Article Text

Abstract
Objective To examine whether breast feeding is associated with behavioural development in children aged 5 years.
Design The authors used data from a large, prospective, nationally representative UK cohort, the Millennium Cohort Study.
Participants 10 037 mother–child pairs from white ethnic background (9525 term and 512 preterm children) were included in the analyses.
Methods Duration of breast feeding (at all or exclusively) was ascertained from parental interview at study baseline, when the children were aged 9 months. Child behaviour was assessed using a parent-completed questionnaire, the Strengths and Difficulties Questionnaire (SDQ). The authors used logistic regression to investigate the associations of breastfeeding duration with abnormal parent-rated SDQ total and subscores at age 5 in term and preterm children separately.
Results Abnormal SDQ scores were less common in term children (n=1129/9525, 12%) than pre-term (n=78/512, 15%) children. Term children breast fed for 4 months or longer (n=2741/9525, 29%) had lower odds of an abnormal total SDQ score (multivariable-adjusted OR compared with never breastfed children (n=3292/9525, 35%) 0.67, 95% CI: 0.54 to 0.83). This effect was similar for all the SDQ subscores. In preterm children, longer duration of breast feeding was generally associated with lower odds of abnormal SDQ total and subscores but the effect estimates were imprecise. The associations between exclusive breast feeding and abnormal SDQ scores were similar to those of any breast feeding and abnormal SDQ scores.
Conclusions The findings suggest that, at least in term children, longer duration of breast feeding is associated with fewer parent-rated behavioural problems in children aged 5 years.
Statistics from Altmetric.com
Introduction
Few large prospective studies of the association between infant feeding and child behaviour have been undertaken and overall these studies have had inconsistent findings. In some studies, the researchers have reported breast feeding being associated with child behaviour even after adjustment for potential confounders, whereas in others the associations attenuated considerably with adjustment for socioeconomic and parental factors.1,–,4 Some inconsistent findings may relate to the relatively small number of participants in many studies as well as inadequate adjustment for potential confounders. Furthermore, the relationship of breast feeding with child behaviour may differ according to gestational age at birth, because infant feeding5 and problems in many areas of behaviour6 differ in preterm and term children.
What is already known on this topic
▶ In most observational studies, breastfed children have had fewer behavioural problems than formula-fed children.
▶ This difference has attenuated or disappeared with adjustment for socioeconomic and other potentially confounding factors, suggesting that it has been largely due to confounding.
What this study adds
▶ In our large prospective study of singleton, white UK children, breast feeding for 4 months or longer was associated with lower odds of behavioural problems at 5 years.
▶ In term children, this association remained after adjustment for a large number of potential confounders.
Children learn appropriate behaviour from people around them and during the learning process all children sometimes behave inappropriately, for example, have temper tantrums or are aggressive. Behavioural problems, however, are inappropriate behaviours that occur repeatedly over a period of time, have a negative impact on the child's development and interfere with the child's or their family's everyday life.7 Behavioural problems can constitute emotional symptoms (eg, clinginess, anxiety), hyperactivity (eg, restlessness) or conduct problems (eg, lying, stealing).8 Infant feeding could influence child behaviour through biological or psychosocial mechanisms. It is possible that increased intake of essential fatty acids from breast milk leads to improved neurological development and behavioural learning and thus fewer behavioural problems.2 Breast feeding may also lead to more mother–baby interaction and better communication,9 thus improving behavioural learning and development.10
In order to better understand the associations of infant feeding with child behaviour, we examined whether the duration of breast feeding (at all or exclusively) was associated with parent-rated measures of behavioural development, the Strengths and Difficulties Questionnaire (SDQ) scores in children aged 5 years, using data from a large, prospective, nationally representative UK cohort, the Millennium Cohort Study (MCS).
