Article Text

Abstract
Aim: To assess the Scottish newborn screening programme for congenital hypothyroidism from 1994 to 2003 (period 2) for performance and compare with an initial audit covering 1979 to 1993 (period 1).
Design: Performance data—age at blood spot sampling, notification by screening laboratory, start of treatment, and the prevalence of late testing, notification or treatment—were compared, together with the incidence of congenital hypothyroidism.
Results: Comparing data for period 2 with period 1, the mean annual incidence of true congenital hypothyroidism was 1:3655 live births v 1:4363. Median age for Guthrie sampling (all referrals) was 6 v 7 days (p<0.0001). Late sampling (>10 days) had fallen from 10.7% to 7%. For infants requiring repeat sampling before notification, the median (range) interval between initial and final repeat samples was 11 (1 to 52) compared with 14 (3 to 73) days. Median age at notification for true congenital hypothyroidism was 10 v 12 days (p <0.0001). Late notification (>15 days) was justifiable (mild TSH elevation) in 10 of 13 patients in period 2. Median age at start of treatment for true congenital hypothyroidism had improved to 11 days from 13.5 days. For true congenital hypothyroidism, late treatment (>16 days) occurred in 7% of patients compared with 19% (p<0.0001).
Conclusions: There has been an improvement in performance measures for the congenital hypothyroidism screening programme in Scotland. However, late sampling, occurring primarily in inpatients and which is never justified, remains a problem, while the interval between initial and recall sampling is a further source of delay.
- IRMA, immunoradiometric assay
- RIA, radioimmunoassay
- TFT, thyroid function test
- TSH, thyroid stimulating hormone
- congenital hypothyroidism
- screening
Statistics from Altmetric.com
- IRMA, immunoradiometric assay
- RIA, radioimmunoassay
- TFT, thyroid function test
- TSH, thyroid stimulating hormone
Congenital hypothyroidism is a relatively common disorder, with an incidence of 1:3000 to 1:3500 in white populations.1,2 Severe untreated congenital hypothyroidism leads to profound mental impairment and growth failure (cretinism). Detection and treatment within the first few weeks of life will prevent severe cognitive impairment3,4 but clinical diagnosis can be difficult in this period. The finding that thyroid hormones and thyroid stimulating hormone (TSH) could be measured in cord blood5 paved the way for newborn screening, which was first introduced in 19746 using neonatal heel prick blood samples, a technique pioneered by Guthrie and Susi for phenylketonuria screening.7 Congenital hypothyroidism screening is now universally accepted as being both clinically and cost effective. Indeed, the American Office of Technology Assessment has reported congenital hypothyroidism screening to be one of the few programmes of preventative medicine in public health to have a positive cost–benefit ratio (of 10:1).8
Screening for congenital hypothyroidism began in Scotland in 1979. A 1979–1993 audit reported favourable median ages for Guthrie sampling (7 days), notification by the screening laboratory (12 days) and initiation of thyroxine treatment when indicated (13.5 days).9 However, 37 (10.7%) of the 347 infants referred had their initial Guthrie sample taken after 10 days of age, while 45 (13%) of the cohort did not start treatment until more than 20 days after birth. The audit concluded that the programme could be improved if Guthrie sampling was undertaken earlier and more consistently. It was also recommended that all infants in hospital, regardless of feeding status, gestation, or sickness, should have a congenital hypothyroidism screening sample taken by day 5. In this report we present new data from 1994–2003 and compare our findings with those from the first audit.
METHODS
Subjects
Data on all infants referred with TSH elevation by the Scottish Newborn Screening Laboratory have been kept since screening began in August 1979. Information is collected using a structured proforma recording details of demographics, birth history, screening data, thyroxine treatment, biochemistry, and growth. In 1992 a computerised database (Borland Paradox v3.5, upgraded to Microsoft Access in 2001) was established to facilitate continuing follow up of individuals with congenital hypothyroidism and screening programme audit. Clinical data was held and reviewed by the clinical team. As this was an audit, no research ethics committee approval was required or sought. We have termed the first audit (1979 to 1993) period 1 and the current audit (1994 to 2003) period 2.
