Article Text

Abstract
Aims: To determine whether the risk of hyponatraemia in children with gastroenteritis receiving intravenous (IV) fluids is decreased by the use of 0.9% saline.
Methods: A prospective randomised study was carried out in a tertiary paediatric hospital. A total of 102 children with gastroenteritis were randomised to receive either 0.9% saline + 2.5% dextrose (NS) or 0.45% saline + 2.5% dextrose (N/2) at a rate determined by their treating physician according to hospital guidelines and clinical judgement. Plasma electrolytes, osmolality, and plasma glucose were measured before (T0) and 4 hours after (T4) starting IV fluids, and subsequently if clinically indicated. Electrolytes and osmolality were measured in urine samples. Results were analysed according to whether children were hyponatraemic (plasma sodium <135 mmol/l) or normonatraemic at T0.
Results: At T0, mean (SD) plasma sodium was 135 (3.3) mmol/l (range 124–142), with 37/102 (36%) hyponatraemic. At T4, mean plasma sodium in children receiving N/2 remained unchanged in those initially hyponatraemic (n = 16), but fell 2.3 (2.2) mmol/l in the normonatraemic group. In contrast, among children receiving NS, mean plasma sodium was 2.4 (2.0) mmol/l higher in those hyponatraemic at baseline (n = 21) and unchanged in the initially normonatraemic children. In 16 children who were still receiving IV fluids at 24 hours, 3/8 receiving N/2 were hyponatraemic compared with 0/8 receiving NS. No child became hypernatraemic.
Conclusions: In gastroenteritis treated with intravenous fluids, normal saline is preferable to hypotonic saline because it protects against hyponatraemia without causing hypernatraemia.
- ADH, antidiuretic hormone
- IV, intravenous
- RRP, rapid replacement protocol
- SRP, slow replacement protocol
- sodium
- gastroenteritis
- fluid therapy
- infusions intravenous
- dehydration
Statistics from Altmetric.com
- ADH, antidiuretic hormone
- IV, intravenous
- RRP, rapid replacement protocol
- SRP, slow replacement protocol
Recent publications1–3 have highlighted the potential for life threatening hyponatraemia associated with the use of intravenous hypotonic saline in hospitalised children, including children with gastroenteritis.2,4 Although most guidelines recommend low osmolarity oral rehydration solutions for rehydration of children with mild to moderate dehydration secondary to non-cholera gastroenteritis,5–7 intravenous fluids are frequently used when oral rehydration is not tolerated, particularly in developed countries.8,9,10 There is no consensus however on the most appropriate electrolyte composition of intravenous (IV) fluids, with recommendations ranging from 0.45% to 0.9% saline solutions.5–7,11 Previously, we have documented antidiuretic hormone (ADH) activity inappropriate for the plasma sodium and osmolality in children receiving intravenous fluids for mild to moderate dehydration associated with gastroenteritis.12 While this could cause dilutional hyponatraemia irrespective of the saline content of the fluid, the use of a fluid with a higher tonicity presenting less electrolyte free water should reduce this risk.1,13
To explore this, we studied the changes in blood and urine biochemistry in children with a presumptive diagnosis of gastroenteritis in whom a decision to treat with IV fluids had been made by their treating physician. Apart from randomisation to either normal or half normal saline, other aspects of management, including fluid rate, were determined by the treating physician based on hospital guidelines and clinical judgement. As we found previously that the biochemical response to IV fluids differed according to the plasma sodium at presentation,12 we analysed the results according to whether children were hyponatraemic or normonatraemic at presentation.