Methods
The Millennium Cohort Study
The MCS is a survey of infants born in the UK during a 12-month period in 2000–2001. Details of the study's design and data collection have been reported previously.11 12 Briefly, the MCS is a clustered, stratified sample of households identified from the UK government Department of Work and Pensions Child Benefit records. The households invited to participate were selected on the basis of residential location immediately after the birth of the would-be cohort child. The sample was clustered at the electoral ward level and economically disadvantaged wards and wards with large proportions of ethnic minority residents were over-sampled. The baseline data were collected by trained interviewers, who visited the participating households when the cohort children were 9 months old (Sweep 1). Since the baseline interview, participating households have been followed-up with home interviews at approximately 2-year intervals. The MCS was approved by the London Multicentre Research Ethics Committee.
Participants
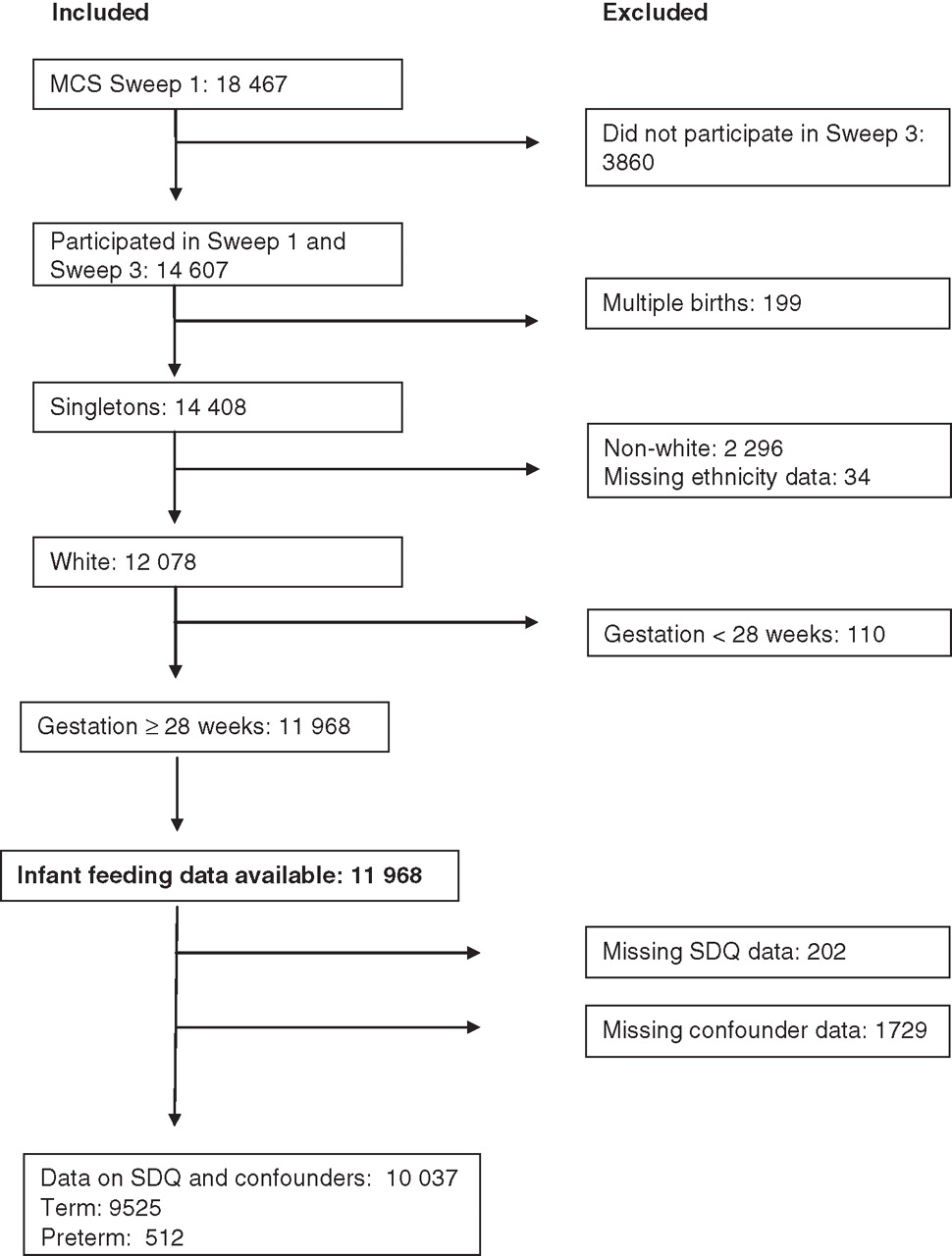
Our analyses comprised mother–child pairs who participated at Sweeps 1 (when the children were aged 9 months) and 3 (when the children were aged 5 years). We excluded mother–child pairs from non-white and mixed ethnic groups because a considerable proportion (36–41%) of mothers in these groups did not respond to the SDQ. We also excluded twins and triplets because their behavioural development differs from singleton children.13 14 Children born extremely prematurely (before 28 weeks of gestation) were excluded because their complicated feeding during the first months may not have been adequately captured in the MCS. We also excluded mother–child pairs with missing data on infant feeding, SDQ or potential confounders. A total of 10 037 mother–child pairs with complete data on SDQ and all potential confounders were included in our analyses. Of these children, 9525 were born at term (≥37 weeks of gestation) and 512 were born preterm (born before the 37th gestational week) (figure 1).