Blood spot TSH assay
Guthrie screening tests, calibrated against whole blood, are carried out on dried, whole blood spot samples. In 1994 an immunoradiometric assay (IRMA) was used. This was superseded by a time resolved, dissociation enhanced, lanthanide fluorescent immunoassay (DELFIA) for neonatal human TSH in 2002. Approximately 4000 assays were done in parallel, so that the DELFIA ranges established for normal, borderline, and raised TSH are equivalent to the ranges used with the IRMA, such that the actual sensitivity of the screening test is unaltered.
Since 1979 the laboratory values for normal, borderline, and raised TSH in milliunits per litre (mU/l) have varied according to the assay used, as follows: Corning RIA (1979–1982), <25, 25–49, ⩾50; in-house RIA (1982–1989), <15, 15–39, ⩾40; IDS IRMA (1989–2002), <10, 10–39, ⩾40; PerkinElmer DELFIA (2002 to present), <8, 8–24, ⩾25.
In 1985 and 1986 problems occurred with the supply of anti-TSH antibody.
Protocol for referral by the screening laboratory to the clinician
Samples are tested within two working days of receipt. Using the reference or “cut-off” values given above, results are reported as normal, borderline, or abnormal. If the TSH value is frankly abnormal the laboratory informs the responsible clinician by telephone as a matter of urgency. This process is termed notification. For repeat samples, if the TSH is equal to or greater than the lower limit of the borderline range, notification automatically ensues. Since 1989 the first point of contact has been the clinical coordinator (or designated deputy) or regional paediatric endocrinologist, who then contacts the relevant paediatrician, requesting that the infant is recalled for confirmatory venous thyroid function tests (TFTs) within 24 hours of notification. The need for further diagnostic tests and the decision whether or not to treat the infant are at the individual clinician’s discretion. Since 1979, Grampian region has offered 131I isotopic scanning for all referred patients. Combined isotope (technecium99) and ultrasound thyroid scanning (hereafter referred to as “dual scanning”) was introduced in the West of Scotland in January 1999.
Diagnostic categories
We have previously devised criteria for distinguishing between true congenital hypothyroidism and transient TSH elevation.9 This is important given that transient TSH elevation may occur in sick newborn infants.10 Our four diagnostic categories are definite and probable (“true”) congenital hypothyroidism, transient TSH elevation, and status uncertain (table 1).
Diagnostic categories and inclusion criteria for congenital hypothyroidism used in Scotland
Statistics
Annual live birth data were obtained from the General Registrar’s Office of Scotland. We used χ2 tests to compare proportions of interest between periods 1 and 2. Mann–Whitney tests were used for comparisons between continuous variables. Analyses were done using Minitab (Version 13) with a significance level of 5%. For the purposes of audit we defined late Guthrie sampling as occurring after day 10, late notification as occurring after day 15, and late treatment as starting after day 16.
RESULTS
Table 2 shows the annual number of live births and Guthrie tests carried out by the screening laboratory in Scotland from 1979 to 2003. The number of tests exceeds live births each year, owing to repeats, except in 1979 when screening began in August, and in 1980 when screening coverage was significantly below 100%. Figures are available for screening uptake from 2000–2003 and show a small number of parental refusals, ranging from 15 to 45 (0.028% to 0.09%),11 giving a mean population coverage of the Scottish congenital hypothyroidism screening programme of 99.95%.
The number of live births, Guthrie tests carried out, infants with true (definite and probable) congenital hypothyroidism or transient TSH elevation, and incidence of true congenital hypothyroidism by year is given for period 1 and period 2
Prevalence of congenital hypothyroidism
In period 2, when the live birth rate in Scotland declined by around 17%, the prevalence of true congenital hypothyroidism increased to a mean (range) of 1:3655 (1:2698 to 1:4619) live births, compared with 1:4363 (1:2885 to 1:7312) during period 1. The χ2 test for trend to the changing incidence of true congenital hypothyroidism from 1980 to 2003 failed to reach statistical significance (p = 0.07).
