Article Text

Abstract
Background: Spinal injury in children is rare, and poses many difficulties in management.
Aims: To ascertain the prevalence of spinal injury within the paediatric trauma population, and to assess relative risks of spinal injury according to age, conscious level, injury severity score (ISS), and associated injuries.
Methods: Spine injured children were identified from the UK Trauma Audit & Research Network Database from 1989 to 2000. Relative risks of injury were calculated against the denominator paediatric trauma population.
Results: Of 19 538 on the database, 527 (2.7%) suffered spinal column fracture/dislocation without cord injury and 109 had cord injury (0.56% of all children; 16.5% of spine injured children). Thirty children (0.15% of all children; 4.5% of spine injured children) sustained spinal cord injury without radiological abnormality (SCIWORA). Cord injury and SCIWORA occurred more commonly in children aged ⩽8. The risk of spine fracture/dislocation without cord injury was increased with an ISS >25 and with chest injuries. The risk of cord injury was increased with reduced GCS, head injury, and chest injury.
Conclusions: Spinal cord injury and SCIWORA occur more frequently in young children. Multiple injuries and chest injuries increase the risk of fracture/dislocation and of cord injury. Reduced GCS and head injuries increase the risk of cord injury.
- AIS, Abbreviated Injury Scale
- GCS, Glagow Coma Score
- ISS, injury severity score
- RTC, road traffic crash
- SCI, spinal cord injury
- SCIWORA, spinal cord injury without radiological abnormality
- SCIWORA
- cervical spine
- epidemiology
- spinal injury
Statistics from Altmetric.com
- AIS, Abbreviated Injury Scale
- GCS, Glagow Coma Score
- ISS, injury severity score
- RTC, road traffic crash
- SCI, spinal cord injury
- SCIWORA, spinal cord injury without radiological abnormality
Spinal injury in the paediatric trauma patient can have catastrophic consequences. It has been reported previously that children have a different injury profile from adults,1 due to different anatomical and physiological features and exposure to different risk factors. The facet joints of the child’s vertebrae are aligned in a more horizontal fashion than in adults. The spine is thought to adopt a more adult alignment at between 8 and 10 years of age.1 The child’s head is relatively large, hence the fulcrum where flexion takes place is at a higher level than in adults (C2/3), and the neck muscles less well developed. Compliance is greater in the bones of children, increasing the likelihood of soft tissue injury without associated fracture. Positioning in motor vehicles and type of restraint may be expected to lead to different injuries in the paediatric population.
Many factors, ranging from patient anxiety, communication difficulties, and lack of clinician experience may make assessment of the paediatric spine difficult in the emergency room. Emergency physicians and paediatricians who care for injured children may need to make decisions regarding the risk of spinal injury to their patient partly based on degree of suspicion of injury. For children who are unconscious, decisions regarding further imaging, such as magnetic resonance, may need to be made in order to define the degree of damage, if any, to the spinal cord. Knowledge of the typical patterns of injury will help define those patients at highest risk and develop a directed approach towards the use of further imaging and patient care.
To date, no study has been published concerned with the prevalence of spinal injury across all spinal regions in a denominator paediatric trauma population. Two analyses of the National Pediatric Trauma Registry in the USA taken over two different time periods have investigated the prevalence of cervical spine injury.2,3 These studies showed a prevalence of cervical spine fracture in the denominator trauma patient (excluding burns patients) of 1.6% and 1.5% respectively, and a prevalence of cord injury of 35% and 28.6% respectively in those with cervical spine injury. Spinal cord injury without radiological abnormality (SCIWORA)4 was responsible for 17.3% and 18.9% of spine injuries respectively. Similar rates of cervical spine injury (2.2%), have been shown by other authors from a single trauma centre.5 Many studies have been published from specialist centres for spinal injuries, with predictably higher prevalences of cord injury (42–50%),6–12 and similar rates of SCIWORA. Motor vehicle accidents account for approximately 50% of paediatric spinal injuries in most series, followed by falls from a height. Head injuries are the commonest associated injury in all articles where this has been studied, but this also reflects the large number of articles concerned with cervical injuries alone.