{kind=link}
Participant flow chart. MCS, Millennium Cohort Study; SDQ, Strengths and Difficulties Questionnaire.
Exposure and outcome ascertainment
Breastfeeding initiation was ascertained from the Sweep 1 interview question ‘Did you ever try to breastfeed your baby?’ Breastfeeding duration was ascertained from Sweeps 1–3 questions on the age when the cohort child was last given breast milk and when first given formula, other types of milk and solids. Breast feeding was defined as exclusive if the infant had received only breast milk, and no other milk, solids or fluids other than water.
Behavioural problems were assessed at Sweep 3 using the SDQ completed by the child's parent, usually the mother. The SDQ, which consists of 25 informant-rated statements in five areas of a child's behaviour, is a validated reliable instrument for identifying children with behavioural problems in clinical as well as community settings.8 15 16
Details of the ascertainment of breast feeding and behavioural problems are provided in online supplementary appendix 1.
Statistical methods
Exposures and outcomes
All analyses were conducted separately for term and preterm children because there is evidence that infant feeding and behavioural outcomes differ in these groups.17 18 Breastfeeding duration (at all or exclusively) was categorised into never, <2.0 months, 2.0–3.9 months and ≥4.0 months for the term children. These categories were chosen based on the UK infant feeding guidelines at the time of the study baseline, which recommended introducing solid foods after 4 months of age.19 For the preterm children breastfeeding duration was categorised into never, ≤2.9 months and ≥3.0 months because the number of preterm children in our study was too small to be split into further categories (table 1).
Participant characteristics
We calculated SDQ subscores by adding up the relevant question scores and the total SDQ score using the standard method, by adding up the subscores bar—the prosocial score.15 We defined abnormal SDQ scores using cut-off points (shown in tables 2–4), which corresponded to approximately 90th percentile of the distribution of the SDQ scores in our study population and which have been identified in previous studies as differentiating between abnormal and normal scores in 5-year olds in low-risk populations.15 20 We also conducted sensitivity analyses modelling the SDQ scores as continuous outcomes.
Summary of the association of breast feeding and abnormal total SDQ score
Summary of the associations of breast feeding and abnormal SDQ subscores in term children (n=9525)
Summary of the associations of breast feeding and abnormal SDQ subscores in preterm children (n=512)
Potential confounders
We adjusted our models for a set of a priori confounders and a set of additional potential confounders. A priori confounders were factors which previous research has shown to be associated with breast feeding and child behaviour.1 21,–,24 Additional confounders were factors which could plausibly be confounders and which, when added to the models including the a priori confounders, changed the main effect estimates by 5% or more. Details of the ascertainment of the potential confounders have been reported previously19 25 26 and are provided in online supplementary appendix 1. Briefly, a priori confounders were household socioeconomic position (SEP),27 mother's mental health (Malaise Inventory and Kessler scales)28,–,30 and mother's age, education, smoking during pregnancy and relationship status and baby's admission to a neonatal unit. Additional potential confounders were mother–baby attachment (Condon scale),31 baby's birth order, mother's alcohol use during pregnancy,26 type of childcare the child attended and age when the child started childcare.
