Article Text

Abstract
Aims: To assess the clinical effectiveness of a paediatric hospital at home service compared to conventional hospital care.
Methods: A total of 399 children suffering from breathing difficulty (n = 202), diarrhoea and vomiting (n = 125), or fever (n = 72) were randomised to Hospital at Home or in-patient paediatric care. Main outcome measures were: comparative clinical effectiveness as measured by readmission rate within three months (used as a proxy for parental coping with illness); and length of stay/care and comparative satisfaction of both patients and carers.
Results: Clinical effectiveness of both services was not significantly different. Length of care was one day longer in the Hospital at Home group; however, most parents and children preferred home care.
Conclusions: Hospital at Home is a clinically acceptable form of care for these groups of acute paediatric illness. Readmission rates within three months failed to show any advantage in terms of parental coping. Parents and patients expressed a strong preference for hospital at home.
- clinical effectiveness
- hospital at home
- randomised controlled trial
- HAH, hospital at home
- HC, hospital care
- RCT, randomised controlled trial
Statistics from Altmetric.com
Increasing costs and an increase in patient demands have put considerable pressure on the National Health Service with the result that clinicians and health planners have been exploring alternative methods of managing patient care.1,2 A number of hospitals have begun to examine the concept of “Hospital at Home” (HAH) as an alternative to traditional hospital care (HC) for patients with non-life threatening illness. Most of the research carried out in this area has looked at the management of elderly patients or patients recovering from surgical operations.3–5 In these patients, a reduction in the length of hospital stay and the early return to home is seen as an advantage.
Traditionally, hospital care has been the only choice for acutely ill children requiring admission. There have been various attempts to develop alternative strategies for managing these patients with anecdotal benefit.6 Cuttell and Gartland described a paediatric home care renal nursing service, which showed improved satisfaction with an extended domiciliary nursing service.7 Dougherty et al reported improved health and social outcomes in a randomised controlled trial (RCT) comparing home care and HC for newly diagnosed diabetic children.8 Spinner et al showed significant cost savings by early home discharge from a neonatal unit.9 To our knowledge there have been no RCTs examining the outcomes of HAH and routine HC in acutely ill children.
We wished to set up a HAH scheme and were encouraged by one of our funding bodies (Wirral Health Authority) to do this by an evidence based evaluation. In this paper we describe an RCT comparing traditional HC with HAH for moderately ill children admitted to a district hospital with the following problems: breathing difficulties, diarrhoea with or without vomiting, or a feverish illness.
The objectives of the study were as follows:
To assess parental coping strategies during subsequent illnesses in their child as evidenced by the number of readmissions within 90 days of discharge
To determine the effects of HAH and routine HC on the length of stay for children with the three conditions
To assess qualitatively parental and patient satisfaction with the two types of care
To assess the cost effectiveness of both types of care.
SUBJECTS AND METHODS
Wirral NHS Trust is a large district general hospital in the north west of England with a 64 bedded paediatric unit, serving a population of 84 000 children.
HAH was set up as a nursing scheme operating 24 hours a day, seven days a week, providing planned visits until 23 00 hours and an on-call service during the night. The HAH nurses’ role was to support and care for children and their families, at the same time educating and empowering parents to care for their child. The children admitted to the scheme remained under the care of hospital consultants throughout. The number of nursing visits (1–4 visits daily) was determined by the patient’s condition. The HAH nurses planned the care and treatment of each child with the parents prior to them leaving hospital. This was reviewed and updated throughout the child’s illness according to change in condition, and in conjunction with the HAH treatment protocols. Discharge from the HAH scheme was decided by an HAH nurse, guided by agreed criteria (table 1). Nursing staff had access to medical advice and can arrange medical review if necessary. Families could contact an HAH nurse directly within 48 hours of discharge from the service, if the same symptoms recurred.
Criteria for discharging patients
The HAH team developed and piloted patient information booklets for each condition. These outline the possible course of the illness, signs and symptoms of potential deterioration, appropriate treatment, and contact information.
Any moderately ill patient with a feverish illness, diarrhoea with or without vomiting, or breathing difficulties, who fulfilled the agreed criteria was considered for the trial. The criteria for breathing difficulties were based on the British Thoracic Society guidelines for moderate asthma.10 The others were decided in-house and underwent pretrial piloting (table 2). The consensus among the consultant paediatricians at the beginning of the trial was that these patients required admission.
Criteria for trial entry
Patients fulfilling the criteria were accepted onto the trial after assessment by a doctor (registrar or consultant) and with the agreement of the HAH nurse (fig 1). The researcher, senior house officer, registrar, or consultant obtained consent from the patient’s parent(s), informed by written and taped explanations of the study.
