Article Text

Abstract
Ensuring a safe and effective transition of young people with chronic illness and disability from paediatric care to adult health services is a key quality issue for the NHS. To achieve this, three elements must be pursued with vigour. Firstly, a cultural shift in NHS staff attitudes and training is required. Secondly, systems must change to ensure that all paediatric chronic illness and disability services have effective transition programmes in place. Thirdly, young patients need to be trained and empowered to allow them to be an effective partner in their own transition. Improvement of this transition is merely one part of a wider need to improve health care for adolescents.
Statistics from Altmetric.com
Reports and standards on adolescent health in the UK
Platt report. The welfare of children in hospital. Platt H, Ministry of Health. Central Health Services Council, London: HMSO, 1959
Court report. Fit for the future: The report of the Committee on Child Health Services. Volume 1, Court D, London: HMSO, 1976
Bridging the gaps: Healthcare for adolescents. Report of the Intercollegiate Working Party on Adolescent Health, 2003 5
Adolescent health. BMA Board of Science, 2003
National Service Framework for Children, Young People and Maternity Services, 2004 3
Youth matters: Youth Green Paper. HM Government, July 2005
You’re welcome quality criteria: making health services young people friendly. Department of Health, London, 2005
Transition: Getting it right for young people, Department of Health, 2006 1
The need to provide better services for adolescents within UK paediatric departments is now widely acknowledged, and has been driven by a series of governmental reports and standards over the past 5 years (see the box below). It also reflects a growing recognition of the importance of adolescent care to paediatric practice in the UK.1–5
One particular aspect of adolescent care, namely the transition from paediatric services to adult health services, is particularly topical. This topicality stems in part from a recent (and ongoing) Department of Health initiative on transition (the Transition Champions Project), aimed at ensuring that young people do not miss out on healthcare during the transfer between paediatric and adult services.
The now standard definition of transition is that of the Society for Adolescent Medicine in the US, which notes that transition can be defined as “a purposeful, planned process that addresses the medical, psychosocial and educational/vocational needs of adolescents and young adults with chronic physical and medical conditions as they move from child-centred to adult-oriented healthcare systems.”6 It is important to recognise that this transition is merely one part of the wider set of educational, personal, family and social transitions young people make during adolescence.
Transition is now a key quality issue for paediatric services1 for two main reasons. Firstly, increased survival of children with complex or congenital conditions has produced cohorts of adolescents and young adults with diseases previously unseen by adult services. For example, the prevalence of cystic fibrosis (CF) in people over 15 years of age in the UK more than doubled between 1977 and 1985,7 and by the mid 1990s, the mortality rate for childhood CF was so low that the main determinant of the adolescent and young adult CF population was the number of children born.8 Currently the vast majority of children with childhood congenital or chronic illness survive to adult life. Furthermore, the burden of other common chronic illnesses in adolescence is increasing. Significant increases have been recorded during the 1990s of the prevalence of the commonest chronic conditions, such as asthma9 and diabetes.10
Secondly, and perhaps most importantly, poorly planned transition can be associated with increased risk of non adherence to treatment and of lack of follow-up, with subsequent measurable adverse consequences in terms of morbidity and mortality as well as in social and educational outcomes.11 The particular dangers of moving from paediatric to adult services is well illustrated by reports of disasters resulting from the treatment of adult congenital heart patients by cardiologists with little knowledge of congenital heart disease.12 In solid organ transplants, non-adherence and problems with transition have been identified as one of the major causes of graft loss.13 14
There has been a raft of recent publications on how to improve transition and provide quality services for adolescents during transition. They all essentially emphasise the same issues and have been comprehensively reviewed in the Department of Health’s recent guidance: Transition: getting it right for young people. Improving the transition of young people with long term conditions from children’s to adult health services,11, which is freely available on the Internet.
The basics of transition are simple and are common to all diseases and conditions. Firstly, prepare young people and their families well in advance for moving from paediatric to adult services and ensure they have the necessary skillset to survive and thrive there. Secondly, prepare and nurture adult services to receive them. Thirdly, listen to young people’s views.
Clearly there is variation by disease and geographical location, but key generic elements of a successful transition programme are outlined in the box above.1
Transition issues may be particularly pertinent and problematic for vulnerable young people, such as those in care, looked after and in other special circumstances (see the box above right).11
Young people’s views on what they want from transition are outlined in the box on the right.
Much of the transition literature has focused on change at a system level, improving the health services that the adolescent moves between according to the principles outlined in the list above. This has largely informed the current Department of Health’s Transition Champions Programme, although this has also taken the innovative approach of identifying key local and national “champions” to spearhead change in practice.
