Article Text

Abstract
Objective: Most babies receive at least some formula milk. Variations in formula-feeding practices can have both short- and long-term health consequences. The literature on parents’ experiences of bottle-feeding was systematically reviewed to understand how formula-feeding decisions are made.
Methods: Relevant English-language papers, identified by searching 12 electronic databases, reference lists and related articles and by contacting first authors of included papers, were systematically searched for and appraised. The included studies were analysed and synthesised using a combination of narrative and thematic approaches. Consensus on the final inclusion, interpretation and synthesis of studies was reached across the research team.
Results: Six qualitative studies and 17 quantitative studies (involving 13 263 participants) were included. Despite wide differences in study design, context, focus and quality, several consistent themes emerged. Mothers who bottle-fed their babies experienced negative emotions such as guilt, anger, worry, uncertainty and a sense of failure. Mothers reported receiving little information on bottle-feeding and did not feel empowered to make decisions. Mistakes in preparation of bottle-feeds were common. No studies examined how mothers made decisions about the frequency or quantity of bottle-feeds.
Conclusions: Inadequate information and support for mothers who decide to bottle-feed may put the health of their babies at risk. While it is important to promote breastfeeding, it is also necessary to ensure that the needs of bottle-feeding mothers are met.
Statistics from Altmetric.com
Breastfeeding is unanimously recognised as the optimal way to feed babies, with many benefits to mother and child.1 However, despite the worldwide increase in governmental, institutional and professional support for breastfeeding—for example through the Unicef Baby Friendly Initiative2—repeated surveys show that the vast majority of babies receive at least some formula (“bottle”) milk in the first year of life.3 While it is important to promote breastfeeding, the needs of mothers who decide to bottle-feed their babies should also be considered.
The 2005 Infant Feeding Survey showed that while 78% of mothers in England initiated breastfeeding, only 45% of babies were exclusively breastfed at 1 week of age; this proportion dropped to 21% at 6 weeks of age and to less than 1% at 6 months of age.3 Importantly, the survey also highlighted that almost half of mothers who prepared powdered infant formula did not follow key recommendations, which are intended to reduce the risk of infection and overconcentration of feeds. Similarly, a systematic review on formula-feed preparation published in 2003 identified five studies that all reported a high frequency of errors in reconstitution.4 In addition to these short-term health risks, a higher calorie intake and rapid weight gain during infancy have been shown to predispose to later obesity.5–7
Mothers who formula-feed their babies have been studied extensively, but largely in the context of identifying their reasons for not breastfeeding in order to develop interventions to promote breastfeeding.8 In order to support the development of interventions to optimise the delivery of formula milk feeding, we therefore performed a systematic review of the available evidence on parents’ experiences of infant formula-feeding. Within this overall review question, we specifically aimed to identify their views regarding sources of information and support for formula-feeding, how feeds were prepared and how they made decisions regarding the quantity and frequency of feeding.
METHODS
Search strategy
We searched 12 electronic literature databases for English-language publications from their inception date up to March 2008. The search strategy included free text and, where possible, thesaurus mapping for key terms “bottle, formula, artificial, infant, feeding, feeds, milk, breast-milk-substitutes” and “perception, experience, knowledge, information, preparation, prepare, quantity, view, belief, believe.” Plurals and all synonyms were included (further details of the search strategy are in supplementary materials table 1). The search syntax was deliberately sensitive rather than specific in order to retrieve the maximum number of articles. All citations were exported to a Reference Manager database and relevant studies were identified by scanning titles and abstracts in a two-stage process. We also searched selected on-line journals (Annals of Anthropology, Archives of Diseases in Childhood, Journal of the American Dietetics Association, Journal of Advanced Nursing, Journal of Pediatrics and Child Health, Midwifery and Pediatrics) using the terms “formula feeding” and “bottle feeding.” We performed citation-tracking, related-article and reference-list searches on all included papers and contacted first authors to identify additional published or unpublished studies.