Models
We used logistic regression to investigate the associations of breast feeding with abnormal SDQ scores and ran unadjusted, a priori adjusted and fully adjusted (a priori + additional confounders) models for each exposure-outcome pair. Stata's survey commands with Sweep 3 sampling weights were used to adjust for the unequal probability of the participants being included in the study and the attrition between Sweeps 1 and 3. All analyses were conducted using Stata SE 10.1 (Stata Corporation, College Station, Texas, USA).
Results
Participants
The characteristics of the children in our study are summarised in table 1. Breastfeeding initiation was equally common in term and preterm children (65% in both groups). Twenty-nine per cent of term children and 21% of preterm children were breast fed for at least 4 months (mean duration of breast feeding in this category was 9.8 and 9.6 months, respectively). A larger proportion of preterm (15.2%) than term children (11.9%) had abnormal total SDQ scores.
Associations of breast feeding and SDQ scores in term children
The associations of breast feeding with having an abnormal total SDQ score are summarised in table 2. In term children, breast feeding was associated with lower odds of an abnormal total SDQ score (table 2) and subscores (table 3) in the unadjusted analyses. Adjustment for a priori confounders attenuated the ORs of breast feeding for <2.0 months (n=2580, 27%) or 2.0–3.9 months (n=912, 10%) to the null. However, term children breast fed for 4 months or longer (n=2741, 29%) had lower odds of an abnormal total SDQ score even after adjustment for potential confounders. The associations of any and exclusive breast feeding with total SDQ scores were similar in direction and magnitude. There was no clear evidence of any SDQ subscore driving these associations (table 3) and although the point estimates suggest associations of breast feeding with fewer behavioural problems, there were no consistent trends across the breastfeeding duration categories. After adjustment for potential confounders, exclusive breast feeding for 4 months or longer was associated with lower odds of abnormal emotional and conduct scores. The associations of breast feeding and hyperactivity, peer problems or prosocial scores varied from positive to negative.
Associations of breast feeding and SDQ scores in preterm children
In the unadjusted analyses, having been breast fed for 3 months or longer (n=133, 26%) was associated with lower odds of an abnormal total SDQ score (table 2) and subscores (table 4) in preterm children (n=512). However, adjustment for potential confounders considerably attenuated these effect estimates. The associations of any and exclusive breast feeding with SDQ subscores were similar in direction and magnitude. We were unable to estimate the effect of breast feeding on emotional and prosocial subscores in preterm children due to small numbers of children with abnormal scores (n=21 and 8, respectively).
The results in the sensitivity analyses with SDQ scores as continuous outcomes did not differ from the main findings presented here.
Discussion
Associations of breast feeding with SDQ scores
Overall, our findings that abnormal SDQ scores were less common in breastfed than formula-fed children were similar to those in many previous studies.2 In our study, adjustment for potential confounders attenuated the association of breast feeding and child behaviour to the null in term children breast fed for less than 4 months. However, term children breast fed for 4 months or longer had lower odds of abnormal total SDQ scores independently of socioeconomic factors, mother's mental health, mother–baby attachment or early childhood exposures. These findings were consistent for any breast feeding and exclusive breast feeding as the exposures. There was no clear evidence of any SDQ subscore driving these associations, although the point estimates suggest associations of breast feeding with fewer behavioural problems. However, these subgroup analyses should be interpreted with caution, because they were inconsistent across the categories of breastfeeding duration. We are not aware of evidence for a threshold effect of breast feeding for 4 months or longer and our findings may relate to breast feeding for this long being relatively uncommon in the UK. In 2000, about 29% of infants in England were still being breast fed at the age of 4 months.32 Thus, these children may be growing up in families that are different from formula-fed children's in terms of parenting or other unmeasured confounders.
In preterm children, longer duration of breast feeding was generally associated with lower odds of abnormal SDQ total and subscores. Although the point estimates in our adjusted analyses suggest a beneficial effect of breast feeding on behaviour, their 95% CIs cross the null value and thus do not rule out the possibility of an adverse effect or no association. This may be due to lack of power, as the numbers of preterm children in our cohort were relatively small. Another explanation could be that preterm children are a heterogeneous group in terms of infant feeding and other health exposures and outcomes, and while breast feeding may be associated with improved behavioural development in some preterm children, the association is not apparent in this group as a whole.