There is a need to acknowledge that change in systems to give young people good transitions in health care, however desirable, might be difficult to achieve amid the competing demands of our constantly reformed health services. In the USA, for example, where transition issues have been on the agenda for over 20 years, little progress seems to have been made. Although it is likely that health services such as the NHS in the UK may be more successful in improving transition, we must also move towards empowering young people to help drive their own transition by beoming self-aware fully engaged young expert patients. Moving beyond mere “support” and instead enhancing young people’s self-management skills must become an essential element of good transition practice. As noted recently by Sawyer et al., “The notion of transition to adult healthcare is implicitly based on the need to help actualise young people’s emerging capacity for self-management.”16
It is customary when writing about transition to deplore the paucity of published evaluations of transition programmes that go beyond surveys of satisfaction. Although we strongly support the need for focused evaluation of different models of service provision, and we welcome the emerging evidence base,15 17 we should not wait for rigorous evaluation evidence before instituting programmes that ensure that adolescents are adequately trained in disease self-management and that a plan is in place to ensure their disease control or quality of life does not suffer in the move from paediatric to adult services.
Even more important is the recognition that transition is only one part of the more important agenda of improving the lot of adolescents in the NHS. There is a growing recognition within UK paediatric services that a greater emphasis is needed on training paediatricians to deal with adolescents within paediatrics services, not merely to organise their transfer to adult services. This was strongly enunciated in the National Service Framework (NSF) for Children, Young People and Maternity Services3 and in the Royal College of Paediatrics and Child Health (RCPCH)-led Intercollegiate Adolescent Working Party Report: Bridging the gaps.5
Traditionally, young people aged over 12 years have been the poor relations to babies and younger children in our health services. Training of paediatricians has focused overwhelmingly on the under threes, with few paediatricians having received or sought training in the specific issues of adolescents. Similarly, UK paediatric services have focused on acute care for neonates and young children, as well as a more recent focus on community paediatric services for children with a disability. Many acute paediatric services continue to not admit acute adolescents over the age of 14 years, despite clear guidance from the NSF that paediatric services should retain responsibility for young people until they reach 16, if not till 18 years.3
There are undoubtedly beacons of excellence where individual clinicians and teams have developed services that recognise the specific needs of young people, particularly for certain chronic conditions and in isolated services for marginalised or vulnerable young people. That these are the rare exceptions rather than the rule is an indictment of UK paediatric services, according to the quality standards of the NSF.
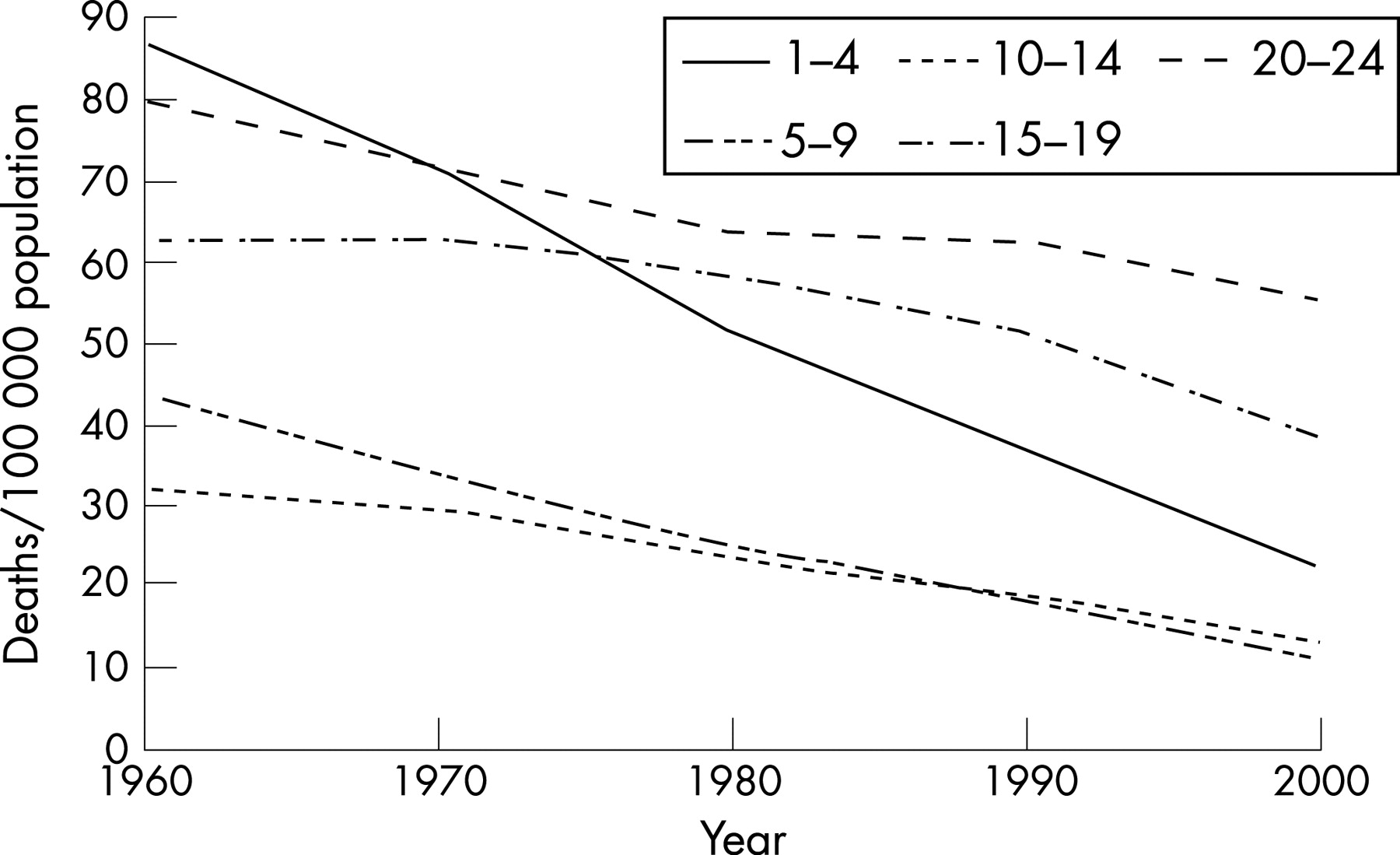
