Article Text

Abstract
Objectives: To gather data on the ages and weights of paediatric patients between 1 and 10 years of age, and to compare these data with the current weight estimation formula weight(kg) = 2(age+4). If a significant difference was found, the data would be used to derive a more accurate formula.
Design: Retrospective study using data collected from paediatric attendances at an emergency department (ED).
Setting: A large ED in a major UK city, treating both children and adults.
Patients: 17 244 children aged 1–10 years, attending the ED between June and December 2005.
Main outcome measures: Weight difference between the measured weight and the expected weight, the latter given by weight = 2(age+4).
Results: The weights of seriously ill children were recorded in only 41.5% of cases, necessitating a weight estimate in the remainder. The formula weight = 2(age+4) underestimated children’s weights by a mean of 18.8% (95% confidence interval (95% CI) 18.42% to 19.18%). Using linear regression and analysis of each individual age group, ten new formulas were tested. Of these formulas, weight(kg) = 3(age)+7 proved the most accurate with a mean underestimate of just 2.48% (95% CI 2.17% to 2.79%).
Conclusions: Weight estimation remains of paramount importance in paediatric resuscitation. This study shows that the current estimation formula provides a significant underestimate of children’s weights. When used to calculate drug and fluid dosages, this may lead to the under-resuscitation of a critically ill child. The formula weight(kg) = 3(age)+7 provided a safe and more accurate estimate of the weight of today’s child.
- APLS, advanced paediatric life support
- 95% CI, 95% confidence interval
- ED, emergency department
- EPLS, European paediatric life support
- MAC, mid-arm circumference
- PICU, paediatric intensive care unit
- child
- weight
- estimation
- formula
- resuscitation
Statistics from Altmetric.com
- APLS, advanced paediatric life support
- 95% CI, 95% confidence interval
- ED, emergency department
- EPLS, European paediatric life support
- MAC, mid-arm circumference
- PICU, paediatric intensive care unit
In the management of the acutely unwell child most interventions, such as drug doses, fluid boluses and DC shocks for defibrillation, are based on the weight of the child in kilograms. For various reasons it is not always possible to weigh the child accurately, for example if the child cannot be moved due to trauma, active resuscitation or severe pain. In these instances an estimation of the child’s weight must be made, and there are various published methods for calculating this. The most commonly accepted method for weight estimation of children aged 1–10 years in Europe, South Africa, Australia and New Zealand is the age based formula recommended by the advanced paediatric life support (APLS) course.1 This formula uses the child’s age at its last birthday, that is age in completed years, and is given by weight (in kg) = 2×(age in years +4).
The purpose of this study is to compare this current formula with a large sample of present day children’s weights to assess its reliability and to examine whether a different formula would be more accurate, thereby improving the resuscitation of the unwell child. A pilot study of children in England and New Zealand has indicated that the current formula may be inaccurate.2 The questions asked are:
-
Given an increase in children’s weights, is the current weight estimation formula still accurate in a Western paediatric population?
-
Should the current formula prove inaccurate, is there another formula that is more accurate?
METHODS
Ethical permission was obtained from the North Sheffield Research Ethics Committee. With the assistance of a medical statistician, a sample size calculation was carried out to establish the minimum number of children needed to provide sufficient data to enable individual age group analysis. Thus, using a 5% level of statistical significance with power of 80%, this was determined to be 400.
The data were collected on 17 244 children from 1–10 years of age (inclusive) so as to match the age range covered by current formula.
Details of weight, age at presentation, sex, ethnicity and emergency department (ED) streaming category (table 1) were collected retrospectively from June 2005 to December 2005 from the database at the Emergency Department, Queen’s Medical Centre Hospital, Nottingham. These data are recorded by the receptionist, triage nurse or doctor by weighing the children on a Proweight Excel (weighbridge), a Seca 1 (standing scale) or a Weymed 550BT (infant scale), each of which is regularly calibrated. Weights were recorded with children wearing a minimum of clothing and without shoes. Data outlier removal occurred for points lying outside 4 standard deviations and subjectively if it was clear that data had been entered incorrectly. A scatter plot was used to assist with this. A t test was employed to look for difference between male/female ages and weights.
Paediatric attendances at an emergency department
The difference between measured weight and that derived using the current formula was calculated and expressed as a percentage of the estimated weight rather than a kilogram value. This was because a weight difference in kilograms would differ markedly from young to older age groups as weight increases with age. The percentage weight difference gave comparability across all age groups.
The standard deviation of the percentage weight difference was calculated. A linear regression analysis was performed for weight (y axis) and age (x axis) to obtain a line of best fit. Using the gradient and y axis intercept as starting points, a variety of new formulas were devised according to the following three rules. The formula must:
-
be easily calculable in order to allow mental arithmetic,
-
be more accurate than the current formula,
-
not significantly overestimate weight, to avoid drug over-dosage.