The Trauma Audit & Research Network (TARN) Database contains data on 19 538 injured children collected from 1989 to 2000. Data are submitted from approximately 50% of the trauma receiving hospitals in England and Wales. The primary aim of this study was to analyse the database and identify, for the first time, the prevalence of spinal column and cord injury in a denominator trauma population. We aim to ascertain the relative risks for bony injury and for cord injury for different groups of patients according to age, mechanism, level of consciousness, injury severity, and associated injuries.
METHODS
Patient selection
The TARN database contains information on all trauma admissions with hospital stays of three or more days, all trauma deaths, all trauma admissions to intensive care or high dependency units, and all trauma referrals for further specialist care involving one or more participating hospitals. Patients over the age of 65 with isolated fractured neck of femur and patients with uncomplicated injuries are excluded. Injuries are coded according to the 1990 Revision of the Abbreviated Injury Scale (AIS).13 The database also contains information regarding the aetiology of the injury and Revised Trauma Score on admission.
Patients were identified from the database as those aged 15 or under with spinal injuries according to the AIS criteria. Patients with single isolated transverse or spinous process fractures were not placed in the fracture/dislocation group for analysis. The AIS coding system allows the level (C1–C3 or C4–C7) of cervical cord injuries to be identified, but not the level of cervical fractures in isolation. There is no differentiation between levels within the thoracic and lumbar regions. Unstable and stable fractures are not separately classified.
The Injury Severity Score (ISS) is an internationally accepted and validated tool for assessing the severity of a patient’s injuries, originally devised by Baker and colleagues.14 It is an anatomical rather than a physiological scoring system. The ISS is calculated using the AIS dictionary. In this, each injury is given a severity score from 1 (minor) to 6 (fatal).
The body is divided into six regions:
-
Head and neck
-
Face
-
Chest and thoracic spine
-
Abdomen, lumbar spine, and pelvic contents
-
Upper and lower extremities and pelvic girdle
-
External (that is, skin).
The single worst injury in each of the three most severely injured regions is squared. The sum of these three values is calculated to give the ISS. Any injury with a score of 6 automatically attracts an ISS of 75, the highest score possible (table 1).
Injury severity score