Initial categorisation of infants notified by screening laboratory
The screening laboratory issued notification for a total of 250 infants (table 3) in Period 2. No pre-treatment venous samples were taken in 15 (6%) infants, preventing initial categorisation, but subsequently 12 satisfied the criteria for true congenital hypothyroidism and two for transient TSH elevation.
Perinatal data according to diagnostic categories in infants referred with raised TSH on neonatal screening during periods 1 and 2
Aetiology and sex ratio of true congenital hypothyroidism
From 1979 to 2003 the overall female to male ratio for true congenital hypothyroidism was 2.1:1. Ascertainment of the aetiology of congenital hypothyroidism improved during period 2 with the adoption of dual scanning in the West of Scotland in January 1999: from 1994 to 1998 aetiology was known in 25 of 77 patients (32.5%), rising to 64 of 84 patients (76.2%) from 1999 to 2003 (table 4). The diagnostic breakdown in patients with known aetiology was thyroid ectopia in 32.9%, athyreosis in 29.1%, hypoplasia in 11.4%, and dyshormonogenesis in 26.6%.
Aetiology of true congenital hypothyroidism for period 2, before the introduction of dual scanning (pre-1999) in the West of Scotland and after the introduction of dual scanning (from January 1999)
Age at Guthrie sampling
Figure 1 shows the age in days at which the initial blood spot sample was taken for all infants referred. Median age (range) of sampling was 6 days (range 1 to 76) compared with 7 days (1 to 56) in period 1 (p<0.0001).
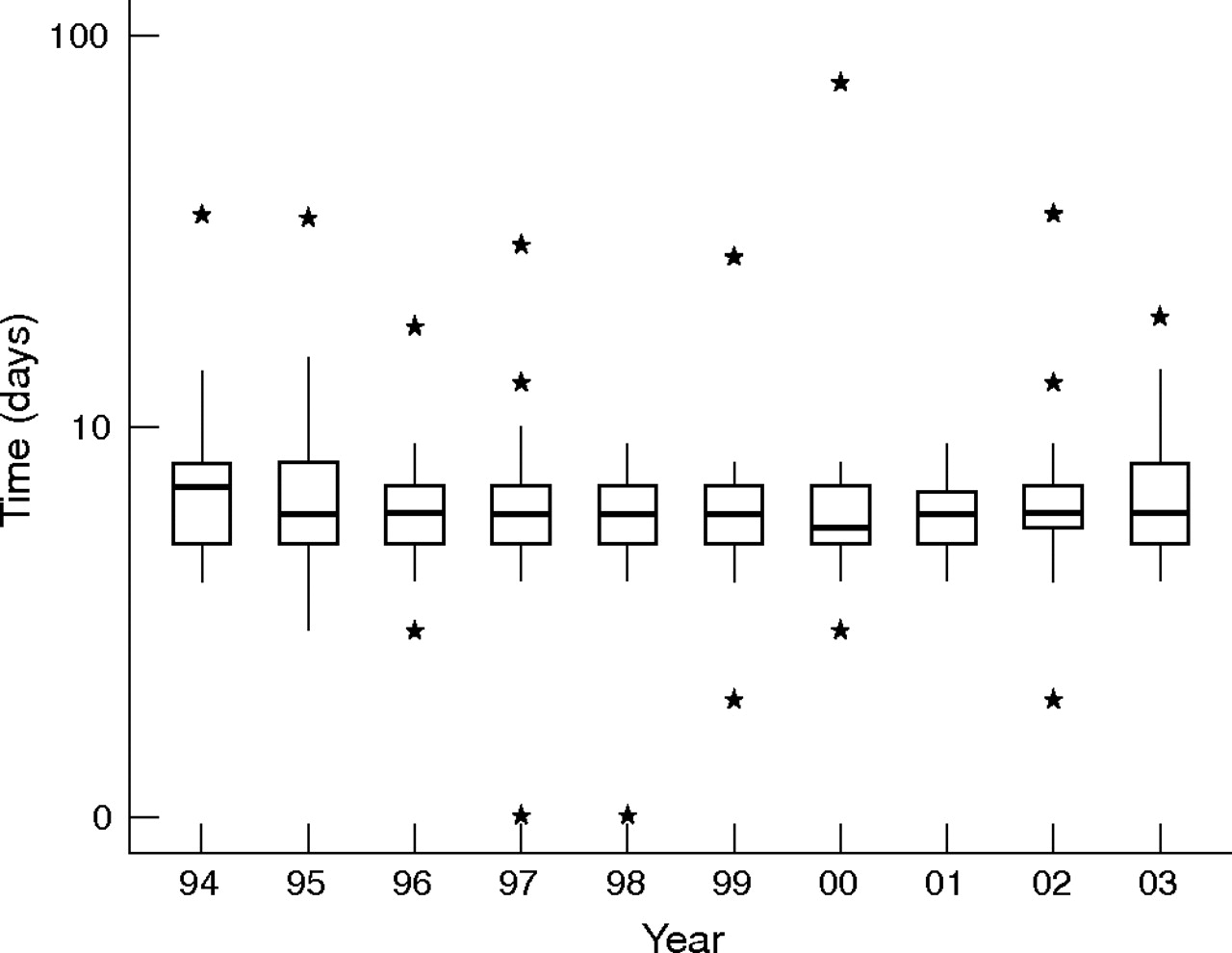
Box and whisker plot of log of age in days at first Guthrie sample, for all infants with raised TSH detected by the Scottish congenital hypothyroidism screening programme, by year for period 2. The boxes represent the interquartile range with a horizontal line at the median value. The vertical line (whisker) indicates the range. Individual outliers are shown as asterisks. TSH, thyroid stimulating hormone.