The reasons for the neglect of adolescents in UK paediatrics are largely historical. Paediatric services in the UK were largely a product of the foundation of the NHS and were built in response to concerns about infant and young-child mortality in the earlier part of the twentieth century. Sixty years later patterns of morbidity and mortality are very different; the marked improvements seen in mortality rates of young children have not been matched by those of adolescents, and mortality in older adolescents now outweighs that of the under fives (see Figure 1). The new speciality of community paediatrics is for the most part devoted to chronic conditions and disability, and acute paediatricians spend an increasing proportion of their time managing chronic conditions such as asthma, diabetes and epilepsy. The proportion of time that paediatricians spend working with young people is unknown; however, UK hospital statistics suggest that adolescents now make up about 25% of the outpatient workload of hospital paediatric services (www.hesonline.gov.uk). Yet the training and focus of UK paediatricians, despite a recognition of the importance of chronic-illness management and multidisciplinary working, has up till now fundamentally retained the 1950s mindset that the business of paediatrics is prepubertal children.
{kind=link}
Fortunately there are signs that this is beginning to change. The RCPCH’s curriculum contains a number of competencies specifically relating to adolescents. By the end of Level 1 Training, trainees will:
Begin to understand the processes of adolescence including experimental behaviours, learning by experience, achieving independence from the family, and the consequences of these on health and illness in young people.
Understand and begin to develop skills to respond appropriately to episodes of self-harm in adolescents.
Understand the different specific and changing health needs of adolescents as inpatients and outpatients.
Understand normal and abnormal pubertal development and its relationship to growth.
be aware of national policies for reduction of teenage pregnancy.
Understand contraceptive and sexual health issues and know where appropriate advice might be sought.
Be aware of issues relating to gender and sexual identity.
Know about issues around transition from paediatric to adult care in adolescents with chronic conditions.
Although these are a tiny proportion of the competences in the entire paediatric curriculum approved by Postgraduate Medical Education and Training Board this year. More encouragingly, the RCPCH is developing an exciting e-learning training package in adolescent health for trainees that covers all the College’s adolescent competences, as part of a wider multi-professional educational programme in adolescent health funded by the Department of Health.
Conclusions
Transition is now well established as a major issue on the quality of care agenda for both paediatricians and for adult healthcare providers. The basics are simple and are applicable to any condition, service configuration or geographical location. Although some additional resources will be necessary, changes in attitude and behaviour are important cost-neutral strategies, which must not be overlooked. However it is important that transition is seen as only one part of a wider improvement of healthcare for young people.
REFERENCES
Footnotes
Funding: This work was undertaken at University College London Hospital/University College London, which received a proportion of funding from the Department of Health’s NIHR Biomedical Research Centres funding scheme.
Competing interests: None.