Attempts were made to retrieve missing data on the precise nature of the spine injury by contacting participating hospitals and searching through clinical notes, x ray reports, and postmortem reports.
Patients were divided into two age groups (0–8 and 9–15) for comparison due to the differences described in current literature.
Statistical analysis
Data were analysed using the Statistical Package for Social Sciences for Windows, Standard Version, release 10.0. Categorical variables such as the pattern of injuries were analysed using Pearson’s χ2 test. Fisher’s exact test was performed where the expected incidence was less than 5. Median ISS was compared using the Mann-Whitney U test. Relative risk ratios were calculated using EpiInfo, Version 6. Prevalences are given with 95% confidence intervals in parentheses throughout.
RESULTS
Prevalence and age associated patterns of spinal injury
Over the study period, 19 538 paediatric patients were admitted to participating hospitals with trauma for three days or more (see tables 2 and 3). Of these, 662 patients had one or more spinal injury according to the above criteria. This amounts to 3.4% of the total paediatric database (3.1–3.6%).
Patient and injury characteristics in the overall data set and spinal injury subsets
Relative risk ratios
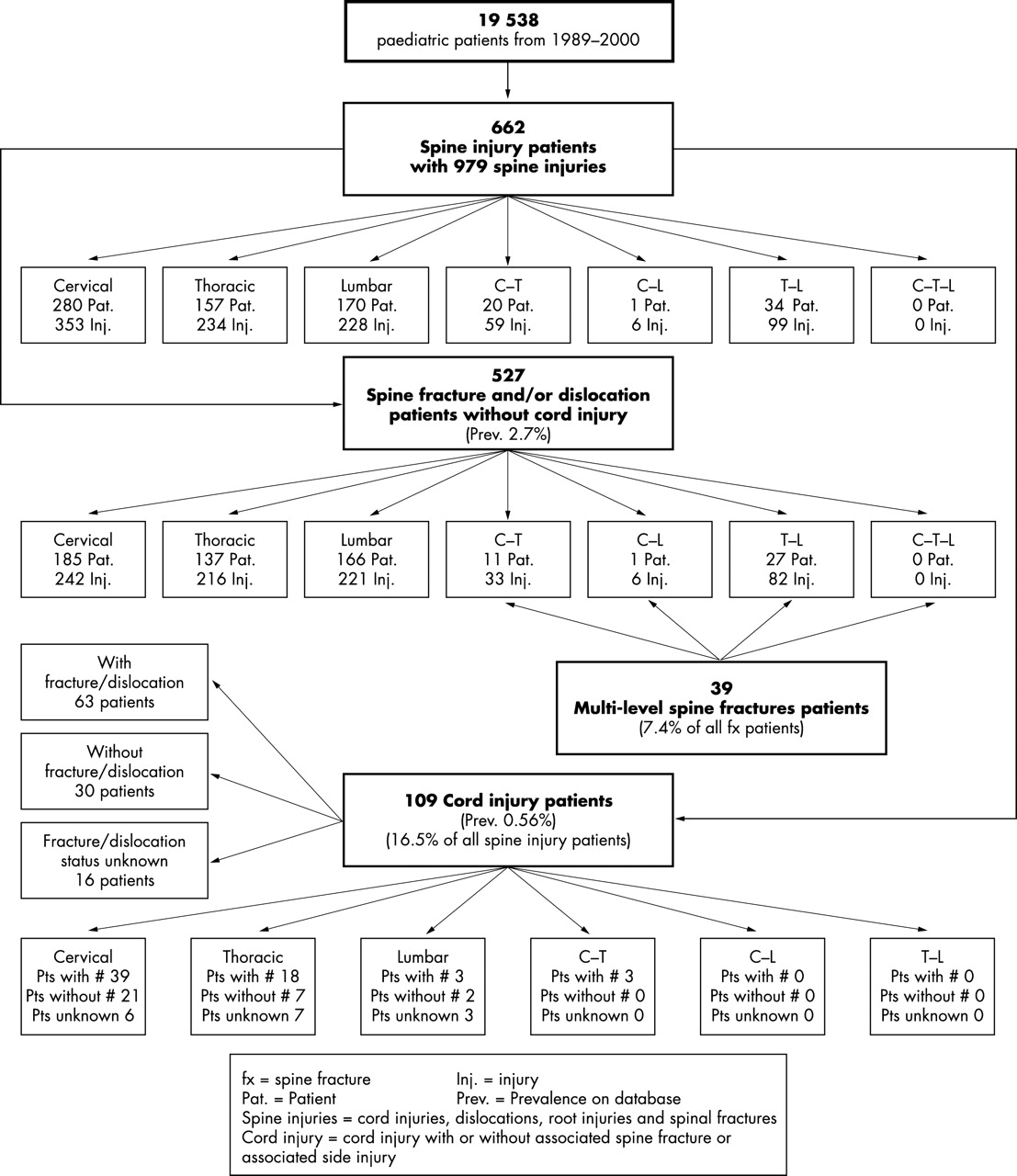
A flow diagram has been constructed to show the distribution of injuries within different regions of the spine (fig 1). Of these patients, 527 (79.6% (76.5% to 82.7%)) suffered a fracture or dislocation without associated spinal cord involvement at that level (spine fracture group). This gives a prevalence of 2.7% (2.5% to 2.9%) in children admitted to hospital with major trauma. A total of 7.4% (5.2% to 9.6%) of spine fracture/dislocation patients suffered multi-level injuries.
Pattern of injuries.
One hundred and nine patients received a spinal cord injury (SCI). This gives a prevalence of 16.5% (13.6% to 19.3%) of spinal cord injury in all paediatric spinal injuries, and of 0.6% (0.5% to 0.7%) of all paediatric trauma admissions. Thirty of these patients had no bony injury (spinal cord injury without radiological abnormality, SCIWORA): 4.5% (3.0% to 6.1%) of spinal injuries and 0.15% (0.10% to 0.21%) of all paediatric trauma admissions. On 16 patients, we were unable to establish whether or not a fracture had been present.
Nineteen patients (2.87% (1.6% to 4.14%) of all spine injuries; 0.1% (0.05% to 0.14%) of whole database) suffered isolated disc injury, nerve root injury, cauda equina injury, or transverse/spinous process fracture without other associated fracture or cord lesion at that level.