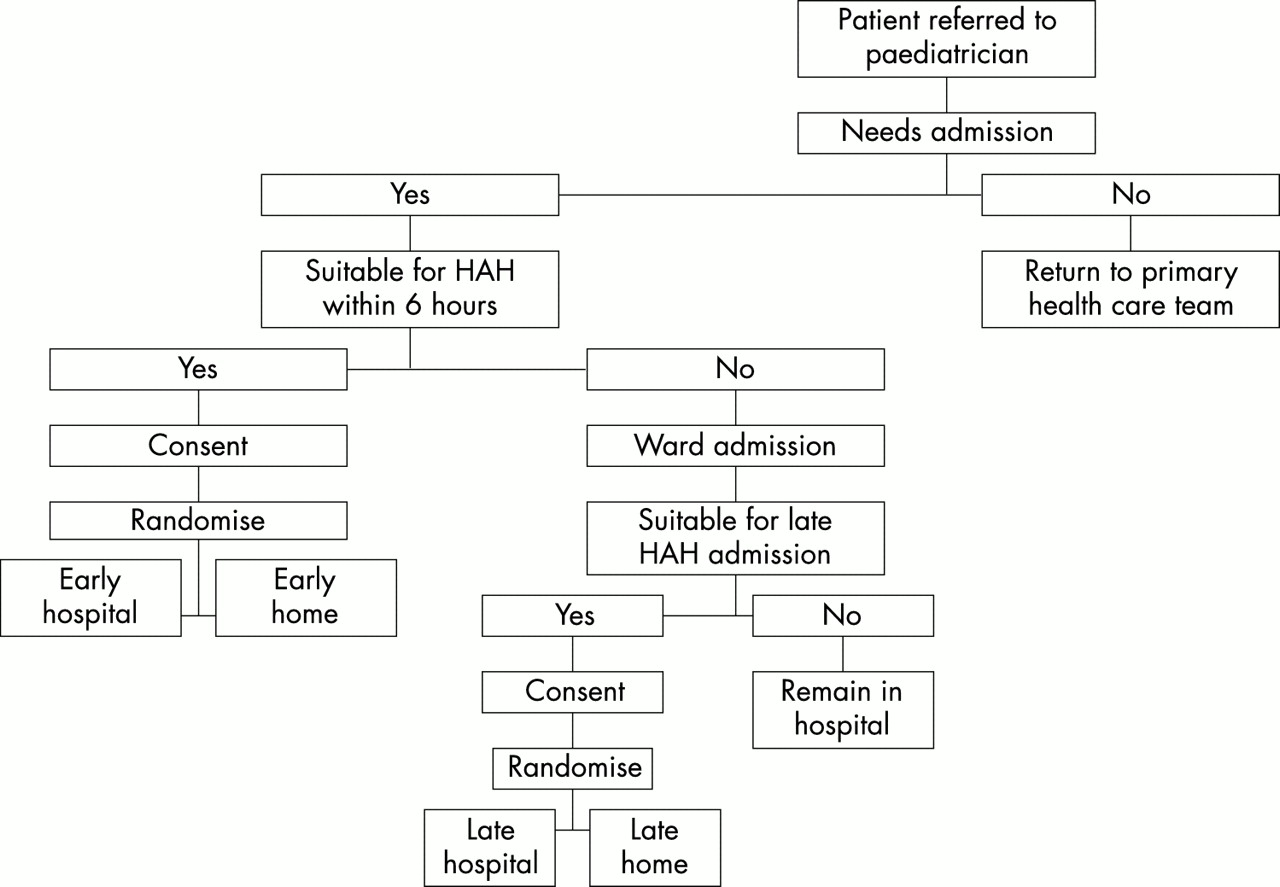
Assessment and randomisation process.
Patients were accepted between 09 00 and 22 00 hours, seven days a week, either at initial assessment (early group) or after review on the post-take ward round (late group). The early group was assessed within six hours of admission, and the late group included patients up to 24 hours after admission, providing they required at least a further 24 hours care.
Patients randomised to the HC group received standard hospital care relevant to their condition. Patients were randomised using a sealed numbered and opaque envelope technique. Ethical approval was obtained from the Wirral Health Authority Research Ethics Committee.
The sample size was calculated using reduction in readmissions as the primary outcome. Analysis of data from 1996/97 suggested that the readmission rate for children with these three problems was 17%. The study was designed to detect a relative reduction of 50% in this rate, requiring 195 patients in each group to detect such a change (80% power, 5% significance).
Secondary outcomes were included: A&E attendances within 90 days; length of stay/care and quality of care, assessed using patient and parental satisfaction interviews.
Data collection was conducted over 17 months (December 1998 to May 2000). This included sociodemographic details, information about the illness and its course, readmission within 90 days of discharge, and economic data. To avoid bias, an independent consultant paediatrician (DM) reviewed patient’s case notes and verified the diagnoses for all patients readmitted.
