Article Text

Abstract
Background: The annual reported incidence rates for laboratory confirmed invasive pneumococcal disease (IPD) underestimate the true burden of invasive disease attributable to pneumococcal infection.
Aims: To estimate the proportion of “unspecified” mortality of infectious cause in infants and young children aged 1 month to 4 years reported by the Office for National Statistics (ONS) in England and Wales that could reasonably be attributed to IPD, thereby revising the total number of deaths per year potentially attributable to IPD, and producing a more accurate figure for the number of deaths that may be prevented by a programme of pneumococcal conjugate vaccination.
Methods: Polymerase chain reaction, latex agglutination, and other alternate methodologies to microbiological culture have been applied in various studies to the detection of Streptococcus pneumoniae. Some of these tests have been shown to be more sensitive indicators of pneumococcal infection. In our analysis the implications of these tests were applied theoretically to the “unspecified” clinical deaths caused by septicaemia, meningitis, and pneumonia reported by the ONS, with a 20% correction/reduction factor for nasopharyngeal carriage which these sensitive tests may coincidentally detect.
Results: The ONS reported an average of 13 deaths per year (1989–99) in infants and children aged 1 month to 4 years caused by pneumococcal septicaemia, meningitis, or pneumonia. By applying the rates for the more sensitive tests to the most recent ONS “unspecified” mortality data available (1999), the actual annual number of deaths caused by IPD in the age group 1 month to 4 years is shown to be at least as high as 43.
Conclusions: The mortality as a result of IPD in infants and young children may be at least three times the reported rate. The 7 valent pneumococcal conjugate vaccine may have the potential to prevent up to 26 (61%) of the IPD deaths per year in infants and young children in England and Wales alone.
- invasive pneumococcal disease
- pneumococcal conjugate vaccine
- pneumococcal meningitis
- pneumococcal septicaemia
- pneumococcal pneumonia
- mortality
- IPD, invasive pneumococcal disease
- ONS, Office for National Statistics
- PCR, polymerase chain reaction
- PCV, pneumococcal conjugate vaccine
Statistics from Altmetric.com
- invasive pneumococcal disease
- pneumococcal conjugate vaccine
- pneumococcal meningitis
- pneumococcal septicaemia
- pneumococcal pneumonia
- mortality
- IPD, invasive pneumococcal disease
- ONS, Office for National Statistics
- PCR, polymerase chain reaction
- PCV, pneumococcal conjugate vaccine
The annual reported incidence rates for laboratory confirmed invasive pneumococcal disease (IPD) in infants and young children underestimate the true burden of invasive disease attributable to pneumococcal infection in England and Wales. On average there were 12 laboratory confirmed deaths reported per year (1996–98) in infants and children 2 months to 4 years of age.1 This under reporting may be a result of several factors including prior antibiotic usage, blood, and CSF samples not being collected, and insensitivity of microbiological methods.
In contrast to laboratory reporting, the Office for National Statistics (ONS) collects clinical mortality reports for IPD from doctors which are published in tables according to the ICD-9 code.2 Alongside this mortality as a result of IPD, the ONS publishes data on deaths as a result of “unspecified” septicaemia, meningitis, and pneumonia. Had more sensitive diagnostic tests been used in these latter groups, a percentage could, in all likelihood, be attributed definitely to pneumococcal infection.
A 7 valent pneumococcal conjugate vaccine covering serotypes 4, 6B, 9V, 14, 18C, 19F, and 23F is licensed for use in European infants and children aged between 2 months and 2 years. Mortality as a result of pneumococcal septicaemia, meningitis, and pneumonia, the major clinical IPD syndromes, could be reduced with a programme of pneumococcal conjugate vaccination.3 A proportion of “unspecified” septicaemia, meningitis, and pneumonia will also be reduced by such a programme. For an under reported disease such as IPD, only the successful implementation of the vaccination programme will reveal, in retrospect, a realistic measure of disease burden prevented.
The aims of this study were to estimate the proportion of “unspecified” mortality in infants and young children 1 month to 4 years of age in England and Wales that could reasonably be attributed to IPD, thereby revising the total number of deaths per year potentially attributable to IPD, and to produce a more accurate figure for the number of deaths that may be prevented by a programme of pneumococcal conjugate vaccination.