There was a significant difference in the pattern of spinal injuries across the two age groups (0–8 years and 9–15 years), with cord injury and SCIWORA occurring more commonly in the younger population (p < 0.001 for spine injuries, fractures, and cord injuries, and p = 0.03 for SCIWORA). When compared with the entire paediatric database, the relative risk of fracture or dislocation in those aged less than 9 was 0.37 (0.30 to 0.45; p < 0.001), the relative risk of cord injury was 1.00 (0.69 to 1.47; p = 0.98), and the relative risk of SCIWORA was 1.99 (0.96 to 4.13; p = 0.06). For those aged 9 or over, the relative risk of fracture or dislocation was 2.73 (2.23 to 3.36; p < 0.001), the relative risk of cord injury was 1.00 (0.68 to 1.45; p = 0.98), and the relative risk of SCIWORA was 0.5 (0.24 to 1.04; p = 0.06).
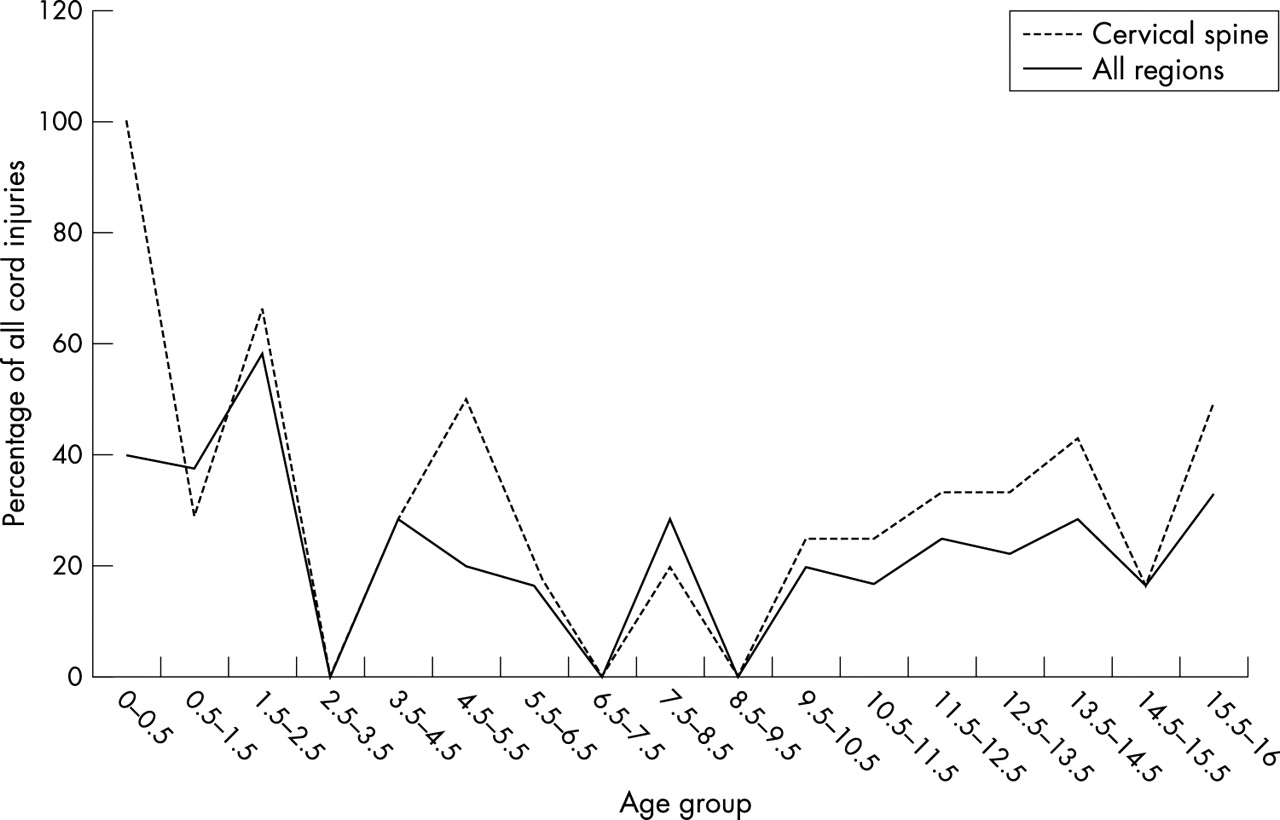
Assessing the prevalence of SCIWORA in children with cord injury across all age groups revealed that there was no clearly defined change in the prevalence at a given age. Rather, there was a gradual decline in the prevalence as children became older (fig 2).
{kind=link}
{kind=link}
Prevalence of SCIWORA.