METHODS
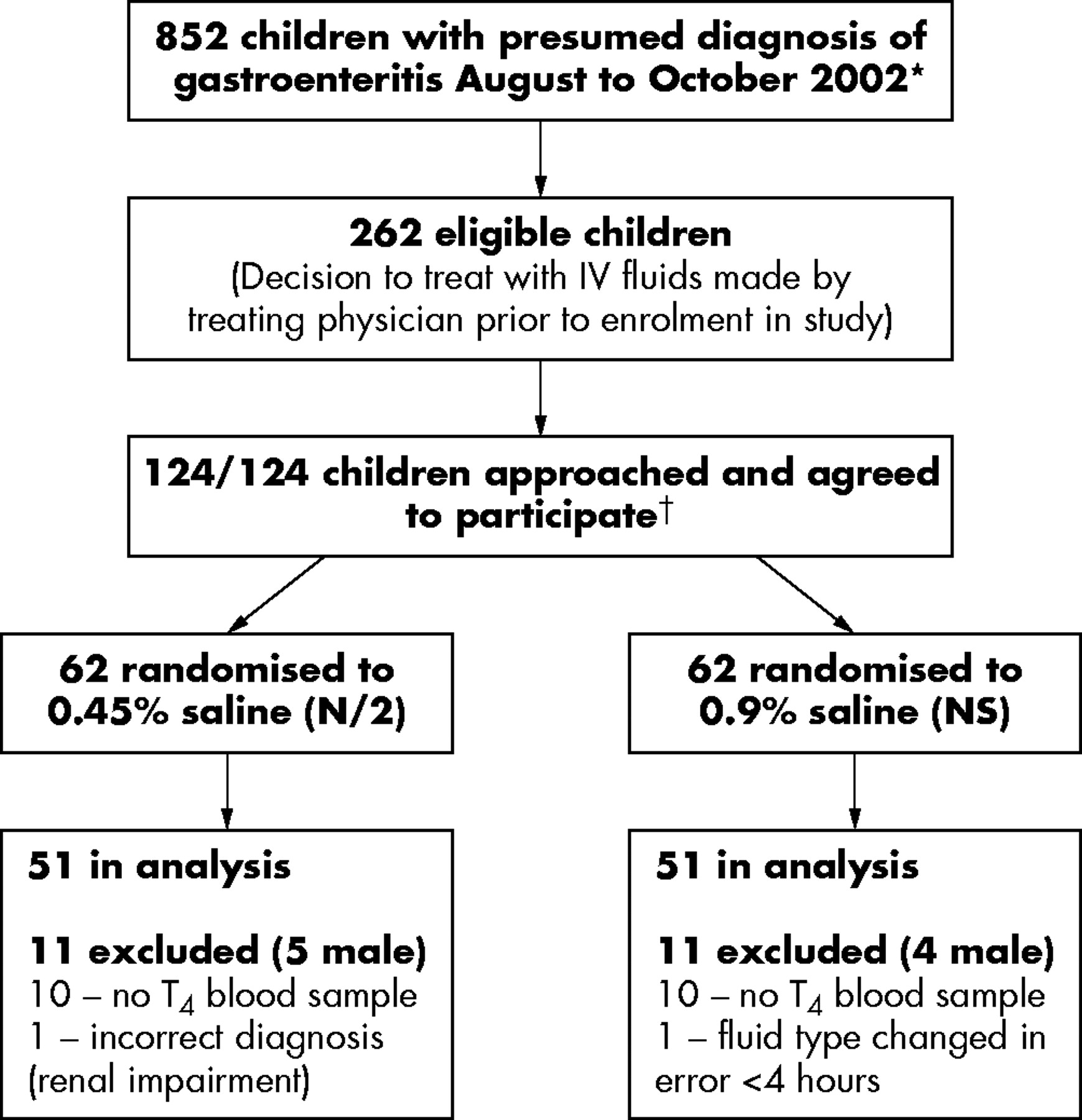
The study was conducted at Sydney Children’s Hospital between the months of August and October 2002, corresponding to the annual peak incidence of rotavirus infection.14 Children aged between 6 months and 14 years with a presumptive diagnosis of gastroenteritis were eligible for enrolment in the study only after a decision to treat with intravenous (IV) fluids had been made by their treating physician, independent of the study (fig 1). The reasons recorded for this decision were the combination of dehydration and either continued vomiting or inadequate intake of oral fluids in the emergency department. Children were excluded from the study if they had a known abnormality of ADH secretion, nephrogenic diabetes insipidus, pituitary or hypothalamic disease, renal disease, acute or chronic lung disease, or were receiving drugs known to stimulate ADH secretion. The study protocol was approved by the South Eastern Area Research Ethics Committee and informed consent was obtained from a parent/guardian of all children.

Flow diagram of patient selection. *Corresponding to the annual peak incidence of rotavirus infection. †A registered nurse was employed 40 hours per week (including weekends and after hours) to facilitate the correct administration of the study protocol in a busy emergency department. Enrolment was carried out only during her shifts.