METHODS
A number of studies in paediatric populations have ascertained the sensitivity and specificity of the polymerase chain reaction (PCR) of conserved regions, latex agglutination, pneumolysin immune complexes, pneumolysin antibodies, C polysaccharide antibodies, and combinations of the above for the detection of Streptococcus pneumoniae in the following conditions:
In only one of these studies did pneumolysin immune complexes contribute towards the diagnosis in a small number of cases,5 PCR being the mainstay in all six studies. The authors of these studies applied these tests to subjects with culture negative unspecified septicaemia, meningitis, or pneumonia, thereby estimating the proportion which may be a result of pneumococcal infection (table 1⇓):
Summary of sensitivity and specificity of PCR, latex agglutination, and other tests in the detection of pneumococcal septicaemia, meningitis, and pneumonia, and the application of these tests to “unspecified” septicaemia, meningitis, and pneumonia in the cited studies
In our analysis, in order to be conservative, the lower rates (16% and 36% respectively) were applied to the “unspecified” deaths caused by septicaemia (ICD-9 code 038.9) and pneumonia (ICD-9 codes 485, 486), and the 45% rate was applied to the “unspecified” deaths caused by meningitis (ICD-9 codes 320.9, 322.9), in infants and children aged 1 month to 4 years as reported by the ONS.2 This rate was derived from a study in India, so may not be applicable in the UK.7 The pneumonia rate is consistent with the 33% rate found for abnormal chest radiograph in the “vaccine probe” Northern California Kaiser Permanente efficacy trial of the 7 valent pneumococcal conjugate vaccine (PCV).9 Studies have shown a PCR positivity rate for well children of 16–17%,6,8 probably caused by nasopharyngeal carriage of Streptococcus pneumoniae. Because coincidental nasopharyngeal pneumococcal carriage may be detected by the tests in subjects who died of causes unrelated to pneumococcal infection, a conservative correction/reduction factor for nasopharyngeal carriage of 20% was applied in order to account for this.
We then calculated the preventable proportion of the 1999 deaths, the year for which the most recent ONS “unspecified” mortality data are available, on the basis of a serotype coverage of 76% for the age group 6 months to 4 years,1 an efficacy of 97.4%,3 a vaccine uptake of 93%, and a subtraction of an estimated four deaths for those in the age group 1 to 4 months not fully vaccinated (Dr E Miller, PHLS, personal communication).