Late Guthrie sampling (>10 days) occurred in 17 of 250 infants (7%) referred, compared with 36 of 344 (10.5%) during period 1. All but one of these 17 infants, which included two with true congenital hypothyroidism, were sick at the time of sampling, six being preterm. In two infants, late sampling (27 and 31 days) was related to the need for urgent transfer between centres in the neonatal period. Median age (range) at sampling in these 17 patients was 15 (11 to 76) days, resulting in late notification (23 (16 to 78) days) and, in the 11 patients judged to require thyroxine, delayed treatment at a median of 21 (16 to 49) days.
For infants requiring repeat sampling before notification the median (range) interval between initial and final repeat sample was 11 (1 to 52) days (n = 58) compared with 14 (3 to 73) days in period 1 (n = 54).
Age at notification
Figure 2 shows age at notification in days for infants with true congenital hypothyroidism (excluding “other” causes) by year. Median (range) age was 10 (3–35) days compared with 12 (5–59) in period 1 (p<0.0001). Late notification (>15 days) occurred in 14 of 158 patients (8.9%) compared with 47 of 240 (19.6%) in period 1. Late notification was justifiable because of borderline TSH elevation in 11 of the 14 patients (78.6%).

Box and whisker plot of age in days at notification for infants with definite or probable congenital hypothyroidism by year, for period 2. The boxes represent the interquartile range with a horizontal line at the median value. The vertical line (whisker) indicates the range. Individual outliers are shown as asterisks.