At enrolment, children were prospectively randomised to receive either 0.45% saline + 2.5% dextrose (N/2) or 0.9% saline + 2.5% dextrose (NS) by sequential selection of an opaque sealed envelope containing the fluid choice. The treating physician was told which fluid had been selected. The rate of infusion was not randomised, but was determined by the treating physician according to one of two clinical protocols in use in the emergency department: the “rapid replacement protocol” (RRP; 10 ml/kg/h for 4 hours), or the “slow replacement protocol” (SRP; maintenance fluids15 + estimated dehydration as a percentage of body weight replaced over 24 hours). Blood samples were collected before (T0) and 4 hours after (T4) the start of IV fluids, with the T4 measurement corresponding to completion of the RRP. The study protocol permitted the treating physician to change the fluid type after the first 4 hours of infusion. However this was done in two patients only: one child was changed from NS to N/2 at 5 hours because the plasma sodium concentration had increased from 130 to 135 mmol/l; and one was changed from N/2 to NS at 10 hours because the plasma sodium concentration remained below 135 mmol/l.
Details of the illness prior to presentation were recorded. The admission weight, length (in children under 2 years), or height and body mass index (BMI; weight/height2) were expressed as standard deviation scores (SDS)16,17 to allow comparison across ages. The degree of dehydration at presentation was estimated using standard clinical measures.18 Stools for culture and rotavirus antigen testing were obtained in 35/102 children, 30 of which were positive for rotavirus antigen. There were no differences in the historical, clinical, or biochemical characteristics at presentation or the fluid rate received, comparing the 51 children who received N/2 with the 51 who received NS (table 1) as would be expected from the randomisation.
Baseline clinical and biochemical characteristics of the children randomly assigned to receive either 0.45% saline (N/2) or 0.9% saline (NS)
The blood samples were analysed for the concentrations of sodium, potassium, bicarbonate, urea, and creatinine using ion selective electrodes, glucose using an oxygen rate method, and osmolality using freezing point depression. Urine sample collection via urine bag in incontinent children and clean catch specimens in toilet trained children was attempted for the determination of sodium and potassium concentrations, tonicity (urinary sodium plus potassium concentration), and osmolality. In addition, ketonuria was assessed by Ketodiastix (Bayer Clinitest 50, Bridgend, South Wales, UK) in the first urine specimen passed; the results were recorded as either absent, trace, small, moderate, or large. A sample of the first urine passed was collected in 76/102 children, in only 43 of whom was it passed between −1 and +2 hours of T0, consistent with this being a dehydrated population. In 36/43 children a subsequent urine specimen (U2nd) was obtained between 3 and 12 hours (median 4.8 hours) after T0, allowing analysis of the change in electrolytes and osmolality.
The short term response of plasma and urinary electrolytes and osmolality to treatment was analysed according to whether the children were hyponatraemic (plasma sodium <135 mmol/l) or normonatraemic at T0. A change in plasma sodium of ⩾2 mmol/l was considered to be biochemically significant as this exceeds the coefficient of variation (CV) of the assay for the laboratory reference range of 135–145 mmol/l (CV 1.3–1.5%).
To gauge the prevalence of hypo- or hypernatraemia during prolonged fluid administration, plasma and urinary data in 42/102 children (22 N/2) whose IV fluids were continued for >4 hours were analysed in each child. Variable data on each child were available (between 8 and 31 hours after T0) depending on the duration of IV infusion.
Statistical analysis
All statistical analyses were performed using the Statistical Package for Social Sciences (SPSS Inc., Chicago, IL, version 11.0 for Windows). Results were expressed as either mean (SD) or median (range) unless otherwise indicated. Means between groups were compared by independent t tests and paired variables by paired sample t tests. Medians were compared by the Mann-Whitney U test and changes over time were compared by the Wilcoxon signed rank test. Categorical data were analysed using cross tabulation and the χ2 test or Fisher’s exact test if two cells had expected counts less than 5. Statistical significance was defined as a p value less than 0.05.
