Article Text

Abstract
Aim: To find an effective symptomatic treatment for osteogenesis imperfecta (OI).
Methods: In a prospective observational study disodium pamidronate (APD) was given as monthly intravenous infusions to 28 children and adolescents (aged 0.6–18 years) with severe OI or a milder form of the disease, but with spinal compression fractures.
Results: During treatment for 2–9 years, dual energy x ray absorptiometry measurements of the total body and of the lumbar spine showed a gradual increase in bone density. All bone metabolism variables in serum (alkaline phosphatase, osteocalcin, procollagen 1 C-terminal peptide, collagen 1 teleopeptide) and urine (deoxypyridinoline) indicated that there was a decrease in bone turnover. All patients experienced beneficial effects and the younger patients reported a major improvement in wellbeing, pain, and mobility without significant side effects. Vertebral remodelling was also seen.
Conclusions: APD seems to be an efficient symptomatic treatment for children and adolescents with OI.
- bisphosphonate
- osteogenesis imperfecta
- ALP, alkaline phosphatase
- APD, disodium pamidronate
- 1CTP, collagen 1 teleopeptide
- DXA, dual energy x ray absorptiometry
- OI, osteogenesis imperfecta
- P1CP, procollagen 1 C-terminal peptide
Statistics from Altmetric.com
- ALP, alkaline phosphatase
- APD, disodium pamidronate
- 1CTP, collagen 1 teleopeptide
- DXA, dual energy x ray absorptiometry
- OI, osteogenesis imperfecta
- P1CP, procollagen 1 C-terminal peptide
Osteogenesis imperfecta (OI) is a congenital disease of collagen with variable phenotype. In milder forms the fracture rate is only slightly increased and the stature is normal or slightly decreased. In severe forms, bone softness and multiple fractures lead to progressive bone deformities with extreme shortness, frequent skeletal pain, and confinement to a wheelchair. In most cases, there are mutations in the COLIA1 or COLIA2 genes localised to chromosomes 17 and 7, respectively. This leads either to a reduced production of normal collagen type I, or to the synthesis of abnormal collagen type I. The current classification into four major subgroups (types I–IV), based on clinical findings, was proposed by Sillence et al in 1979.1,2
Some relation between genotype and phenotype has been reported,3,4 but in general the genotype is an unreliable predictor of phenotype and severity.
Many types of pharmacological treatment have been tried for the severe forms of OI. Sodium fluoride has been tried without any convincing benefit.5 Growth hormone shows a beneficial effect, mostly in milder forms of OI.6 Calcitonin was, at the start of our study available only as an injectable preparation. It had beneficial effects but pronounced side effects.7,8
The bisphosphonates are stable analogues of pyrophosphate, have a long half life when incorporated into bone, and have multiple effects, predominantly inhibition of osteoclast activity.9–11 Bisphosphonates have been used extensively for treatment of hypercalcaemia and pain in osteolytic bone metastases, and in osteoporosis.12,13 They have also been used to treat children with juvenile idiopathic osteoporosis and Gaucher's disease.14 After two promising case reports of oral treatment by Devogelaer and colleagues15 and Huaux and Lokietek16 in 1987 and 1988, we chose to initiate treatment with intravenous disodium pamidronate (APD). The rationale for bisphosphonate treatment in OI is that the complex function of bisphosphonate, with a predominantly inhibitory effect on osteoclasts, might lead to a net effect of increased bone mass in OI patients.9–11 The beneficial effect on our first patient was dramatic and was reported at the Fifth International Conference on OI in 1993. Since then the study has expanded and similar studies have been started elsewhere. Glorieux et al have described the treatment of 30 children, but with a shorter observation time.17 We have previously published very promising long term results in three adolescents with severe OI.18 We now confirm benefit in 28 carefully monitored patients, in whom treatment was started before or in the early teens.