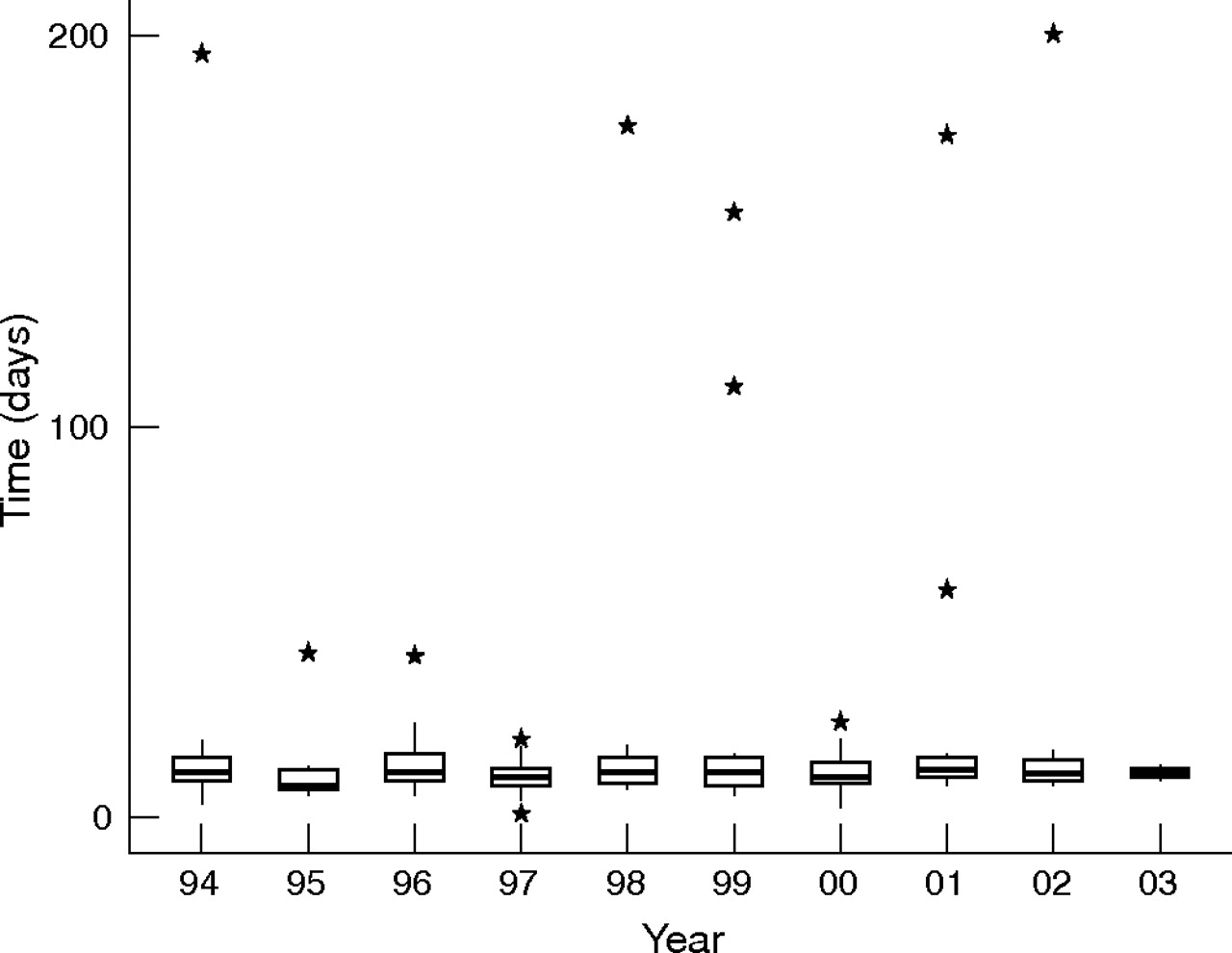
Age at starting treatment
Median (range) age at start of treatment for true congenital hypothyroidism (excluding “other” causes) was 11 (1 to 200) days (fig 3), compared with 13.5 (2 to 313) days for period 1 (p<0.0001). Six infants began treatment following clinical diagnosis before notification occurred, and two on the day of notification. Five of these had dyshormonogenesis, one had isoimmune thyroiditis, and one was exposed to radioiodine in utero. The remaining infant underwent venous TFT testing on day 3, before exchange transfusion, which revealed grossly abnormal results (TSH 555 mU/l, tT4 22 nmol/l). Treatment was started on day 6 while routine neonatal screening was carried out on day 5 with notification on day 7.