The original data, with outliers removed, were then reprocessed for each new formula to calculate the mean weight difference between measured and calculated weights for all ages overall and for individual age groups (eg, 1 year olds, 2 year olds, etc).
RESULTS
The percentage of weights recorded by ED streaming category is shown in table 1. The target is 100% weight recording. Ethnicity was poorly recorded and not used in the final results. The number of data outliers removed totalled 104. There was no statistical difference between males and females in terms of weight or age in the data used (p<0.05 for both weight and age).
The recorded weights when compared to the current formula of weight = 2(age+4) showed that children’s weights were underestimated by a mean of 18.8% (95% confidence interval (95% CI) 18.42 to 19.21) by the formula.
Linear regression analysis yielded weight = 2.57(age)+7.24. From this and using the rules set out in Methods, ten new formulas were tried. All the formulas were, as a mean, more accurate than the current formula when considered over all ages. However, the individual age group analysis revealed that weight = 3(age)+7 was the most accurate formula. This equation yielded a mean underestimate of weight of 2.48% (95% CI 2.17 to 2.79). It was the same as the current formula for 1 year olds and more accurate at all other ages, although it overestimated some weights in the middle age groups (maximum 5.17% at 5 years). Unlike the other formulas, it successfully estimated weights at the higher age groups.
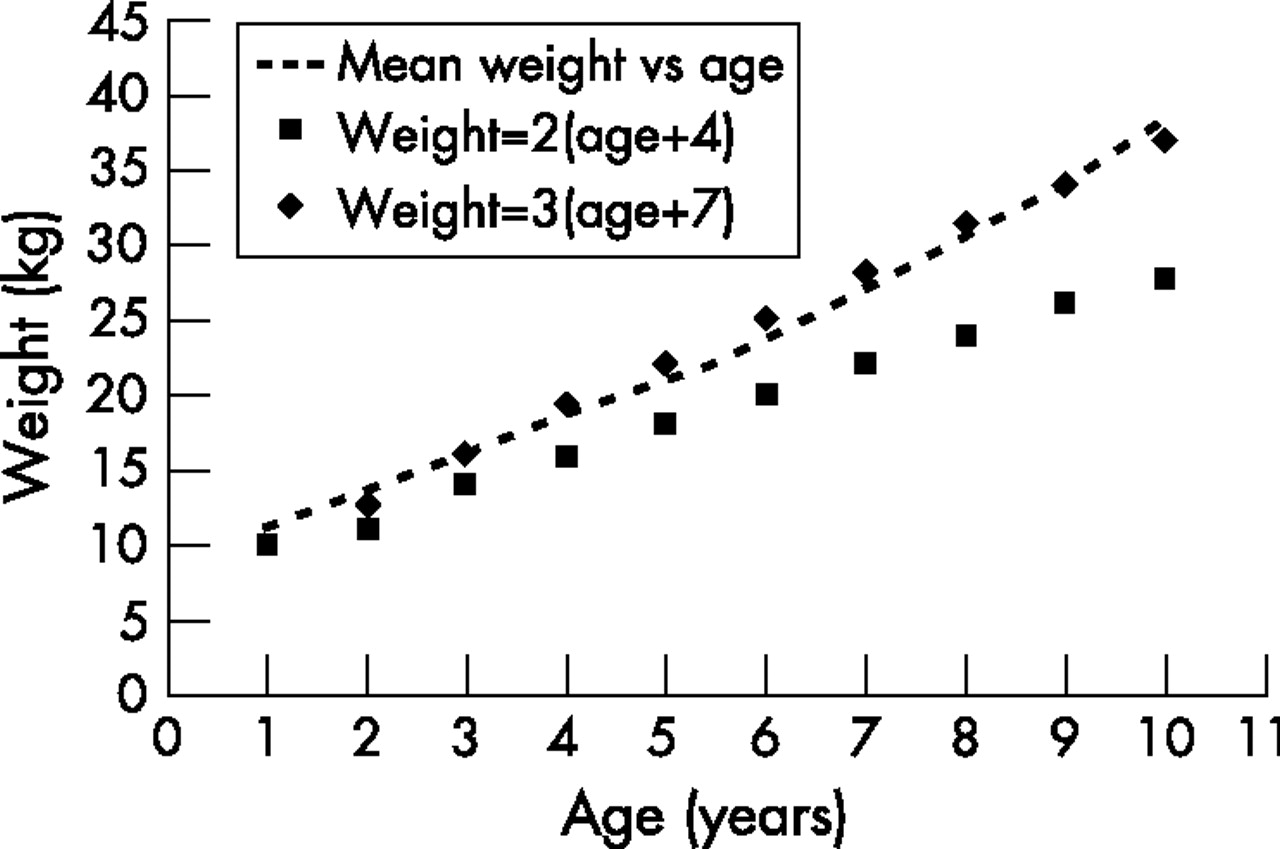
Individual age group breakdowns using this and the current formula are compared in table 2. The graphical representation of these results is shown in fig 1.