RESULTS
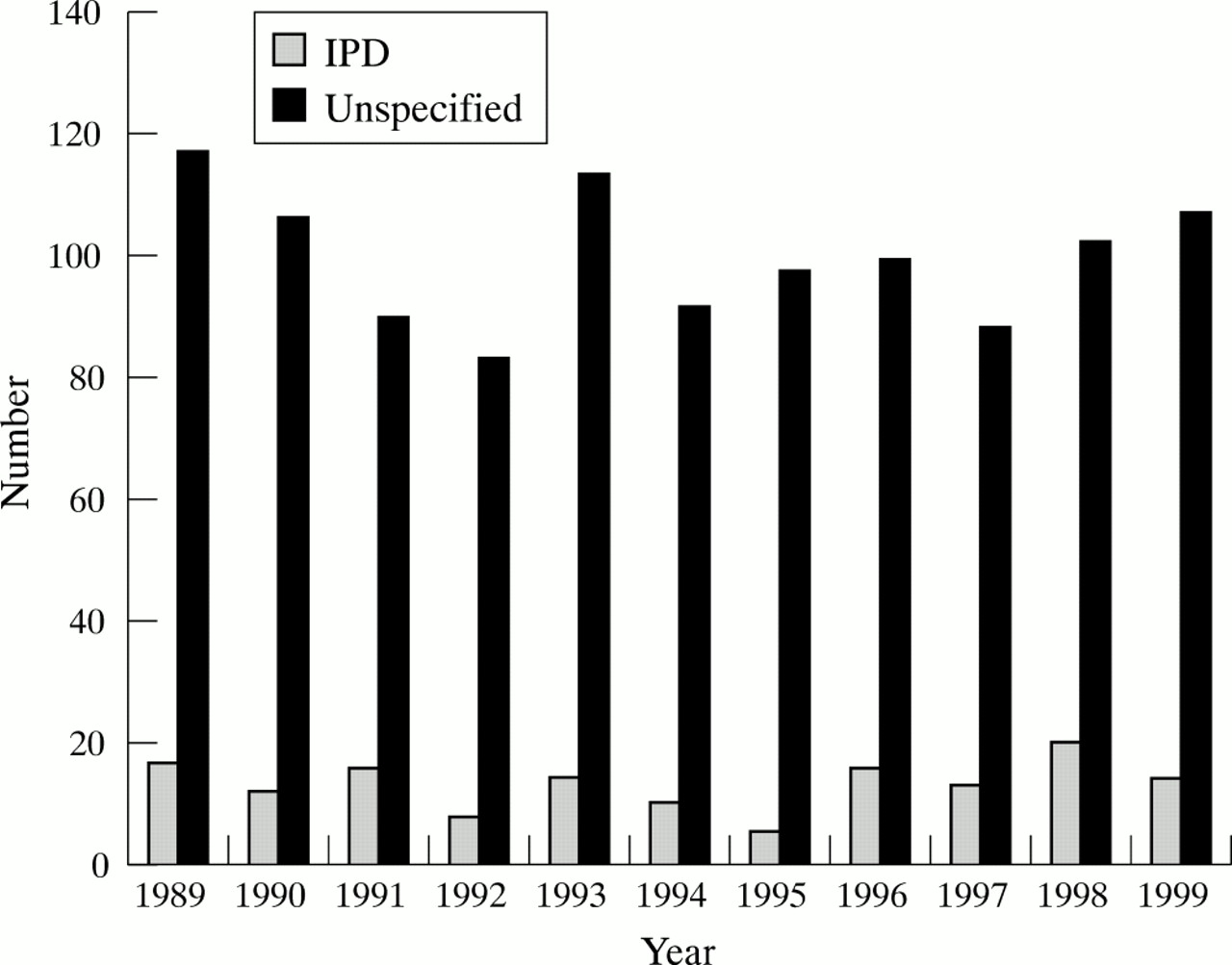
There were 14 IPD deaths (three septicaemia, eight meningitis, three pneumonia) in the age group 1 month to 4 years reported to the ONS for the year 1999; this is consistent with the average number of deaths per year of 13 for 1989–99 as shown in table 2⇓ and fig 1⇓ (Glenn Meredith, Office for National Statistics, Mortality Statistics Section, personal communication). In addition there were a total of 107 deaths caused by “unspecified” septicaemia (n = 17), meningitis (n = 13), and pneumonia (n = 77) in 1999. Table 3⇓ shows the underlying conditions present in the 14 IPD deaths and in 102 of the 107 “unspecified” deaths for which information was available (Glenn Meredith, ONS, Mortality Statistics Section, personal communication). In one of the 14 IPD deaths there was an underlying condition; in 45 of the 102 “unspecified” deaths was such a condition present. Our study cannot specify what proportion of those with or without underlying conditions is preventable with vaccination. Figure 1⇓ shows that the longer term trend for the annual “unspecified” deaths has fluctuated around 100 per year. The five years during the period 1989 to 1999 when the lowest number of IPD deaths occurred correspond to four of the five years in which the lowest number of “unspecified” deaths occurred.
ONS 1989–99 England and Wales reported deaths due to IPD in the age group 1 month to 4 years
Underlying conditions in deaths in 1999, age group 1 month to 4 years (ONS)

IPD and unspecified meningitis, septicaemia, and pneumonia deaths, 1989–99, in England and Wales reported to ONS.
For the 17 cases of “unspecified” septicaemia, 16% were potentially caused by pneumococcal infection, giving an additional three deaths; for the 13 cases of “unspecified” meningitis, 45% were potentially caused by pneumococcal infection, giving an additional six deaths; and for the 77 cases of “unspecified” pneumonia, 36% were potentially caused by pneumococcal infection, giving an additional 27 deaths. Applying the correction factor of 20% for coincidental nasopharyngeal carriage, these numbers are reduced to two, five, and 22 respectively, giving a total of 29 extra deaths potentially caused by IPD.