Potential mechanisms
One explanation for the association of breast feeding with child behaviour is that breast milk contains large amounts of essential long chain polyunsaturated fatty acids (LCPUFAs), growth factors and hormones, which have an important role in the development and function of the brain and central nervous system.2 33 Up to about a decade ago, formula milks were not supplemented with fatty acids and it is thus possible that the associations of breast feeding with child behaviour in the older studies reflect better neurological development in breastfed than formula-fed children. However, in the past decade many formula milk manufacturers have begun supplementing formulas with essential fatty acids.34 The evidence for effectiveness of the supplementation is unclear,35,–,37 but it is likely that the formula-fed children in our study received supplemented formulas. If LCPUFAs are the mechanism linking infant feeding and child behaviour, this would have diluted any associations.
Another mechanism could be that breast feeding leads to more interaction between the mother and the child, better learning of acceptable behaviours and fewer behavioural problems.10 However, in our analyses of term children, having been breast fed for 4 months or longer was associated with fewer behavioural problems independently of indicators of mother–baby interaction (Malaise Inventory, Condon and Kessler scales, birth order and type and duration of childcare), suggesting that the effect was not mediated by these factors. A further potential mechanism could be that formula feeding is associated with infections and hospitalisations during infancy,19 38 39 which could lead to behavioural problems in children, perhaps due to time spent separated from the parents.
Strengths and limitations
Important strengths of our investigation are that we used a large prospectively collected dataset and adjusted our analyses for a large number of potential confounders, most notably mother's age and education and household SEP. However, it is possible that our findings have been influenced by residual confounding from unmeasured confounders.
Breastfeeding duration in the MCS was ascertained from interviews with the mother. Although there is evidence that maternal recall is a valid and reliable method of ascertaining breastfeeding initiation and duration,40 some bias may have resulted from poor recall or desire to give the interviewer a socially acceptable answer. Also, there may have been some misclassification of breast feeding in preterm children and children in the shortest breastfeeding duration categories. For example, the mothers of some infants, particularly of those admitted to neonatal intensive care units, may have reported that they never breast fed even if their babies received expressed breast milk from the mother or a donor. Also, the shortest breastfeeding duration category included some infants who only received breast milk for a few weeks or days. Such recall bias and exposure misclassification may have led to an underestimate or overestimate of the effect of breast feeding, as well as reduced the accuracy of the effect estimates. Due to the small number of preterm children in our study, we were unable to use the same categorisation of breastfeeding duration for term and preterm children and any comparison of effects between these groups should be done with caution. Furthermore, no information was collected on types of formula milks.
Our findings are generalisable to white singleton children in the UK. Further studies would be needed to investigate whether these findings replicate in multiple births, extremely premature children and children from other ethnic backgrounds. One way to examine this would be to pool data from existing studies in these groups, for example, by using individual-participant meta-analysis.
Conclusions
Our findings suggest that longer duration of breast feeding (at all or exclusively) is associated with having fewer parent-rated behavioural problems in term children. The evidence for an association between breast feeding and behavioural problems in preterm children was unclear.
Acknowledgments
The authors would like to thank the MCS families for their cooperation in the study and the MCS study team at the Institute of Education, where the MCS data are deposited.
References
Supplementary materials
Web Only Data adc.2010.201970
Files in this Data Supplement:
Footnotes
-
Funding This paper reports on an independent study which was funded by the Policy Research Programme in the Department of Health, UK. The views expressed are not necessarily those of the Department. The MCS was funded by the Economic and Social Research Council, UK. KH and MAQ were funded by the Department of Health. AS and YK were funded in part by the UK Economic and Social Research Council Centre for Lifecourse Studies in Society and Health (grant number RES-596-28-0001). MJR was funded by the University of York.
-
Competing interests None.
-
Ethics approval The Millennium Cohort Study was approved by the London Multicentre Research Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.