Individual age group breakdown
{kind=link}
Weight versus age. The curve of the mean recorded weights versus ages is shown as the broken line. At approximately 6 years old there is a change to steeper gradient.
DISCUSSION
The weight of children is increasing3 and childhood obesity is a topical debate in both medical and international media. There has been an unprecedented rise in obesity in the United Kingdom and in the European Union.4
An increase in children’s weights may mean the currently used formula underestimates weight, thus leading to failure in achieving optimal resuscitation with the consequence of increased mortality and morbidity, a theory supported by Argall et al.5 Therefore, the origins of any weight estimation formulas should be carefully checked. The APLS manual and an online literature search failed to identify any research or data to support the origins or accuracy of the current formula.
In Fanconi and Wallgren’s Textbook of paediatrics from 1952, mean weights of children are listed, but no weight estimation formula is given.6 When the current formula is applied to these weights it gives a good estimate, with a mean underestimate of just 5.2% for all ages. However, these data are more than 50 years old and use the weights of post-war children. A weight estimation formula applicable to these children is unlikely to be accurate in the present day child, implying the need for a new formula.
Historically, parents or clinicians caring for the child have visually estimated or “guesstimated” weights, a technique which has been shown to be inaccurate.7,8,9,10 Various tools were introduced to help clinicians, such as the Broselow tape,11 which estimates drug doses from the length of the child, and also growth tables, but their use is limited by their availability. Some other suggested formulas dependant on shoe size and mid-arm circumference (MAC) are discussed by Carroll et al,12 who indicate that these formulas (6.8×(shoe size×0.102) and (MAC (in cm)×3.6)−40, respectively) are not straightforward. Although limited by sample size, these methods may be more accurate than the current formula but their complicated nature makes them difficult to apply clinically. Carroll also suggests the use of a computer or portable device to calculate weights, but these are not always available depending on the location of resuscitation. Paediatric resuscitation is a stressful environment, and complicated formulas only increase the potential for error.
In paediatric resuscitation, drug doses, fluids, ventilator settings and DC shocks are based on the weight of the child. Weighing the child is the gold standard, but a weighbridge or scales may not available or appropriate due to the child’s condition. The results of this study illustrate this, as only 41.5% of triage category 1 patients (ie, those in need of immediate resuscitation) were weighed despite the availability of a weighbridge, compared to 94% of triage category 7 patients (minor injuries to be seen by a nurse practitioner). Therefore, accurate, quick estimation of the sick child’s weight is sometimes required.
This study shows the current formula gives a significant (18.8%) underestimate of the weight of children aged 1–10 years. If this weight is then used to guide therapy, there will be a corresponding significant under-administration (again 18.8%) of fluid boluses, resuscitation drugs, etc. This may lead to additional procedures, such as tracheal intubation and blood transfusion, occurring unnecessarily with additional risk and cost.
Any simple formula will give only an estimate of a child’s weight, and the child’s true weight will only rarely be calculated, but a formula closer to the mean weight will allow more accurate weight estimation. Paediatric drug dosages are calculated from body weight and are also an estimate, based on physiological data and therapeutic ranges. To maximise the effectiveness of these drugs, a weight estimation formula should be as accurate as possible. In deriving this formula a linear regression analysis was used to find the line of best fit and yielded weight = 2.57×age+7.24. This is, once again, too complicated for mental arithmetic and the risk of calculation error is high, especially in difficult clinical situations.
An overall increase in accuracy was provided by the formula weight = 2(age+5), also suggested by the pilot study,2 although the individual breakdown of age groups (not performed in the pilot study) showed it became increasingly inaccurate at higher age groups. The formula weight = 3(age+2), suggested by Argall et al, provided a better estimate from the age of 6 and older than either the current formula or the weight = 2(age+5) formula and could effectively be used for these age groups. However, under the age of 2 it falls below the current formula and the proportionally greater blood volumes in this age group would exaggerate potential under-resuscitation.13 However, to replace one formula with two may be a source of confusion, particularly as resuscitation guidelines have evolved to standardise paediatric treatments for wide ranging age groups (1 year old to puberty).14
The formula weight = 3(age)+7 was the most accurate of all those tried, with a mean underestimate of 2.48%. It was the same as the current formula at age 1, but more accurate at all other ages. It is more accurate than all the other formulas from age 6 and older. There is an overestimate of weight at the middle age ranges with a maximum overestimation of 5.17%, but given the high volume of distribution (VD>1 l/kg) of resuscitation drugs this will not translate into a significant increase in plasma drug concentration. When considered against the current formula, which provides a 15.9% under-dose at this age and a 36.6% under-dose at age 10, then the current formula is potentially more harmful.