Adding this number to the 14 deaths reported as being caused by IPD, there were thus 43 deaths in 1999 in this age group for which Streptococcus pneumoniae could reasonably be given as the cause. The 7 valent PCV is reported to provide a serotype coverage of 76% for IPD in England and Wales for the age group 6 months to 4 years.1 With 97.4% efficacy,3 93% uptake, and subtracting an estimated four deaths in the age group 1–4 months (those not fully vaccinated), this would represent 26 (61%) preventable deaths per year in the age group 5 months to 4 years in the event of a 7 valent pneumococcal conjugate infant vaccination programme. Limiting the same calculation process to the age group 5–11 months, one obtains 26 deaths, of which 14 (54%) would be preventable with an infant vaccination programme.
DISCUSSION
Vaccination programmes targeted at Haemophilus influenzae type b (Hib) (fig 2⇓) and Neisseria meningitidis group C have resulted in substantial reductions in mortality in vaccinees. Further reduction in infant and child mortality is an achievable public health aim. The full extent of such a reduction and the inherent cost–benefit ratio can be predicted when the true burden of disease is calculated. Although the methodology described herein could be applied to the considerable morbidity attributable to IPD, it is the application to mortality that this analysis addresses.

{kind=link}
{kind=link}
H influenzae deaths, 1979–99, in England and Wales reported to ONS.
Our calculation estimates the annual death rate from IPD to be 43 infants and children in the age group 1 month up to and including 4 years, which is around three times the rate published for laboratory confirmed cases or clinical reports. This may be a conservative estimate based on the application of alternate tests, mainly PCR, which may be more specific and sensitive than culture, to clinical syndromes potentially caused by pneumococcal infection, combined with actual clinical reports for pneumococcal mortality. Although the actual mortality may be higher than 43 per year it is possible that it is lower and closer to the ONS rate of 13 per year; the true mortality savings should be revealed by the application of a pneumococcal immunisation programme which would include those under the age of 2 years. A US study based on the Active Bacterial Core surveillance and the National Vital Statistics System for the period 1996–98 concluded that IPD deaths in all age groups may be underestimated by 15–45%.10 Enhanced surveillance proved an effective means for estimating the true burden of Hib disease in the UK between 1985 and 1991.11
The proportion of “unspecified” disease (septicaemia, meningitis, and pneumonia) attributable to pneumococcal infection was calculated using paediatric studies from various countries: USA,4,6 India,7 Israel,8 and Finland.5 Such studies have not been performed in the UK. Perhaps the greatest generalisation we have made is in applying Indian data to the UK. However, even if the estimate of 45% for “unspecified” meningitis is substantially reduced to 20%, the estimated number of “unspecified” deaths would be little affected: 26 instead of 29. Most of the “unspecified” deaths are attributable to pneumococcal pneumonia, for which we have more robust data in the form of the large Northern California Kaiser Permanente study,9 where 33% of “abnormal chest radiograph” pneumonia was prevented by the 7 valent pneumococcal conjugate vaccine.
While 44% of the “unspecified” deaths were associated with an underlying condition as shown in table 3⇑, the majority did not have such a condition identified. Nevertheless, had more extensive microbiological investigations been possible, a definitive cause may have been found, although empiric antibiotic treatment may have rendered such investigations negative. Because of the theoretical nature of our study we do not specifiy which of the deaths were preventable, only that a proportion is preventable.
The Department of Health National Health Inequalities Targets12 stated that there were 109 deaths as a result of infection in the year 1999 in infants 1 month to 1 year of age. If 14 of these deaths are caused by IPD, as estimated by the present study, a 13% reduction in infant deaths caused by infection could be achieved by means of a robust pneumococcal conjugate infant vaccination programme.
In conclusion, the total number of deaths per year caused by IPD in infants and young children 1 month to 4 years of age in England and Wales is estimated to be 43. The number of deaths each year that may be prevented by a programme of 7 valent pneumococcal conjugate infant vaccination may be as high as 14 for the age group 5–11 months and 26 for the age group 5 months to 4 years. The vaccine has the potential to contribute towards additional mortality savings that will only become evident after its introduction.
Footnotes
Competing interest: The first author is employed by Wyeth, which owns and markets 7 valent pneumococcal conjugate vaccine. The second author is a paid consultant to Wyeth.