Study selection and exclusion criteria
Since we wanted to capture the bottle-feeding experiences of parents, we excluded studies where the focus was on comparing different types of formula, comparing health outcomes in breast- versus formula-fed babies, formula-feeds and HIV prevention, or formula-feeding in preterm or low-birthweight babies. In order to perform a synthesis of studies conducted in a similar context, we restricted our review to studies carried out in developed countries.
Data extraction and quality appraisal
Data extraction and quality appraisal were performed by one of the authors (RL) and verified by DO or KO, any disagreements being resolved by discussion within the review team. The quality criteria used were developed by Atkins et al9 adapted from the CASP assessment tool for qualitative studies.10 There is much debate as to whether quality criteria can be applied to the meta-synthesis of qualitative studies,11 12 and some researchers consider the application of such criteria to be excessively reductionist.13 We therefore decided a priori not to exclude any relevant studies on the basis of the quality assessment. For the purposes of this review, we classified studies in which it was possible to explore views and opinions as qualitative (eg, those using in-depth interviews, focus groups or participant observation) and others as quantitative (eg, those using surveys, review of clinical notes or objective measurement).
Data synthesis
Since the studies we identified used different approaches in quantitative and qualitative research, and methods for systematically reviewing such bodies of literature are still evolving,14 15 we performed both textual narrative and thematic analyses. For the textual narrative analysis, we tabulated the study characteristics, key findings and conclusions of individual studies. For the qualitative studies, thematic synthesis was performed in three stages as recommended by Thomas and Harden.16 In stages 1 and 2, we coded the text and developed the “descriptive themes.” Directly reported participant quotes (first-order constructs) and author interpretations (second-order constructs) were recorded separately, to retain the richness or “thickness’ of the data. Greater weight was given to directly reported quotes. In stage 3, we used our original review questions to develop the “analytical themes” and added data from the quantitative studies to strengthen the analysis.
RESULTS
Studies identified
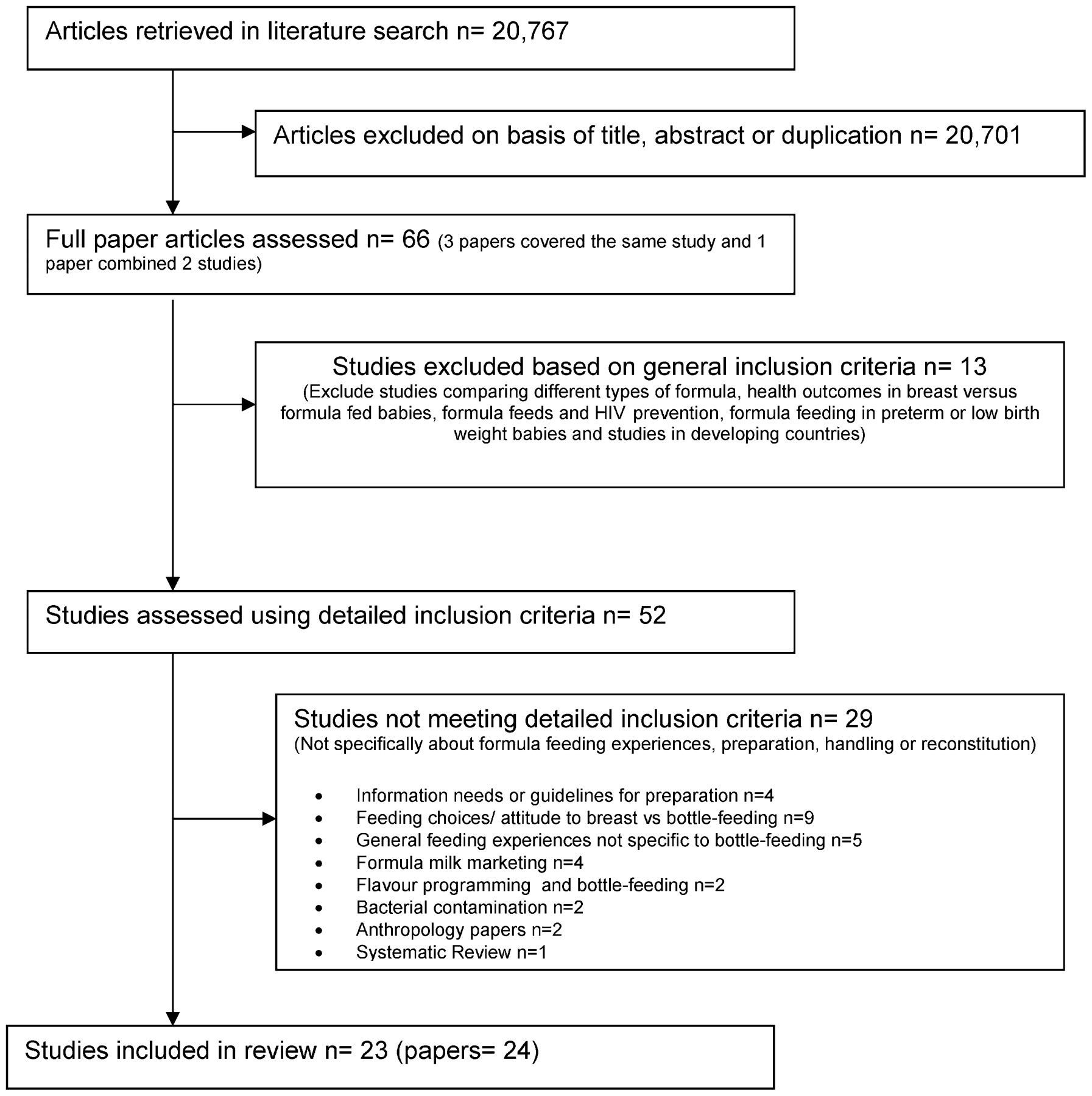