PATIENTS AND METHODS
Patients
A total of 92 patients have been referred to our centre for assessment; 45% fulfilled the criteria for treatment. Between September 1991 and February 2001 APD was administered for at least two years to 28 patients under 18 years of age with either severe OI (including short stature, skeletal deformities, and pain) or with a milder form of the disease but with compression fractures of the spine. All children and adolescents fulfilling these criteria were offered and accepted treatment. Treatment was not offered to patients with mild OI without compression fractures of the spine, or who were aged over 20 years. Ten of the patients had severe OI (type III) with extreme shortness and skeletal deformities. Thirteen had a moderate form of the disease (12 with type IV and one with type I) with some deformities and moderate growth retardation, and five had a milder form (type I) with only slightly affected growth but with vertebral compression (table 1). The age range at the start of treatment was 0.6–18 years (mean 9.2, median 9.9 years). The study was approved by the local ethics committee and by the Swedish Medical Products Agency. The treatment was given after informed consent and could be discontinued by the patients or parents at any time.
Clinical features and change in wellbeing, pain, analgesic intake, and mobility before and during APD treatment
Treatment
The patients were treated with monthly infusions of 10–40 mg/m2 APD, over 5–8 hours, preceded by hydration with buffered glucose 25 mg/ml (total dose 500 ml/m2 for 2–4 hours). The treatment protocol was maintained for 2–9 years. The intravenous route was chosen mainly to prevent differences in bioavailability from interfering with the interpretation of results. Seven of the children, one of whom also has mild von Willebrand disease, had an intravenous port (port-a-cath) without any vascular or infectious complications.
The dose chosen was based on experience from treatment of hypercalcaemia and osteolytic bone metastases in children. For the first three months a dose of 10 mg/m2 was given, over the next three months 20 mg/m2, followed by 30 mg/m2 for further treatment. After 1–2 years, five of the younger children reported recurrence of some skeletal pain and less wellbeing during the last week before the next dose was due. An increase to 40 mg/m2 made these symptoms disappear for up to two years of further treatment. Four adolescents have received a dose of 30 mg/m2 for 4–9 years without any such symptoms or need for dose change. The duration of treatment has been at least two years, and for 14 of the patients, three years or more (median 2.8 years; table 1).
To compensate for a generalised decrease in serum calcium, 18/28 patients were also given oral treatment with 1,25-dihydroxycholecalciferol. The dose varied individually from 0.08 μg/m2 every second day during the first week after the infusion, to 1.0 μg/m2 daily during week 1 and then 0.5 μg/m2 daily or every second day for the rest of the month. We imposed no dietary restrictions but made sure that milk products were not avoided. Five of the adolescents changed after 2–6 years of APD treatment to oral sodium alendronate, in a standard daily dose of 10 mg (0.2–0.3 mg/kg), with continuing benefit. The rationale for changing to oral treatment was that they had responded well to intravenous treatment and were old enough to swallow tablets, thereby freeing them from monthly intravenous infusions and hospital contacts. After 18 months one of these patients chose to return to intravenous APD because of gastrointestinal side effects.
Methods
Bone turnover was assayed every sixth months for two years, then annually, by determining serum osteocalcin, alkaline phosphatase (ALP), procollagen 1 C-terminal peptide (P1CP), collagen 1 teleopeptide (1CTP), calcium, and phosphate. Urinary calcium/creatinine quotient and deoxypyridinoline were analysed. Because of known diurnal variation the samples were, with very few exceptions, taken between 9 and 11 am. As the normal reference values for many methods differ considerably between small children and adolescents and our patient group was heterogeneous, we chose only to compare changes in the medians for the whole group during treatment and not give ranges.