RESULTS
Baseline clinical and biochemical characteristics
The mean (SD) plasma sodium concentration at T0 in the 102 children was 135 (3.3) mmol/l (range 124–142). Thirty seven of the children (36%) were hyponatraemic at T0, four of whom had a plasma sodium concentration less than 130 mmol/l. The median length of illness prior to presentation was longer in the hyponatraemic children (2 days, range <24 hours to 5 days) compared with the normonatraemic children (1 day, range <24 hours to 7 days; p < 0.01) and the mean BMI SDS was lower (−0.7 (1.2) v −0.1 (1.1); p < 0.01). Comparing the children who were hyponatraemic versus those who were normonatraemic at T0, there were no differences in age (mean 2.8 (1.3) years v 2.9 (2.0) years; p = 0.72), sex (51% v 46% male; p = 0.61), percent dehydration (median 5% (range 3–7) v 5% (range 3–7); p = 0.27), rotavirus positivity (12/13 v 18/22 tested; p = 0.74), or the type (43% v 53% N/2; p = 0.30) or rate (78% v 75% RRP; p = 0.73) of intravenous fluids subsequently received.
The first urine was passed a median of 2.3 hours (range −1.0 to 13.5) after starting intravenous fluids. In the 76/102 in whom this was collected, the median urinary sodium concentration was higher in samples containing “moderate” or “large” ketones (57/76; 58 mmol/l, range <10–209) compared with those that were negative for ketones or had only trace or small amounts (19/76; 20 mmol/l, range <10–109; p < 0.01).
In the 43 children for whom a urine sample was passed and obtained within 2 hours of T0, the median urinary osmolality was 971 mOsm/kg (range 315–1290 mOsm/kg), median urinary sodium concentration was 58 mmol/l (range <10–209 mmol/l), and median urinary potassium 71 mmol/l (range 13–232). The median urinary tonicity (urinary concentrations of sodium + potassium) was 161 mmol/l (range 19–300), approximately that of normal saline (154 mmol/l). The urinary sodium, tonicity, and osmolality were similar in the NS (20/43) and N/2 (23/43) groups (table 1) and were independent of whether children were hyponatraemic (16/43) or normonatraemic (27/43) at baseline (hyponatraemic versus normonatraemic children: median urinary sodium 52 (range <10 to 204) v 70 (range <10 to 209), p = 0.39; median urinary tonicity 131 mmol/l (range 19 to 285) v 163 mmol/l (range 22 to 300), p = 0.1; median urinary osmolality 935 (range 315 to 1290) v 1036 (range 356 to 1239), p = 0.35). The median urinary potassium however was lower in the hyponatraemic children (68 (range 13–91) v 89 (range 16–232), p = 0.03).
Effect of IV fluid infusion rate on change in plasma sodium
The infusion rate (RRP versus SRP) was not a determinant of the change in plasma sodium in either treatment arm.
In the NS group, those treated with the RRP (38/51) had a median change in sodium of +1 mmol/l (range −7 to 6) versus SRP +2 mmol/l (range −1 to 8) (p = 0.08). In children receiving N/2 the median change in plasma sodium in those who received RRP (40/51) was −1 mmol/l (range −6 to +2) versus −1 (range −5 to +3) in those treated according to the SRP (p = 0.92, Mann-Whitney U test).
Effect of IV fluid type on plasma sodium at T4
The plasma sodium response to N/2 versus NS differed depending on whether the children were hyponatraemic or normonatraemic initially.
After 4 hours rehydration with N/2, the mean plasma sodium had not changed in the hyponatraemic children (p = 0.32) but had decreased significantly in the initially normonatraemic group (p < 0.001; table 2, fig 2). In the normonatraemic group, plasma sodium decreased by ⩾2 mmol/l in 51% (18/35) compared with 13% (2/16) in the hyponatraemic group (p < 0.001; table 2). In 20% of the initially normonatraemic children (7/35), the fall was ⩾5 mmol/l. The maximum decrease was 6 mmol/l in two children treated with N/2 by RRP. The maximum increase in plasma sodium over 4 hours was 3 mmol/l in a child treated with N/2 by SRP.
Mean (SD) plasma sodium and osmolality at baseline (T0) and after 4 hours of intravenous rehydration (T4) in the initially hyponatraemic (plasma sodium <135 mmol/l) versus normonatraemic (plasma sodium 135–145 mmol/l) children who received either 0.45% saline + 2.5% dextrose (N/2) or 0.9% saline + 2.5% dextrose (NS)

{kind=link}
{kind=link}
Box plots showing the plasma sodium concentration at baseline (T0; shaded) and after 4 hours (T4; white) infusion of either N/2 or NS in (A) all children and those who were either (B) hyponatraemic or (C) normonatraemic prior to starting IV fluids. Box plots show the mean (solid horizontal line), median (dashed horizontal line), interquartile range (box limits), and minimum and maximum (whiskers), except that extreme outliers (greater than 1.5 box lengths from the edge of the box) are shown as individual data points. In the N/2 group, mean plasma sodium concentration did not change in the initially hyponatraemic children and decreased in the initially normonatraemic children. In the NS group however, mean plasma sodium increased in the hyponatraemic children and did not change in the normonatraemic children. No child became hypernatraemic. *Paired t test T4v T0.