We screened 20 767 references, retrieved 66 potentially relevant full-text articles and finally selected 23 studies for inclusion in the review (fig 1). The studies were heterogeneous in their design, context, focus and quality (see supplementary materials tables 2–4). There were six qualitative studies17–22 (involving 145 participants) and 17 surveys or quantitative studies3 21 23–39 (19 papers involving 13 118 participants). Fourteen studies were from the UK, seven from the USA, one from New Zealand and one from Australia. While we had aimed to capture the experiences of parents of either sex, none of the studies included fathers. Five studies selectively recruited only bottle-feeding mothers,21 23 34 35 38 and most of the mothers in the remaining studies were bottle-feeding by the time they were assessed. The studies considered bottle-feeding with formula-milk and not expressed breast-milk. The qualitative studies used a variety of methods and criteria for recruitment (supplementary table 2): four recruited participants on the basis of particular feeding criteria (mothers who used mainly formula milk,21 whose babies had supplementary formula feeds on the postnatal ward,19 who intended to breastfeed antenatally17 or who initiated and then stopped breastfeeding22), while two recruited mothers using a variety of feeding methods (one recruited mothers irrespective of feeding method20 and the other specifically recruited mothers using different feeding methods18).

{kind=link}
Review flow chart.
Themes identified
We identified evidence related to five main themes: experiences of bottle-feeding, sources of information and support, feed preparation, quantity of feeds and formula milk changes. The qualitative studies mainly explored experiences of bottle-feeding, while the quantitative studies largely described sources of information and support, feed preparation and formula-milk changes.
Experiences of bottle-feeding
The six qualitative studies explored experiences of bottle-feeding in detail. Remarkably similar themes emerged in these studies, despite wide differences in their contexts—for example Lee described a “breastfeeding culture,”21 and Bailey talked of a “bottle-feeding culture.”17 When mothers chose to bottle-feed their babies, they experienced many negative emotions, especially if they had decided antenatally that they would breastfeed. This may have been because mothers had good knowledge about the benefits of breastfeeding.20
Guilt
Many of the mothers felt guilty about not doing what was best for the baby, and about taking account of their own needs. This was highlighted in all six qualitative studies.