Blood chemistry: Na, K, Mg, alanine aminotransferase (ALT), aspartate aminotransferase (AST), albumin, creatinine, and parathyroid hormone, as well as white blood cells (WBC), platelets, and haemoglobin were determined 3–6 months before the start of treatment, then every six months during the first two years, then annually. Concentrations of calcium and phosphate were also measured at the time of each treatment, both before and after the APD infusion. Ca and phosphate concentrations were measured after three and seven days until stabilisation of serum Ca was achieved. ALP was determined by IRMA (immunoradiometric assay); P1CP and 1CTP were determined by RIA (radioimmunoassay). The total coefficients of variation were 6.3% and 5.4% for serum P1CP concentration of 111 μg/l. The interassay coefficients of variation were 6.3% and 2.2% for mean serum 1CTP concentrations of 8.3 and 20.7 μg/l respectively; intra-assay coefficients of variation were 6.3% and 6.2%, respectively. Osteocalcin was determined by IRMA. The interassay coefficients of variation were 5.2% and 4.5% for mean serum osteocalcin concentrations of 21.9 and 183.9 μg/l respectively; intr-aassay coefficients of variation were 3.8% and 3.9%, respectively. Deoxypyridinolines were measured by EIA (enzyme immunoassay). The total coefficients of variation were 11% and 7.4% for mean urine deoxypyridinoline concentrations of 13.5 and 98 nmol/l. All other tests were performed by standard techniques.
Bone density was assessed every six months during the first two years and then annually, by dual energy x ray absorptiometry (DXA)19,20 measurements of the total body and spine (L1–L4) using the lunar DPX system. The paediatric software for Lunar DPX-L was used, with scan models large (CV% 0.09), medium (CV% 0.28), and small (CV% 0.28). If the patient's weight/height quotient was over 0.72 a slower scan mode was used. The laboratory obtained the new and more rapid Hologic QDR 4500 system after several years of the study. Because of shorter immobilisation time it was first used on the smaller children. During the first period in use determinations were made in parallel with both types of equipment. The observed differences between the obtained duplicates were within the variation of the respective method.
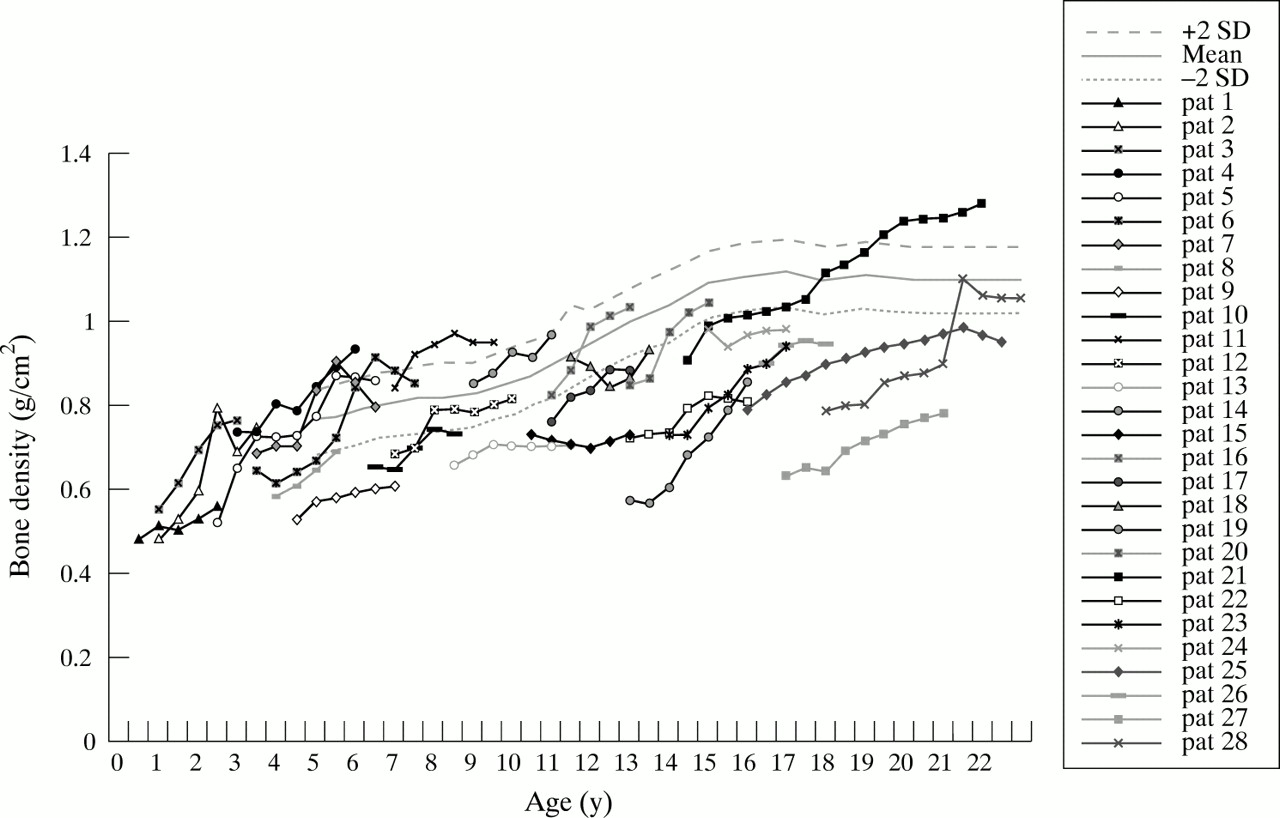
DXA provides a measure of areal bone mineral density (aBMD, mg/cm2) that is calculated by dividing the bone mineral content by the projected bone area of the region of skeleton scanned. As the depth and therefore the volume of the scanned bone is not measured, aBMD fails to distinguish between changes in the mineral density and bone size in growing children. Thus, interpretation of DXA measured aBMD in severe OI (type III), a condition characterised by small and often deformed bones, is problematic. We adopted a pragmatic approach by displaying DXA data graphically against normative mean, 5th, and 95th confidence interval curves (figs 1 and 2, lunar paediatric normative data used).