There was a significant difference between the sex distribution of spinal injuries and that of other injuries across the whole database—387 (58.5%) of spine injured children were male compared to 13 170 (67.4%) of all children (p < 0.001), but there was no difference in the sex distribution of individual spinal injuries.
Mechanism of injury
Road traffic crash (RTC) was the commonest cause of injury across all groups (49.8% of all spinal injuries (46.0% to 53.7%)). The frequency of RTC rose in the SCI group (66.1% (57.2% to 74.9%)). The relative risk of sustaining a spine fracture without cord injury in an RTC against another mechanism of injury was 1.14 (0.97 to 1.35; p = 0.12). The relative risk of sustaining a cord injury in an RTC was 2.64 (1.78 to 3.92; p < 0.001).
Conscious level
The median Glasgow Coma Score (GCS) was 15 in all groups. The pattern of distribution of GCS shows two peaks in all groups, one at a GCS of 15, and the other at low levels of consciousness. This pattern is most marked in the cord injury group.
Data on GCS at admission was available for 16 727 patients (85.6% of total). The relative risk of spine fracture or dislocation without cord injury, with a GCS of 14 or less, excluding those with missing data was 0.98 (0.79 to 1.22; p = 0.86). In order to assess the effect of the missing data, assumptions were also made that that patients with missing data had firstly a GCS of 15, and then of 14 or less. Neither of these assumptions altered the suggestion that a decreased conscious level did not predispose to a spine fracture/dislocation without cord injury (if missing GCS were all 15, RR of fracture was 1.00 (0.8 to 1.23), and if 14 or less, RR was 0.96 (0.80 to 1.14)). However, the relative risk of cord injury with a GCS of 14 or less was 3.12 (2.02 to 4.82; p < 0.001). If all patients with missing data had a GCS of 15, this would still give a relative risk of 2.28 (1.55 to 1.37; p < 0.001).
Injury severity
Median injury severity score in all patients suffering spinal injuries was 9 (interquartile range (IQR) 4–21), which was the same as that seen in the total paediatric database (IQR 4–10). However, patients suffering spinal cord injuries had a higher median injury severity score than other injured children (26; IQR 16–47), showing that they comprised a different population (p < 0.001). The pattern of ISS was such that high ISS scores were more commonly seen in the spinal injuries and cord group. The relative risk of spinal fracture or dislocation with an ISS of 25 or greater was 1.59 (1.26 to 2.00; p < 0.001). The relative risk of cord injury with an ISS of 25 or greater was 15.70 (10.64 to 23.17; p < 0.001). Cord injuries automatically attract an AIS of 3 (contusion), 4 (incomplete cord syndrome), or 5 (complete cord syndrome or cord laceration), leading to a higher ISS. However, the relative risk of spine fracture with an ISS of 42 or above (that is, severe injuries in more than one body region) increases to 2.80 (1.78 to 4.40; p < 0.001), and the relative risk of cord injury with an ISS of 42 or above increases to 35.85 (24.39 to 52.68; p < 0.001).
Associated injuries
The prevalence of injuries in other body regions attracting an AIS of 2 or greater was studied in conjunction with the presence of spinal injuries.
The commonest associated injury in all groups was head injury, suffered by 24.9% (21.1% to 28.6%) of patients with spinal fracture/dislocation without cord injury and 49.5% (40.2% to 58.9%) of cord injured patients; 80.7% (70.5% to 91.0%) of cord injuries in this group occurred at the cervical level. The relative risk of spinal fracture or dislocation in the presence of head injury ⩾AIS 2 was 0.80 (0.66 to 0.97; p = 0.02). However, the relative risk of cord injury was 2.37 (1.63 to 3.45; p < 0.001). An AIS 2 head injury implies structural damage shown on CT scan or skull x ray.
Chest injury showed a more consistent relation with spinal injury; 11.4% (8.7% to 14.1%) of patients with spine fracture/dislocation also suffered chest injury, giving a relative risk of 2.30 (1.77 to 2.99; p < 0.001); 25.7% (17.5% to 33.9%) of cord injured patients suffered an AIS 2 or greater chest injury Again, the relative risk of cord injury in this group was also higher: 6.20 (4.05 to 9.48; p < 0.001; 77.4% (62.7% to 92.1%) of cord injuries in this group occurred at the cervical level.