I did feel really, really guilty that I didn’t try harder to breastfeed and I still do now. (Lee 1082)21
…I felt guilty as sin going out and buying artificial teats [to supplement with]. I felt awful. (Cloherty et al 201)19
…I’m giving more bottles now…and I feel a little disappointed about that… (Bailey et al 247)17
Everybody is telling you breastfeeding is best…what good mother wouldn’t want what’s best for her baby? (Mozingo et al)22
I just felt guilty because I thought I’m being selfish to quit. (Mozingo et al)22
I think the only thing is you feel that breastfeeding has been drummed into you. You almost feel guilty for saying that you want to bottle-feed. (Earle 327)20
Lee reported that 33% of mothers felt guilty, and 44% said they were made to feel guilty.21 Bailey et al described how some mothers tried to counter this guilt with a “give it a go attitude” and took comfort from the fact that others too had failed (to breastfeed) and gone on to bottle-feed.17
You can always try. At least I have tried (to breastfeed). (Bailey et al 244)17
I just wanted to give it a go. (Bailey et al 244)17
…elder sister tried it; … friend tried it… mum tried it...She couldn’t do it either. (Bailey et al 244)17
Anger or pressure
Five studies described the pressure to breastfeed felt by women.18 20–22 25 In the study by Lee, 50% said that women were put under pressure to breastfeed; some mothers found this pressure to be unreasonable and expressed anger about this.21 Mozingo et al also found that while women accepted that breastfeeding had many positive features, they felt considerable pressure to breastfeed.22 Cairney et al found that mothers felt hospital midwives were more likely than other professionals to expect mothers to breastfeed.25
…every single thing says breast is best...the pressure is massive, this is what you must do and if you don’t do it you’re harming your child. (Lee 1083)21
...their (the midwives”) emphasis is always on breastfeeding. If you don’t feel comfortable with breastfeeding you’re doing it just because of pressure so it’s not going to work for you. But their emphasis is on breastfeeding. (Earle 327)20
Sense of failure, shame and worry
In the study by Lee, 32% of mothers reported a sense of failure, 23% worried about what professionals might say, and 20% worried about the effect on their baby’s health.21 Similar feelings were reported in other qualitative studies.
You’re such a failure because all you’ve got to do for this baby is feed it and if you can’t do that, or you’re having problems with that, you must be rubbish. (Lee 1082)21
I just felt like I would be shamed because I wasn’t breastfeeding. (Mozingo et al)22
I think there is a bit of a stigma attached to it (bottle-feeding)…… with the breast-fed babies, the midwives were there, telling them how to do it, I suppose it is because you are left alone, you sort of think “oh I am one of the naughty ones,” so they let you get on with it. (Earle 328)20
…and you’re a horrible mother if you didn’t do it (breastfeeding). (Earle 327)20
It felt like I was going to harm him or something by giving it to him (bottle feeds). (The feelings lasted) for a good four or 5 months definitely. (Lee 1082)21
Uncertainty
Women said they did not get enough information from health professionals, which led to a feeling of uncertainty. Lee reported that 48% of mothers felt uncertain they were doing the right thing.21 In the study by Basire et al, women reported that the lack of clear, consistent information about the practical aspects of bottle-feeding was a problem, and some spoke of the mistakes they had made as a result. They emphatically requested information on all types of feeding, in order to make their own feeding decisions.18
It was bewildering really...you don’t know what you’re doing…we just felt completely in the dark. (Lee 1084)21
Relief
In contrast to the many negative emotions, many studies described a sense of relief when starting to bottle-feed. In the study by Lee, 76% of mothers reported feeling “pleased to find a solution that made things easier,” and 88% reported they were “relieved that the baby was being fed.”21 Mozingo et al reported that the sense of relief was mostly connected to concerns about the baby “getting enough.”22 Cloherty et al described how bottle-feeding gave “reassurance, peace of mind” and relieved anxiety.19