Whether actual harm can be attributed to use of the current formula, or any benefit gained by using an improved estimate, remains unknown and is beyond the scope of this study. If a significant underestimate of weight did lead to unnecessary intubation, blood transfusion or inotropic support (perhaps needing central venous access), then there is clearly the potential for harm as a result of these procedures. The APLS manual recommends considering inotropes and intubation with the third fluid bolus of 20 ml/kg. In addition, a child admitted from the ED to the paediatric intensive care unit (PICU) with a significant weight underestimate may have this weight used throughout their stay on PICU if they are not well enough to be weighed. This has the potential for prolonged underdosing of antibiotics and other drugs and an underestimation of the required urine output, which may be detrimental to the outcome of the child. An improved estimate might prevent this.
However, to continue to use a demonstrably poor weight estimate cannot be considered good medical practice. A transition from one formula to another may cause confusion in the short term, but if a change is needed then it should be implemented and would be relatively simple when compared with the major changes to the 2005 resuscitation guidelines which have been successfully introduced. The formula can be used for both sexes as a t test showed no statistically significant difference at any age between males and females.
CONCLUSIONS
This study has shown that the current formula gives a significant underestimate of paediatric weights for those between 1 and 10 years of age and that this is likely to lead to the under-resuscitation of an acutely unwell child. The study also showed that weight was often not recorded in the most seriously ill children and consequently there is a need for a simple, more accurate formula to minimise error in these situations.
What is already known on this topic
-
The current method of calculating weight from age (in whole years) is given by weight(kg) = 2(age+4) This formula is used by the Advanced Paediatric Life Support Group (APLG), and the European paediatric life support (EPLS) course.
-
The weight of children is known to be increasing.
What this study adds
-
Weight estimation is needed as critically ill children are shown to be weighed far less often than those with minor complaints.
-
The formula weight (kg) = 2(age+4) significantly underestimates weight, possibly causing inadequate resuscitation of the acutely unwell child.
-
The updated formula weight(kg) = 3(age)+7 is simple to calculate and provides a more accurate estimate of the weight of the modern day child.
The use of two formulas may be more accurate overall given the change in gradient of the age–weight curve at approximately 6 years of age. However, in the stressful environment surrounding paediatric emergencies, using two formulas may increase the potential for error. Therefore, the formula which best represents the age range 1–10 years should be used to directly replace the current formula.
The authors recommend the formula weight (kg) = 3(age)+7. The age is in completed years (or age last birthday). It is easily calculable, safe and more accurate than the current formula. It is a revised estimate for the weight of the modern day child.
Limitations of the study
Ethnic origin was recorded in only 40% of cases. Consequently, it is not known if these data apply to all ethnic groups in the UK. This data sample, while large, is only from one city in the UK, although the pilot study showed a similar mean underestimate when using the current formula. The weight of children in the Western world is increasing, but this may not apply to the developing world where there is an increased incidence of disease and poor nutrition. The study did not compare the formulas with other methods of weight estimation and more work may be needed in this area. The graph (fig 1) suggests the new formula may fit well with higher age groups. However, data would need to be gathered for 11–16 year olds to confirm or refute this.
Acknowledgments
We would like to thank the following for their invaluable assistance: Mr Raza Dar (consultant, emergency medicine) gave advice; Mark Fairweather (pharmacist) gave advice on paediatric pharmacology; Jean Johnson (library and information skills training coordinator) helped with literature searching; and Nicola Luscombe (emergency nurse practitioner). Proof reading and advice: Dr Richard Marks (consultant anaesthetist) assisted with the pilot project and gave advice; Phillip Miller (research nurse) helped with data collection; Suzanne Owens (emergency nurse practitioner), proof read and gave advice; and Tracey Young (Trent RDSU) provided statistical advice
CONTRIBUTORS
ML conceived the study and prepared the study design. BO collected the data. ML and BO carried out the study and prepared the manuscript. ML is the guarantor.
Supplementary materials
M Luscombe and B Owens. Weight estimation in resuscitation: is the current formula still valid? Arch Dis Child 2007;92:412�15. The formula published in fig 1 of this paper is incorrect. The correct formula is as written throughout the remainder of the manuscript�that is, "Weight=3(age)+7".
Footnotes
-
Published Online First 9 January 2007
-
Funding: No funds were applied for or received for this study.
-
Competing interests: None.
Linked Articles
- Précis
- Atoms
- CORRECTION