There was no increase in the relative risk of either fracture/dislocation without cord injury (RR 1.37 (0.93 to 2.02; p = 0.11)), or of cord injury (RR 0.49 (0.12 to 2.00; p = 0.31)) with the presence of abdominal injury. Limb injuries were shown not to be associated with either type of injury (RR 0.19 (0.16 to 0.23; p < 0.001) for fractures/dislocations without cord injury, and RR 0.06 (0.03 to 0.12; p < 0.001) for cord injury).
DISCUSSION
This study has identified for the first time, mechanisms of injuries and injury patterns that have high associations with spinal column injury in the paediatric trauma population. In particular, we have identified factors that will be evident early within the presentation, to enable timely intervention in diagnosis and management of spinal injury. Specifically, we have identified aetiological factors (road traffic crash) and examination findings (depressed conscious level, head injury, chest injury, and multiple injury) which are associated with an increased risk of SCI, and findings that increase the risk of spine fracture (chest injuries and multiple injuries). Most paediatric limb injuries are isolated and are not associated with an increased risk of spine injury in this paediatric trauma population. We have also been able to establish the pattern of injuries seen throughout the spinal column for the first time in multiple, non-specialist centres (fig 1).
In our series, 7.4% of children with spine fractures/dislocations have injuries in more than one spinal region. This should be considered to be the minimum prevalence, as there may have been patients who despite having injuries found did not have the whole spine evaluated radiologically, and would therefore have had injuries in other regions of the spine missed.
We have also shown that although spinal injury occurs more commonly in the older child, when it does occur in younger children (aged 8 or less), it is associated with a higher prevalence of cord injury. In particular, the SCIWORA syndrome is primarily a disease of the young child. However, there is no clearly defined age at which the change from SCIWORA to bony injury occurs, and it would seem that these age cut-off points, although in keeping with developmental physiology, are artificial in clinical practice.
Data collection for the TARN database is performed at individual centres and relies heavily on accurate documentation. In several cases of cord injury, it was unclear whether there had been an associated fracture or dislocation. Where possible, this information was clarified after review of radiology reports, case notes, and postmortem examinations, but could not be found in 16 cases. Of those where clarification was possible, there were no cases of fracture or dislocation, implying that when bony injury occurred, this was recorded in the data collection, and therefore the true prevalence of SCIWORA may be higher than that found. Missing data for conscious level could not be easily retrieved, but separate analyses making assumptions on these patients having firstly a GCS of 15, and secondly a GCS of 14 or less (to produce a “worst case/best case” scenario), made no significant difference to the results.
Analysis of the relative risks associated with a decreased coma scale may be affected by the inclusion of children of an age where assessment is difficult. In total, 5215 (26.7%) patients were aged less than 5, at which age the standard GCS becomes less appropriate for young children. However, modified forms of the GCS have been produced and are used in the clinical setting. Moreover, we found that analysis only of children aged 5 or over revealed similar results (RR 0.87 (0.69 to 1.11; p = 0.25) for fracture/dislocation and RR 2.81 (1.68 to 4.69; p = 0.001) for cord injury).
The TARN database is not designed to record the stability of fractures, or the short or long term neurological outcome from cord injured patients, so it is not possible to draw conclusions as to the eventual disability suffered by these patients.
Spinal column injury is a relatively rare event in children, and therefore some of our patient numbers were small, leading to wide confidence intervals, particularly in the cord injury and SCIWORA group. As there were only 30 definite cases of SCIWORA, it was not felt appropriate to analyse them separately for risk factors as confidence intervals would be too large to draw meaningful conclusions.
Two reports from the National Pediatric Trauma Registry (NPTR) in the United States, give a prevalence of 1.6% and 1.5% of cervical spinal injury in the population of injured children.2,3 Our series is consistent with this analysis in some respects, in that 1.54% of all children with major trauma had a cervical spine injury, 1.26% having a cervical fracture/dislocation and/or cord injury. The prevalence of cervical cord injury in our group, however, was only 21.9% of all cervical spinal injuries compared with a level of 35% and 28.6% respectively in the analysis of the NPTR. One explanation for this difference may be due to data collection. The NPTR defines children as being aged less than 20, whereas our study group only includes those aged less than 16. Aetiological factors may also be important, with seatbelt legislation being stricter in the United Kingdom (61% of occupants in road traffic crashes were unrestrained in Patel and colleagues’ paper2), contact sports being less popular, and there being a total absence of penetrating injuries in our data.