Bone density (DXA, L1–L4) in g/cm2 during APD treatment. Data for individual patients are plotted against lunar mean, 5th, and 95th confidence interval curves for healthy children
Bone density (DXA, total body) in g/cm2 during APD treatment. Data for individual patients are plotted against lunar mean, 5th, and 95th confidence interval curves for healthy children
The number and extent of compression fractures of the spine, as well as vertebral height, were assessed by conventional x ray, in frontal and side projection. Assessments were done before the start of treatment and after two (and for those with longer treatment time also after three, four, six, and nine) years of treatment.
Bone age was determined according to the method of Greulich and Pyle before and after two years of treatment.21
Ultrasound examination for possible microcalcifications of the kidneys was carried out after one, three, and six years of treatment; in our only case of microcalcifications this was followed up every six months.
Wellbeing, based on parents' and patients' subjective assessment, was initially assessed 3–6 months before treatment. Patients or parents registered wellbeing in special diaries using an arbitrary 10 grade scale, where 10 represents maximal wellbeing; they could choose any number between 1 and 10. As pain is difficult to assess, especially in small children, we chose only to ask patients or parents to record how many days per month that the children experienced pain, and not to record the intensity of pain.
Ambulation was assessed using the Wilson scale of nine levels: (1) functional walking without aid in all surroundings; (2) functional walking without aid in secluded surroundings; (3) functional walking with crutches in all surroundings; (4) walking with crutches in secluded surroundings; (5) functional walking with key walker in all surroundings; (6) walking with key walker in secluded surroundings; (7) reciprocal crawling with arms and legs; (8) any other form of locomotion; (9) sitting with support and no mobility. This scale, which best shows changes in mobility in non-walkers, includes two grades of non-walking locomotion, including crawling and bottom shuffling (any other form), which are important for functional needs and independent living in the severe form of OI. The scale, which is used in clinical practice in parts of Sweden, was devised by the physiotherapist Janet Wilson of St Louis (Illinois, USA). As this scale is unpublished we also used the five degree scale according to the criteria of Bleck, to facilitate comparison with other studies. Bleck divided ambulation into: (1) non-walker; (2) not functional, physiotherapy walker; (2) household walker; (3) outside but only neighbourhood walker; (4) community walker.22
Stature was measured, in the supine position, every six months and growth rate was compared with pretreatment values.