In contrast, after 4 hours rehydration with NS, there was a mean increase in plasma sodium of 2.4 (1.5) mmol/l in children who were initially hyponatraemic (p < 0.001) compared with no significant change in the normonatraemic group (p = 0.08; table 2, fig 2). Thirteen per cent (4/30) of the normonatraemic group and none of the hyponatraemic group experienced a decrease in plasma sodium of ⩾2 mmol/l (table 2). The maximum decrease in plasma sodium concentration was 7 mmol/l (140 to 133 mmol/l) in a normonatraemic child, in whom fluids were discontinued at completion of the RRP; it was associated with an inappropriately high urinary sodium concentration in concentrated urine at 6 hours (urinary sodium 76 mmol/l, potassium 94 mmol/l, tonicity 170 mmol/l, osmolality 885 mOsm/kg). The maximum increase in plasma sodium over 4 hours was 8 mmol/l, from 124 to 132 mmol/l in a child treated with NS by SRP. Plasma osmolality changes in all groups were consistent with changes in plasma sodium (Table 2).
Response of urinary sodium, tonicity, and osmolality to IV fluids
To assess the response of urinary electrolytes and osmolality to IV fluids, only the 36 children with a baseline (Ubase) and subsequent (U2nd) urine sample were analysed (table 3). Apart from being slightly older than the rest of the study group (median 3.8 years (range 1.1–11.9) v 2.0 years (range 0.8–7.5); p < 0.001), the 36 children’s clinical and biochemical data (T0 and T4) were comparable with the group as a whole. Nineteen received NS and 17/36 received N/2. Eight children in each group were hyponatraemic at T0.
Response of urinary sodium, potassium, tonicity (Na + K), and osmolality to either N/2 or NS, according to whether the children were hyponatraemic or normonatraemic at T0 in the 36 children in whom a baseline urine sample (Ubase) was collected within 2 hours of T0, and a second sample (U2nd) was collected a median of 4.8 hours (range 3–12) after T0
Irrespective of the fluid received or the plasma sodium at T0, urinary potassium concentration decreased (table 3), which would be consistent with a decrease in aldosterone secretion following volume expansion. In contrast, the urinary concentration of sodium in the second sample varied according to the initial plasma sodium concentration and the fluid received. The urinary concentration of sodium decreased in the hyponatraemic children treated with NS and tended to do so in those receiving N/2 (table 3), whereas it increased in the normonatraemic children receiving NS and did not change in those receiving N/2 (table 3).
In keeping with the changes in concentration of sodium and potassium, the median urinary tonicity of the second urine sample had decreased significantly in the hyponatraemic children (table 3) to less than that of half normal saline. In the normonatraemic children, the median urinary tonicity decreased, but remained above that of half normal saline in the N/2 group and remained approximately that of normal saline in the NS group.
Median urine osmolality decreased in both treatment groups irrespective of the initial plasma sodium (table 3).
Biochemical changes during more prolonged fluid administration
Forty two children (22 N/2 and 20 NS) received IV fluids for more than 4 hours. These comprised all 24/102 children who were treated according to the SRP (table 1) plus 18/78 (11 N/2, 7 NS) who completed the RRP but continued IV fluids according to the SRP because of continued vomiting or poor oral fluid intake. Plasma biochemistry at T4 was similar to that of the group as a whole (data not shown). Plasma sodium concentrations were available at 24 hours in 16 children (8 N/2) who continued to receive at least half of their maintenance requirement of fluid15 intravenously, at which time no child receiving NS had a plasma sodium <135 mmol/l (range 135–142 mmol/l) compared with 3/8 of the N/2 group (range 131–140 mmol/l). The maximum increase in plasma sodium over 24 hours was 12 mmol/l to 136 mmol/l in a child receiving NS.