In our series, the prevalence of cord injury is significantly higher in the younger than the older child. This is consistent with data from the National Pediatric Trauma Registry.2,3 We selected the age of 9 years as cut-off, as this best reflects the age at which the spinal column is thought to take on a more adult structure.1 However, in keeping with Kokoska and colleagues,3 we found no age at which there developed a change in the proportion of SCIWORA. Rather there was a gradual decline in prevalence as children became older.
In line with other analyses we have shown that road traffic crash is the most frequent mechanism of spinal column injury in children. In our group, this accounted for nearly half (49.8%) of all injuries, rising to 66.1% of cord injuries. This is similar to the overall frequency of RTC reported by Hadley et al, Osenbach and Menezes, Hamilton and Myles, and Mann and Dodds in specialist centres, encompassing all regions of the spine (39%, 50%, 52%, 46% of all injuries respectively).6,7,10,12 In our group, however, the frequency of sport injuries was reduced compared to most studies from the United States. This is likely to be due to the younger age definition for child (16 in our case) and possibly the lower take up of higher risk sporting activity.
In our study we have identified risk factors for the presence of different types of paediatric spinal column injury relating to associated injuries, overall injury severity, presenting conscious level, and mechanism of injury. This is the first time that this has been quantified from a trauma database. Previous reports have commented on the association of head injuries with cervical spine injuries, but have not shown how this may differ from the rest of the paediatric trauma population.
This study emphasises the factors that are associated with an increased risk of spinal injury—head injury for spinal cord injury, chest injury for SCI and spine fracture, high injury severity (ISS) for both. Although absence of these is associated with a lower risk, this does not imply that proper evaluation of the injured child’s spine need not take place. Rather, the groups identified should be seen as higher risk and therefore those in which particular care should be taken. In a retrospective audit of trauma transfers to a paediatric intensive care facility, Skellett et al found two of three patients with cervical spine fractures had no spinal immobilisation on arrival of the transfer team, and 28 of 58 at-risk patients had no immobilisation, of whom six were transferred this way.15 Particular care should be taken in assessing the spine of young children, and there should be a low threshold for further investigation. It is not within the context of this article to provide recommendations for which course these should take. Adult guidelines, such as those produced by the Eastern Association for the Surgery of Trauma,16 which do not recommend routine use of magnetic resonance imaging for obtunded patients, cannot necessarily be applied to children due to the high incidence of SCIWORA and the different radiographic appearance of paediatric and adult spines. However, studies using MRI are small, and their use needs to be further explored.
In our study group, 7.4% of children had a fracture of more than one spinal region. As has been discussed earlier, the true rate may be higher than this. We recommend that should a fracture be identified in a single region of the spine, radiological evaluation of the whole spine should be performed.
The TARN database does not differentiate between incomplete and complete lesions, and this study is not designed to follow children over a period of time, therefore outcome measures (other than death) cannot be assessed. Pattern of injuries and clinical experience differ from the United States, and therefore it can be assumed that outcomes may also vary. We believe that further studies need to be performed on the comparative roles of magnetic resonance imaging and computed tomography in paediatric spinal injuries, to allow evidence based guidelines to be produced. In these studies injury coding needs to become more sophisticated and a disability based outcome scale should be used.
At the time of writing, the National Institute of Clinical Excellence (NICE) is preparing guidelines for the evaluation of the cervical spine in trauma. It is likely that these are to be based primarily on data derived solely in adult patients, principally the Canadian C-Spine Rule.17 Due to the differences between the paediatric and the adult spine, caution should be used when assessing the risk of injury, even within guidelines such as these.
Conclusions
Although spinal injury in children is rare, it is associated with a high prevalence of cord injury, particularly in the younger age group (8 years and under). Risk factors for the presence of cord injury in the paediatric trauma population are RTC, presence of head, chest, or multiple injuries, and depressed level of consciousness. The prevalence of multilevel fractures (7.4% of all fractures) is sufficiently high to warrant whole spine radiography in the presence of a fracture. Clinicians from all specialties involved in the care of the injured child should be aware of these findings to reinforce the need for careful assessment in the management of those at highest risk of spinal injury.