Statistical analysis
Wilcoxon matched pairs signed ranks tests were used to evaluate the difference between pretreatment levels and levels after two years of treatment for DXA, ALP, osteocalcin, P1CP, 1CTP, and deoxypyridinoline as well as changes in mobility, wellbeing, pain, and the use of analgesics. The tests were two tailed and p < 0.05 was chosen to indicate significant deviation from the null hypothesis. As the results were not normally distributed medians were generally used; however, in the tables we showed both medians and means to facilitate comparison with other studies.
RESULTS
Biochemical changes
Before treatment all but one patient had normal values of serum WBC, platelets, and haemoglobin as well as Ca, PO4, Na, K, Mg, ALT, AST, albumin, creatinine, and parathyroid hormone. One girl, 1.1 years of age, had slightly raised Ca of 2.62–2.72 mmol/l (normal 2.20–2.60). In the days following the pamidronate infusion, serum Ca fell in 18/28 patients, usually to values below the normal limit, with the lowest value at 24–48 hours. The decrease normalised within seven days. Additional daily treatment with 1,25-dihydroxycholecalciferol was given orally to these patients to stabilise serum calcium. For 10/28 patients this supplement was not needed. No difference in the therapeutic effect of treatment (assessed by biochemical markers, DXA, recordings of wellbeing and pain, ambulatory change, and growth rate) was seen between the supplemented and unsupplemented groups (results not shown).
Serum alkaline phosphatase (ALP, p < 0.001), osteocalcin (p < 0.001), P1CP (p < 0.001), 1CTP (p = 0.012), and urine deoxypyridinoline (p < 0.001) all significantly decreased over time, indicating a reduction of bone turnover (table 2). No abnormal values or changes over time were observed for serum WBC, platelets, haemoglobin, Na, K, PO4, Mg, ALT, AST, albumin, creatinine, parathyroid hormone, or urine calcium/creatinine quotient.
Serum ALP, osteocalcin, P1CP, 1CTP, and urine deoxypyridinoline (DPD) before and during APD treatment
Bone density
Before treatment 26 of the 28 patients had low lumbar bone density, compared to normal adult and age matched controls.20,23 The two patients with normal values had the mild form of the disease but with vertebral compression fractures. Most of the patients also had low total body bone density values (figs 1 and 2). During the course of treatment a gradual increase in bone density was observed in all individuals, both from DXA measurements of total body and in the lumbar spine (figs 1 and 2). There was a significant increase in median total body values of 0.106 g/cm2 (p < 0.001) and median lumbar values of 0.248 g/cm2 (p < 0.001) during two years of treatment. This increase brought them closer to the age matched values after two years compared with the pretreatment values. Lumbar values were initially disproportionately low and increased more rapidly than the total body values (figs 1 and 2). In seven of the patients who were investigated at an early age, one or two lumbar spine values were missing. In order to obtain comparable data in the graphs, these missing registrations were calculated from the total spine values in the whole body scans, using each child's own quotient from the recordings where both values were available.
Radiological findings
In younger children with the mild or moderate form of the disease we were able to observe signs of new bone formation with increased vertebral height after two years of treatment, with increased vertebral height compared to vertebral width (fig 3). In the more severe forms and in the prepubertal age group this improvement was usually observed by conventional x ray after three years. In adolescents however, by comparing vertebral height on the radiograms, we could observe slower or no further progress of the vertebral compressions but no bone regeneration after 2–9 years of treatment. Our study is too small to determine the upper age limit (and maturity of the bone) for a chance of vertebral regeneration. This age limit might vary between the types. In OI type I there was substantial regression of vertebral compressions in younger children, and even a slight regression in a 13.3 year old girl. In a 7 year old girl and in three younger children with OI type III, we could see increased vertebral height after 2–3 years, but in an 11.7 year old girl and five older children with type III, there was no increase after 2–9 years. In OI type IV vertebral regeneration occurred in children up to the age of 10.8 years at start of treatment.

{kind=link}
{kind=link}
{kind=link}
Radiographs (lateral view) of the lumbar spine of an 1.1 year old girl with osteogenesis imperfecta type IV (patient 2). (A) Before start of treatment. (B) After two years treatment. A considerable increase of mineralisation and vertebral height can be seen, with almost complete regeneration of the vertebral height around L1
Bone age measured before and after two years of treatment followed the chronological changes in bone maturity, with median values of ±0 SD, and was not affected by the treatment.