{kind=link}
{kind=link}
{kind=link}
Box and whisker plot of age in days at start of treatment for infants with definite and probable congenital hypothyroidism by year, for period 2. The boxes represent the interquartile range with a horizontal line at the median value. The vertical line (whisker) indicates the range. Individual outliers are shown as asterisks.
Late treatment (>16 days) occurred in 19 patients (12%) with true congenital hypothyroidism, compared with 66 (19%) in period 1. Seven of these 19 patients had frankly raised TSH on confirmatory TFT (median 94.2 mU/l, range 50 to 200). The delay in treatment was attributable to late venous sampling, with all seven patients starting thyroxine treatment on the same day that the TFT result was confirmed (median 20 days, range 17 to 24). The remaining 12 patients had modestly raised TSH (median 23.7 mU/l, range 10.36 to 52.0) and consequently began thyroxine later, at a median age of 84 days (range 18 to 200). Subsequent investigation in the 19 patients who were treated late showed dyshormonogenesis in four, ectopia in four, and hypoplasia in two, while the aetiology is still unknown in nine.
DISCUSSION
This audit, which is a temporal comparison of the performance of the Scottish congenital hypothyroidism screening programme, has coincided with the publication of two sets of newborn screening guidelines in the United Kingdom: NHS Quality Improvement Scotland12 and the UK Newborn Screening Programme Centre.13 The criteria set out in these guidelines are broadly similar. During period 2 the Scottish criteria have been met in terms of screening coverage (>99.5%), while timely sampling (<8 days) was achieved in 93.8% of our cohort and targets for notification and starting treatment (<14 days) in 87.6% and 82.0%, respectively.
The mean coverage of the Scottish congenital hypothyroidism screening programme (99.95%) compares favourably with other published data from New Zealand (95%),14 Netherlands (99.5%),15 Western Australia (99%),16 and California (98.6%).17 Coverage in other areas of the UK varies from 97.4% in Merseyside18 and 99.8% in Wales19 to “over 99.9% in three districts outside London”.20
The widely recognised female preponderance of true congenital hypothyroidism is evident in our cohort, consistent with previous studies.17,19,21,22 The apparent increase in the incidence of congenital hypothyroidism, which did not reach statistical significance, could be a chance finding, as the annual incidence of true congenital hypothyroidism varies widely (table 2). Alternatively, it is possible that a genuine, albeit small, increase in the incidence of congenital hypothyroidism has occurred in Scotland. It is interesting that studies from Western Australia,16 California,17 and Israel23 support the latter hypothesis.
The proportion of patients categorised as having transiently raised TSH decreased between periods 1 and 2. This partly reflects erroneous screening results during 1985/1986 when a particularly high proportion of patients (50.0% and 52.4%, respectively) were shown to have transient TSH elevation, attributable to assay problems (see Methods and table 2). Lesser peaks in 1988 (30.3%) and 1990 (28.6%) reflected an unusually high prevalence of prematurity and sickness among infants referred. A further factor is the decline in use of iodine containing products during period 2. A recent survey (1998–2001) did not find a single Scottish neonatal unit still using iodine containing skin antiseptics (Simpson J, personal communication).
We have found that dual scanning, when combined with other diagnostic information, improves the ascertainment of congenital hypothyroidism aetiology (Perry RJ, Maroo S, Maclennan AC, et al, submitted for publication). Importantly, thyroid imaging helps in clarifying the diagnosis of true congenital hypothyroidism when TFTs are equivocal or when there is no pretreatment venous sample, as was the case in 6% of referrals during period 2. However, we recognise that there are practical limitations to thyroid imaging and that biochemistry remains the parameter on which the need for thyroxine treatment must be based.