To gauge the potential for clinically significant dilutional hyponatraemia among the 42 children who received prolonged IV fluids, each individual’s longitudinal biochemical data were studied. Five of the 22 treated with N/2 but none treated with NS (N/2 v NS: p = 0.03, Fisher’s exact test) had persistent significant hyponatraemia (sodium ⩽131 mmol/l) or falls in plasma sodium ⩾4 mmol/l to below 135 mmol/l associated with an inappropriately high urinary sodium content (range 30–140 mmol/l) and urine osmolality higher than plasma osmolality (range 462–1058 mOsm/kg), suggesting that they were at risk of dilutional hyponatraemia. The plasma and urinary abnormalities were documented to persist for a median of 19 hours (range 8–27).
As no child who received prolonged NS developed this problem, we analysed data from the 22 children who received N/2 for more than 4 hours to identify potential clinical or biochemical predictors that could allow early detection of those at risk. Comparing the five children who developed significant dilutional hyponatraemia with the remaining 17/22, no clinical or biochemical parameters emerged that would allow early identification of those at risk, except for continuation of IV fluids beyond 4 hours after completion of the RRP (completion of RRP: 5/5 affected v 6/17 unaffected; p = 0.04). Apart from a slightly higher median urea (6.8 mmol/l (range 5.3–9.1) v 5.1 mmol/l (range 1.2–8.7); p = 0.02) suggestive of more severe dehydration, there were no differences in their median age (p = 0.09), BMI SDS (p = 0.24), estimated degree of dehydration (p = 0.54), length of illness prior to presentation (p = 0.49), baseline plasma sodium (p = 0.82), bicarbonate (p = 0.09), or creatinine (p = 0.14). Three of the five children had stool cultures performed, all of whom were positive for rotavirus.
DISCUSSION
Recently, the basis for the use of intravenous hypotonic saline solutions in sick children has been questioned and it has been suggested that the use of isotonic saline solutions might decrease the frequency of iatrogenic hyponatraemia.1,2,13 In this prospective, randomised study we have shown that when children with gastroenteritis are treated with intravenous fluids, hyponatraemia is less likely to develop or persist if an isotonic rather than hypotonic saline solution is used.
The baseline clinical and biochemical characteristics of the 102 children in our current report were similar to those in our previous study.12 Hyponatraemia was common at presentation (36%). This has been attributed to the sodium content of diarrhoeal losses19,20 and low salt intake;19 but the inappropriately high urinary sodium content we again documented at presentation may also contribute. The relationship we observed between the sodium concentration in the first urine sample passed and the degree of ketonuria suggests that the excretion of ketones as sodium salts may have contributed to the relatively high urinary sodium concentrations, consistent with reported association between natriuresis and starvation.19,21
What is already known on this topic
-
Hyponatraemia in hospitalised children, including those with gastroenteritis, is common and can be associated with cerebral oedema and death
-
Hypotonic saline solutions are frequently used in children and have been suggested to contribute to the development of hyponatraemia
Non-osmotic ADH activity is thought to underlie the development of hospital acquired dilutional hyponatraemia by preventing the excretion of electrolyte free water during fluid administration.3,22 Gerigk and colleagues23 documented raised ADH levels independent of osmolality in children with a variety of common acute childhood illnesses and we have reported that osmotically inappropriate ADH activity is common and persistent in children with gastroenteritis.12 Consistent with this, the biochemical response to N/2 was almost identical in this and our previous study12 in which all of the children received N/2. In both studies, the mean plasma sodium concentrations of children who were initially normonatraemic decreased, and those of children who were hyponatraemic did not improve in response to N/2. Half the normonatraemic children and 13% of the hyponatraemic children treated with N/2 experienced a decrease in plasma sodium ⩾2 mmol/l, and after 24 hours, 3 of 8 children largely dependent on IV fluids were hyponatraemic. In contrast, the use of isotonic saline over 4 hours resulted in maintenance of plasma sodium in those initially normonatraemic and an increase in those initially hyponatraemic. None developed hypernatraemia. After 24 hours, all 8/51 children still receiving normal saline were normonatraemic. Five of the 22 (23%) who received prolonged half-normal saline displayed biochemistry suggestive of dilutional hyponatraemia, compared with none of the 20 treated with normal saline. These findings suggest that in children with gastroenteritis, the use of hypotonic fluids exacerbates the tendency to develop hyponatraemia whereas the use of isotonic saline is protective.