Analysis was conducted on an intention to treat basis. Significance testing was performed using the independent samples t test and non-parametric tests—Pearson’s χ2 test, Mann-Whitney U test, and Fisher’s exact test.
RESULTS
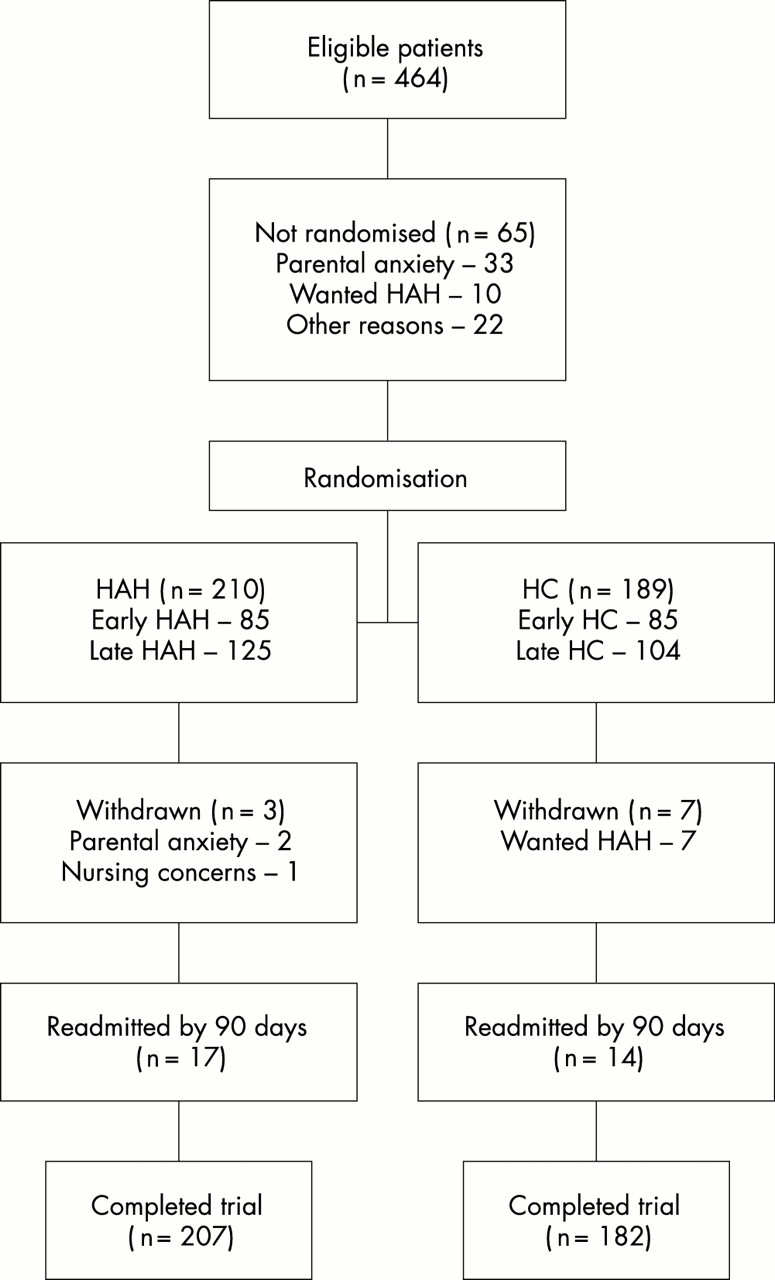
A total of 464 patients were invited to participate in the trial. Most refusals (40/60) occurred in the first six months of the trial. The main reason given was parental anxiety (n = 33), although 10 families refused randomisation because they wanted HAH rather than HC.
A total of 399 patients were randomised: 170 during initial assessment and 229 on the post-take ward round (fig 2). Analysis of sociodemographic data showed no significant differences between HC and HAH patients (table 3). The parental unemployment rates were high in both groups; Townsend deprivation scores were not significantly different (χ2 = 5.57; p = 0.13).
Sociodemographic characteristics of each group

{kind=link}
{kind=link}
Progress of patients through trial.
Patients had a median age of 13–15 months (range 6 weeks to 12 years). Overall, breathing difficulties formed the largest diagnostic group. Although more patients had breathing difficulties in the HC group (56% v 46%), these differences were not significant (p = 0.15; table 4).
Symptoms and length of stay/care by group
The mean length of care varied between HAH and HC patients: patients within the HAH group had an extra day of care compared to HC patients (p < 0.0001; table 4).