He had the bottle to set my mind at rest. (Cloherty et al 197).19
I mean it was relief to put her on the bottle. But the guilt it was unreal. (Bailey et al 247)17
Sources of information and support
Many mothers who bottle-fed their babies reported that they were not given adequate information from healthcare providers.18 25 Both breast- and bottle-feeding mothers considered that hospital midwives spent more time with breastfeeding mothers than bottle-feeding mothers.25 In the study by Lee, only 47% of mothers reported receiving information on use of formula milk.21 Similarly, in Cairney’s study, only 50% of bottle-feeding mothers reported receiving information antenatally on bottle-feeding (rising to 57% postnatally).24 Fein reported that only 21% of mothers had received such instruction by the time their babies were 2 months old. These results may reflect mothers’ beliefs that they already knew what to do.28 29 31–34 In addition, some healthcare providers noted that the WHO/Unicef code discourages active dissemination of information on bottle-feeding.18
Although healthcare providers were the most frequent source of information, women were more likely to initiate a discussion about infant feeding with family and friends,27 probably because women perceived healthcare providers as not being supportive of bottle-feeding.26
You don’t really get information from professionals about bottle-feeding, the do’s and don’ts, you just have to be self sufficient ... (Lee 1084)21
How feeds were prepared
UK recommendations for bottle-feeding include: (1) feeds should be made up with boiled water that has not been allowed to cool to less than 70°C (within 30 min of boiling); (2) the water should be added to the bottle before the milk powder to avoid overconcentration; and (3) equipment should be properly sterilised. Ideally, only one feed should be prepared at a time. However, it is considered acceptable to cool the bottle and store it in a refrigerator for up to 24 h.3
Hygiene and safety
Seven studies showed that recommendations for hygiene and safety for preparing formula feeds were often not followed.3 18 28 29 31 34 37 The UK infant feeding survey found that only 54% of mothers followed the first two recommendations described above.3 Remarkably, the USA Infant Feeding Practices survey (IFPS) found that 33% of mothers mixed formula with warm tap water.29 Furthermore, 20% to 48% of mothers heated preprepared bottles in a microwave,28 29 34 which is not recommended.
Reconstitution errors
Eleven studies reported reconstitution errors; mothers reported over concentrating feeds, under concentrating feeds or adding cereal to the bottle (see supplementary materials table 5).
Quantity of formula feeds
None of the studies explored how parents decided how much formula milk to give their babies or how often to feed them.
Formula milk changes
Although we did not prespecify this theme, we noted that seven studies reported that mothers made frequent changes to the type of formula feeds.23 28 30 33 34 37 38 Both Borghese et al and Polack et al reported that parents often changed the brand of formula milk because of regurgitation when it was possible that the reason for this symptom may not have been intolerance but overfeeding.23 38 The other common reasons for changing formula were colic, excessive crying and constipation.30 The decision to change formula was made by the mother or the health professional,38 and there was a risk that infants would wrongly be labelled as having an intrinsic abnormality (allergy or intolerance) with long-term consequences to their health.30
DISCUSSION
To our knowledge, this is the first systematic review of mothers’ experiences of bottle-feeding. We found that mothers who bottle-fed experienced a number of negative emotions such as guilt, anger, uncertainty and a sense of failure. Mothers were usually well informed of the benefits of breastfeeding but often found the pressure to breastfeed unreasonable.