Clinical changes
During the initial 3–6 month pretreatment period no significant change was identified in pain, wellbeing, analgesic intake, or mobility. All patients' subjective scores for wellbeing, pain, and activities of daily life improved greatly during treatment; these were sustained during 2–9 years follow up (table 1). A dramatic and progressive decrease in pain and improved wellbeing was reported within 2–10 weeks of onset of treatment. The median rating for wellbeing improved by 3.5 units, from 4.5 to 8.0 units after two years (p < 0.001). The most recent recording shows an additional small improvement to 8.5 units (table 1). Twenty one children became pain free during treatment. Two reported a substantial decrease in pain and were pain free most days. Three of the older patients reported pain every day, but with decreased intensity, and were able to discontinue their intake of analgesics (table 1). Two of the youngest patients (aged 0.6 and 1.2 years) are excluded from this analysis because their parents found it hard to estimate the pain their children experienced before treatment (table 1).
The pretreatment median value for pain was 30 days per month. After two years there was a decrease of 30 days to 0 days/month (p < 0.001) and on the most recent recording (after 2–9 years of treatment) this improvement remains. Before treatment 16/28 patients needed analgesics. They decreased their intake of analgesics by between two and 30 days per month (mean eight days). At time of writing, no patient is in need of analgesics, except in case of fracture.
Using the nine degree scale, ambulation improved in 21/28 patients from a mean of 8.0 to 6.0 units after two years. The most recent recordings showed an additional improvement in three children but an unchanged median value of 6.0 (table 1). In the whole group there is a significant improvement of 2.0 units from 8.0 to 6.0 after two years (p < 0.001). It is important to note that values of 6 and lower represent the ability to walk. During treatment 13/22 non-walkers have achieved walking ability, with a median increase of ambulation of 2.0 units. Their median age at the start of treatment was 6.4 years (range 1.1–17.3, mean 8.1 years). No patient deteriorated in their ambulatory function during treatment (table 1). When using the five degree scale, ambulation improved in 15/28 patients from a median value of 0.0 to 2.0 units, both after two years and at the latest recording. There was no change in ambulation of the other 13/28 patients (table 1). In the whole group there was a significant improvement of 1.5 units from 0.0 to 1.0 after two years (p < 0.001). Here 1 represents walking during physiotherapy and 2 or more corresponds to independent walking with or without walking aids. One 16 year old girl with severe OI and a height of 105 cm at the start of treatment improved from no ambulation to walking with aids in sheltered surroundings. Two adolescents with severe OI were still bound to their electric wheelchair during treatment. One child walking freely in secluded surroundings and one walking with crutches did not change their ambulation level. Two children had functional walking in all situations before onset of treatment.
Clinical examples
A boy with type IV OI, was aged 7 months at the start of treatment. He was lying supine with curved lower extremities and compression fractures of the spine. After two years of treatment he was crawling and standing with support and the pre-existing gibbus had resolved.
A girl with type IV OI and severe compression fractures of the spine and curved legs could only lie supine prior to treatment at 1.1 years of age. After 2.5 years of treatment (combined with intramedullary rodding of femora and tibiae after one year of treatment) she is walking without aids; x ray of the spine shows substantial remodelling of vertebral compression fractures and normalisation of the height of several vertebral bodies (fig 3).
A boy with type III OI, who at 3 years of age could not sit without support, was able to walk with a key walker after three years of treatment.
Growth had ceased in four adolescents before starting treatment. For five others we do not have height velocity values for the year preceding start of treatment. For the remainder, the median value of growth was 4.7 cm for the year before treatment; during their first and second treatment years median values were 6.5 and 4.4 cm/year respectively (mean values 4.3, 5.8, and 5.2). The rate of increase in height in the adolescent group was not less than that of younger children.
