clinical presentations of CAH, in particular salt-wasting crises. In our study approximately one-quarter (18/77 (23%); 16 boys) of all children presenting with CAH in the first month of life presented with a salt-wasting crisis after 14 days of age. Although nine children (eight boys, one girl) presented with crises before day 14, none presented before day 9. These findings have implications for the timeliness of newborn screening results, and must be carefully considered in the context of other conditions included within the UK newborn bloodspot screening programme.
This is the first epidemiological study of CAH through the BPSU across three countries using the BPSU's prospective, active surveillance methodology which has a high (94%) response rate by paediatricians and has been used for 25 years to study over 50 conditions, including four endocrine disorders.13 Furthermore, positive dependence in case-reporting between the BPSU and laboratory systems26 led to additional cases being notified in this study. Our study used a broad case definition of CAH that encompassed reporting of rarer subtypes. An expert review system independently verified diagnoses based on the clinical features and diagnostic test results reported by paediatricians. It is important to assess the burden of these rarer subtypes as some, such as CYP11B1 deficiency, are detectable by screening dried blood spots for the 17-OHP biomarker commonly used to test for CYP21A2.
We acknowledge that our study only includes children brought to clinical attention, thus it may have underascertained asymptomatic or mild cases, and we were unable to investigate prenatal diagnosis of CAH and pregnancy terminations. We could not directly evaluate under ascertainment of cases through the BPSU as the laboratory surveillance was not an independent reporting source and was used to identify late reporting by paediatricians as well as potentially unreported cases. Although we found no deaths due to CAH in contrast with previous reports,27 28 surveillance through the BPSU may not detect children who die before diagnosis, especially if postmortem investigations are not performed.
In comparison with a surveillance study using equivalent methodology in Australia, which estimated CAH incidence at 1 in 18 034 births in states without newborn screening, we report similar estimates of newly diagnosed CAH.20 Importantly, ethnicity was not reported for the Australian study and is likely to differ from the British population. In the Australian state which performed newborn screening for CAH, the incidence was estimated at 1 in 15 488 births and recent estimates of CAH incidence in countries with newborn screening are also higher than our estimate based on clinical detection.29,–,31 Such a difference could be explained by the proportion of children that die without diagnosis1 or remain undiagnosed with mild disease in populations without newborn screening for CAH.
In addition to the lack of contemporary estimates for the incidence of CAH, a significant barrier to the introduction of newborn screening for CAH in the UK has been reports of a high number of false positive results from international programmes based on DELFIA assay for the biomarker 17-OHP.32,–,35 Alternative methods, such as liquid chromatography-tandem mass spectrometry and second-tier testing have demonstrated a potential to reduce false positive results.32 36,–,39 Nevertheless the implications of applying these methods to a screening programme within the UK healthcare context would require careful consideration.
This study describes the features at presentation, subtypes and incidence of newly diagnosed CAH in childhood in the multi-ethnic population of Great Britain. Similar numbers of boys and girls present within the first year of life; however, children of Asian ethnicity appear to be over-represented. The potential for presymptomatic detection to prevent severe manifestations of CAH is greatest for boys who would otherwise be more likely to first present with salt-wasting crises. The avoidance of these episodes, which can result in neurological damage and intellectual disability or death, is important in making the case for newborn screening for CAH; however, children who present later with irreversible effects may also benefit.40
Acknowledgments
We thank Mr Richard Lynn and Helen Friend and reporting clinicians of the BPSU for their help with data collection. We are grateful to British Society of Paediatric Endocrinology and Diabetes and Living with CAH (formerly Climb-CAH) for supporting this study. This work was undertaken at Great Ormond Street Hospital/UCL Institute of Child Health which received a proportion of funding from the Department of Health's NIHR Biomedical Research Centres funding scheme. The Centre for Paediatric Epidemiology and Biostatistics also benefits from funding support from the Medical Research Council in its capacity as the MRC Centre of Epidemiology for Child Health (Grant Reference: G04005546). We acknowledge the BPSU, supported by the Department of Health, for facilitating the data collection and all the reporting clinicians. The views expressed in this publication are those of the authors and not necessarily those of the Department of Health or BPSU.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
-
Funding The UK Collaborative Study of Newborn Screening for CAH was funded by a grant from the Department of Health (England) and commissioned by the UK National Screening Committee.
-
Competing interests None.
-
Ethics approval This study was approved by the Thames Valley Multi-centre Research Ethics Committee (07/MRE12/25) and the Patient Information Advisory Group (PIAG/BPSU 1-05(FT4)/2007).
-
Provenance and peer review Not commissioned; externally peer reviewed.