A second major finding of our review was that mothers reported not receiving sufficient information about bottle-feeding. The WHO/Unicef code on infant feeding discourages active dissemination of information on bottle-feeding during the antenatal period, but permits postnatal advice and instruction on bottle-feeding only after the mother has decided to bottle-feed. However, several mothers expressed a desire to be able to make fully informed choices in advance. Furthermore, misinterpretation of the Unicef breastfeeding initiative could also lead to insufficient advice being given postnatally. A qualitative study in the UK by Furber highlighted that some midwives mistakenly thought that they were prohibited to provide active support for bottle-feeding mothers, even after the baby was born (“…we’re not supposed to be doing bottle-feeding demonstrations any more” and “…Bottle-feeding women are closeted away while we show them a demonstration [of preparing a bottle], because it’s a no, no…”).40
When women do not get information from healthcare professionals, they are reliant on friends and family, and incorrect practices are likely to be handed down from one generation to the next. Errors in formula milk preparation and handling occurred across all studies that measured this. Frequent formula milk changes may have led some mothers to believe that there was some intrinsic abnormality with the baby. In addition to the short-term issues of hygiene and safety, it is possible that errors in the measurement and over concentration of bottle feeds may contribute to overfeeding, rapid infancy weight gain and later obesity. It is well recognised that bottle-fed infants have an increased risk of subsequent obesity compared with those who were breastfed, and it has been proposed that bottle-feeding gives the parents more control and the infant less self-regulation, thereby potentially over-riding infant satiation cues.23 41
Strengths and weaknesses of the review
We conducted a comprehensive search, following the recommended stages for systematic reviews described by the Cochrane Collaboration.42 We used the same quality-appraisal criteria to assess both the qualitative and quantitative studies because the framework appeared to work well for both types of studies. The themes were congruent between studies irrespective of quality, and this supports our decision to include all the studies identified without weighting the studies based on quality criteria. Triangulation of data from qualitative and quantitative studies was not possible because they addressed different topics. The main limitations of our review are that the studies were mostly conducted in the UK or the USA. Indeed, to aid consistency of context, we excluded studies carried out in developing countries, and our findings may not be applicable to such settings. Compared with the vast literature on breastfeeding,43 44 we identified only six qualitative studies that explored mothers’ experiences. We found no studies that explored fathers’ experiences or attitudes, and we also found no studies that examined how mothers made decisions about the frequency or quantity of bottle-feeds.
Implications for policy and practice
Since the vast majority of babies receive at least some formula milk during the first year of life, it is important that this is prepared and administered safely and correctly. While it is important to increase the initiation and duration of breastfeeding, it is also necessary to minimise the risks associated with bottle-feeding by providing adequate information and support in a sensitive and non-judgemental manner to parents who choose to bottle-feed their infants. As suggested by Mozingo, “when the decision is made to start formula-feeds, mothers should be reassured that bonding, attachment and infant health are not irreversibly damaged, and the quality of their mothering should not be questioned because of the feeding method chosen.”22
The Unicef Baby Friendly Initiative (BFI) and recent guidance from the National Institute for Health and Clinical Excellence (NICE) on postnatal care, while promoting breastfeeding, also recognise that parents who are giving their babies formula feeds should be offered appropriate and tailored advice to ensure this is undertaken safely.45 46 Our review suggests that such information and support on bottle-feeding does not happen in many settings. Indeed, some mothers may not receive this instruction because of the mistaken belief by health professionals that the BFI prohibits this. With increasing governmental support to expand the number of BFI-accredited units,47 healthcare providers should ensure that the needs of parents who bottle-feed are not overlooked.
What is known on this topic
Almost all babies receive some formula-feeds during the first year of life.
Errors in the preparation of formula-feeds are common. Such errors and other variations in formula-feeding may have both short- and long-term health consequences.
What this study adds
Many mothers who introduce formula-feeds experience negative emotions such as guilt, anger, uncertainty and a sense of failure.
These mothers do not receive sufficient information and support from healthcare providers. While it is important to promote breastfeeding, it is also necessary to ensure that the needs of bottle-feeding mothers are not overlooked.
Acknowledgments
We would like to thank I Kuhn, Reader Services Librarian at the University of Cambridge Medical Library, for her help in developing the search strategy and the first authors whom we contacted for their assistance.
RL led the review and is guarantor. RL carried out the literature search with supervision from DO and help from Isla Kuhn. All authors appraised and extracted data from the primary studies and analysed the findings. RL drafted the manuscript. All authors contributed to the critical revision of the manuscript and approved the final version.
REFERENCES
Supplementary materials
Web only appendix 98;8:596
Files in this Data Supplement:
Web only appendix 94;8:596
Files in this Data Supplement:
Footnotes
Competing interests: None.
Funding: This work was supported by the Medical Research Council. RL is funded by a MRC health services and health of the public fellowship.
▸ Additional supplementary tables are published online only at http://adc.bmj.com/content/vol94/issue8