Despite an improvement in the median age at first Guthrie sample in neonates referred by the screening laboratory, delayed sampling continues to pose a problem, with 7% of the cohort sampled later than 10 days during period 2. This delay occurred predominantly in hospital inpatients.
We documented significant improvements of 2.0 days in the median age at notification for true congenital hypothyroidism and 2.5 days in the median age of starting treatment, accompanied by a reduction in the proportion of patients being treated late. Similarly, for the status uncertain and transient TSH elevation groups, median age at treatment fell. It is inevitable that infants with borderline TSH elevation will be treated late pending surveillance. Thyroid imaging has an important role in this situation and a diagnosis of “hyperthyrotropinaemia” should not be made until thyroid scanning has shown a normal sized gland in situ.
We conclude that the congenital hypothyroidism screening programme in Scotland is performing well, with improvement in outcome measures between the two audits. The importance of the initial confirmatory venous TFT cannot be overemphasised. All infants with an abnormal or borderline TSH result on screening should have serum TSH and T4 measurements, at recall, before the start of any treatment. Further improvement would be achieved by timely initial Guthrie sampling and we reiterate the need for all newborn infants who are retained in hospital to be sampled on day 5, irrespective of gestation, feeding status, or sickness, in line with Scottish National Services Division policy.13 Neonatal units should be particularly wary of overlooking Guthrie sampling when there are overriding clinical concerns or logistic complications. The introduction of pregnancy and newborn Screening Coordinators to Scotland in 2001 is likely to improve all aspects of newborn screening surveillance.
Finally, the delay in obtaining repeat samples in our screening programme requires attention. To encourage more rapid collection and submission of repeat samples, we propose setting a target of 90% of repeat samples being received by the laboratory by day 30 of life compared with the 82% found in period 2. To achieve this, the screening laboratory plans to send repeat requests 10 days after issuing an equivocal result, rather than after 14 days as was the case in period 2. In addition, other more rapid means of communication, such as facsimile and e-mail, are being used to improve communications between those responsible for care of the infant with raised TSH values at newborn screening.
What is already known on this topic
-
Newborn screening for congenital hypothyroidism has largely eradicated the severe, irreversible neurodevelopmental damage and reversible growth failure (cretinism) previously associated with congenital hypothyroidism
-
Newborn screening for congenital hypothyroidism is perceived as very beneficial, so that all developed countries and many developing countries, now operate a screening programme
What this study adds
-
The screening programme for congenital hypothyroidism in Scotland has improved in the subsequent 10 years, when compared with the first 15 years of the programme
-
A large proportion of neonates being sampled late (>10 days) are hospital inpatients; neonatologists need to beware of late sampling for conditions normally screened for early in life
Acknowledgments
We wish to thank members of the Scottish Paediatric Endocrinology Group (Professor Kelnar and Drs Ahmed, Bath, Greene, Hunter, Mayo, Schulga and Smail) and other paediatric colleagues from all over Scotland (Drs Ainine, Al Roomi, Barclay, A Blair, M Blair, Burt, Chapman, Cochrane, Coutts, Duncan, Farmer, Findlay, Galea, Goudie, Ibhanesebhor, Kinmond, Kurian, Loudon, MacDonald, Macmillan, Mitra, Ray, Shepherd, Simpson, Skeoch, Staines, Thompson, Turner, Van Ijperen and Whyte), for their patience and support with repeated requests for information concerning their patients with CH. We are indebted to Dr Lucy Reynolds, Pregnancy and Newborn screening coordinator for Greater Glasgow, for help and advice with the preparation of this manuscript. JJ acknowledges financial support from the Yorkhill Clinical Effectiveness Committee, the Yorkhill Audit Committee and Pfizer Ltd.
REFERENCES
Footnotes
-
Published Online First 4 April 2006
-
Competing interests: none declared