There were 36 readmissions within 90 days of discharge (table 5). The readmission rate for home care was not significantly higher than for hospital care (10.0% v 7.9%; p = 0.49). However, there was a significant difference in the reason for readmission: readmissions for breathing difficulties in the HAH arm occurred at twice the rate for hospital care, whereas readmissions for other conditions were less than half as frequent (p = 0.06; table 5). Thirty five trial patients (8.8%) presented at the A&E department during the 90 days following discharge, and no differences were detected by the study arm, or by initial diagnosis.
Emergency readmissions within 90 days (primary outcome)
A qualitative study compared a purposive sample of 40 families’ experiences of hospital and home care, using a face to face interview technique. The findings showed that 36/40 parents and 7/11 children stated a clear preference for HAH. Parents’ preference for HAH stemmed from their general perception that a child recovers more quickly in their own environment, without unnecessary isolation from other family members. The social disruption and financial cost of hospitalisation were identified as further reasons why parents preferred being at home. Parents were happy with home care provided that their child’s illness was not serious or life threatening and they had appropriate professional support. These findings are the subject of another paper.11
DISCUSSION
This study set out to see whether or not children presenting with three common childhood illnesses could be managed at home with similar outcome measures to traditional hospital care. The primary outcome measure for this study was readmissions as a measurable proxy for parental confidence in coping with a sick child. The results of the trial show some of the limitations of this measure.
The prestudy readmission rate was 17%; the overall hospital readmission rate during the data collection period was 17.5% with an improvement for trial patients to 8–10%. This may partly be attributed to the recognised non-specific effect of conducting any research tending to generate improvements in care.12,13 Within this study the strict admission criteria may have influenced the likelihood of readmission. In addition, the study population was predominantly acutely ill children, and readmission is more likely to occur with chronic illness. One child in the trial (HAH group) did have chronic lung disease and had four readmissions. Furthermore, since the majority of readmissions had different subsequent symptoms to those present on the initial admission, it is unlikely that parents would feel more equipped to care for their child at home.
Increased respiratory readmissions in the HAH group could reflect improved parental recognition of respiratory distress, resulting in more demand for treatment including admission in this group. It is certainly recognised in a primary care setting that parental education will increase demand for treatment in asthma.14 A further indication of this is that breathing difficulties accounted for 50% of overall admissions and 68% of readmissions. Known asthmatics accounted for 8% of initial admissions but 23% of the readmissions. Furthermore, these results may reflect the onset of chronic respiratory disease and asthma. By contrast acute febrile illness and gastroenteritis rarely develop into chronic conditions.
What do we already know?
-
Home nursing teams for children have been set up in many parts of the country with little evidence of their usefulness or cost effectiveness. These teams seldom manage acute illness
-
Most paediatric admissions are for self limiting conditions that need nursing observation
-
Factors that determine admission and readmission are commonly socioeconomic or related to health care delivery
What further information does this paper provide?
-
Acute illness in children with breathing difficulty, fever, or diarrhoea and vomiting can be managed with nursing observation at home when hospital admission would normally be considered necessary
-
Readmissions are at the same rate where initial care is at home or in hospital, but reduced in an RCT. Readmissions were increased for children with breathing difficulties but reduced for pyrexia and diarrhoea with or without vomiting
-
Most parents and children prefer home care
Nineteen per cent of readmissions occurred in the first week following discharge from care, most from the HC group (5 v 2). This is interesting as it may be that parents experiencing the HAH scheme do have some short term improvement in their coping skills.
The average length of stay in the HAH group was greater by approximately one day than in the HC group. However, HAH may be more appropriate and less costly than HC for these patients. Furthermore, HAH care encourages parents to agree a discharge date with the nurses, whereas in hospital it is largely a medical decision. Parents in their own home may find the additional visits beneficial and less stressful than being in hospital.
The large number of initial refusals may be attributed to parents and staff being relatively unfamiliar with the HAH concept. As staff became more knowledgeable about the service and research, fewer parents refused to take part. This may relate to improved information giving during the consent process.
Both groups in the study had low parental employment rates, confirming previous reports of higher paediatric admissions among socially deprived families,2,15 and suggesting that the HAH service is targeting inequalities in health.
This study included a small proportion of the service’s workload; limiting the conditions to control the research will have an impact on the cost and also determine the generalisability of the study. However, it is likely that there are a number of other conditions where protocols can be developed to manage patients within the home environment. This study has been seen locally as a success with expansion of the HAH service.
Most paediatric admissions are for self limiting conditions where HC consists primarily of nursing observations. This trial shows that HAH is an effective alternative for our defined conditions and that qualitative results show child and parent preference for HAH. This study therefore adds to the current evidence about the effectiveness of HAH services.
Acknowledgments
Funding was obtained from the North West Regional Office, Reactive Funding Scheme and Wirral Health Authority. We are grateful to Dr Donal Manning (consultant paediatrician) for validating the readmissions.