The urinary biochemistry may provide some basis for understanding the decreased risk of hyponatraemia in children given isotonic saline and is reassuring with respect to the risk of hypernatraemia. As seen in our previous study,12 despite mild to moderate dehydration and irrespective of the plasma sodium concentration, the median urinary sodium concentration at presentation approximated that of half-normal saline and the urinary tonicity approximated that of normal saline. Urinary tonicity is a better reflection of free water clearance than urinary osmolality24 because an important component of osmolality is urea, which readily crosses cell membranes and therefore does not influence water movement. Administration of a fluid of lower tonicity than that of the urine being passed is predicted to result in a decrease in plasma sodium concentration because of the retention of free water implicit in the excretion of urine with a higher tonicity. After several hours of IV fluids, the urinary potassium decreased in all children in our study and the median urinary sodium concentrations of the hyponatraemic children in both treatment groups had decreased to levels consistent with maximal renal conservation of sodium (approximately 20 mmol/l;25,26 table 3); thus the urinary tonicity of the hyponatraemic children had decreased to less than the tonicity of N/2. As a result, the plasma sodium concentrations of the hyponatraemic children receiving hypotonic saline were maintained (but not improved) over 4 hours, whereas plasma sodium increased in the hyponatraemic children who received NS, a fluid roughly isotonic with respect to their initial urinary tonicity. The normonatraemic children on the other hand, did not conserve sodium. Although urinary potassium excretion decreased in these children, the median urinary concentration of sodium was unchanged in the N/2 group and increased in the NS group. The normonatraemic children treated with N/2 therefore continued to excrete urine that was hypertonic relative to the infused fluid. This would explain the accompanying decrease in plasma sodium concentration. Those given NS continued to excrete urine isotonic with respect to the infused fluid and maintained their plasma sodium concentration unchanged.
What this study adds
-
Biochemical evidence shows that in children with gastroenteritis, hypotonic saline solutions exacerbate the tendency to develop dilutional hyponatraemia while isotonic saline solutions are protective
-
Urinary biochemistry suggests that isotonic solutions are safe because hyponatraemic children retain sodium and normonatraemic children excrete it appropriately
The basis of the greater renal avidity for sodium in the hyponatraemic compared with the normonatraemic children is unclear. A similar phenomenon has been described in rats infused simultaneously with normal saline and ADH, in whom those fed a salt poor diet prior to the infusion were better able to retain sodium and maintain their plasma sodium than those whose dietary content of salt had been normal.27 The median duration of illness was longer in the hyponatraemic children and therefore, in addition to more prolonged sodium losses in diarrhoeal stools19 and urine,12 their dietary intake of sodium is likely to have been lower than for those children who were normonatraemic at presentation. Relatively chronic sodium depletion therefore may have promoted the development of renal adaptive responses, resulting in more rapid reversal of the natriuresis evident at presentation. Differential suppression of aldosterone activity in the normonatraemic versus hyponatraemic children during fluid therapy might have contributed if the hyponatraemic children were more dehydrated at baseline; however there were no clinical or biochemical data to support this. Furthermore, the similar decrease in urinary potassium in the hyponatraemic and normonatraemic children and significant decrease in urinary sodium concentration in the hyponatraemic children treated with NS but not N/2 suggests that mechanisms other than aldosterone were acting.
We conclude that when intravenous fluids are deemed necessary in children with gastroenteritis, isotonic saline solutions with appropriate glucose content should be used. The question arises however as to whether this recommendation should be restricted to gastroenteritis. Non-osmotic stimulants of ADH secretion (such as nausea and vomiting, pain, and metabolic stress)28 are common and likely to be active in a variety of clinical situations for which intravenous fluids are used. The protective effect of normal saline against the development of hyponatraemia and the ability of the normonatraemic children to increase urinary sodium excretion suggest that broadening the use of isotonic fluids with appropriate glucose content should be considered.
Acknowledgments
We thank Ms Kate Lyle (RN), the study coordinator, without whose hard work and dedication the study would not have been possible. The authors gratefully acknowledge the financial support from the Sydney Children’s Hospital Foundation and the Department of General Paediatrics, Sydney Children’s Hospital in conducting this study.
REFERENCES
Footnotes
-
Published Online First 13 December 2005
-
Competing interests: none declared
Linked Articles
- Atoms