Side effects
No adverse effects were seen, with the exception of a short episode of fever occurring over an 8–16 hour period starting 6–8 hours after the first APD infusion in five of the 28 patients, despite prior hydration. Four patients also had an episode of fever after increasing the dose. Only two of these patients experienced muscular pain during this time. None had symptoms of fever or muscle pain after subsequent treatments. One girl, aged 1.1 years, had a slightly increased serum calcium concentration at the start of the treatment, which was sustained; after one year she had microcalcifications of the renal papillae. In Sweden a diet complement of A and D vitamins is generally recommended. This complement was withdrawn, resulting in normalisation of serum calcium; the microcalcifications are regressing. Parathyroid hormone concentrations were normal during this time.
No adverse effects on fracture healing were seen.
DISCUSSION
There are good theoretical reasons for believing that the bisphosphonates could be valuable for symptomatic treatment of OI. After our first report on intravenous treatment in 1993, similar studies have reported beneficial effects.17,24–29 A long term study on the effects of oral bisphosphonates also showed positive results.30 The low incidence and heterogeneity of the disease makes the performance of randomised studies difficult. We now report the beneficial long term (up to nine years) effects of intravenous treatment without significant adverse effects. The overall positive results and absence of adverse effects may be sufficient to recommend the use of this treatment for all children with OI who have the more severe form, and for milder forms with compression of the spine. Despite the limited data on long term follow up, it may be argued that it is unethical not to treat children with OI, especially those with compression of the spine before puberty. While waiting without treatment these prepubertal children may lose their chance of recovery of vertebral height. The benefits of this must be weighed against possible future side effects. In the youngest children, our results indicate that early treatment may prevent and even amend skeletal deformity, especially spinal deformity. Our study confirms ours and others' previous reports showing persisting long term effects, and give evidence of more pronounced effects by starting pamidronate treatment at an early age (table 1). As there are no long term safety data in children and potential side effects are unknown, it is important to follow the patients into late adulthood.
No cure for OI is likely in the near future. The high frequency of new mutations and the fact that nearly every family has its own unique mutation, as well as problems with control of gene expression, make the possibility of gene therapy complex. Two patients can have a similar phenotype and vary considerable in genotype, whereas two patients with the same mutation can differ profoundly in phenotype expression.4,31 It is therefore difficult to find a relevant control group. Earlier studies have described the natural course of the disease without medication.32–34 In our study, each patient is his or her own control, with a 3–6 month run in period.
The bisphosphonates have a low and variable intestinal absorption and a long half life in bone.9–11 Gastrointestinal side effects are common after oral administration, while small children may find it difficult to swallow tablets. We chose the intravenous route for these reasons and to prevent the variable bioavailability from interfering with our interpretation of the observed effects. An alternative to oral supplementation with 1,25-dihydroxycholecalciferol, to increase the concentration of serum calcium, would have been to give additional calcium orally. However, studies have shown that hypercalciuria is common in children with severe OI and that there is a correlation between dietary calcium consumption and urinary calcium excretion.35 Furthermore, high urinary excretion may lead to microcalcifications of the renal papillae.35 This indicates a need for caution with regard to calcium supplementation in these patients.
Several of our patients report that if treatment is delayed by one to two weeks, some low grade skeletal pain reappears and their wellbeing is negatively affected. This indicates a need for further medication and is not a promising sign for the prospect of discontinuing treatment. None of the patients have opted to terminate the treatment.
In evaluating the results, it is important to remember that in OI patients growth, several biochemical measures of bone turnover and bone density deviate from normal. In DXA measurements the z scores are calculated from a normal population with normal height, weight, and bone density and can therefore not be used to assess patients with OI.20,23 If this is corrected for, DXA could be a valuable tool in the evaluation of the effect of APD treatment. The improvement in DXA values may partially be caused by the increase of bone mineral values during normal growth, but we also see greatly increased values in type III patients after termination of growth. The increased height of vertebral bodies contradicts the possibility of new spinal compression fractures as an explanation for the increase in lumbar DXA values. Intramedullary rods falsely increase total body DXA values, so in some of our patients, the level was beyond normal values for healthy individuals (fig 2). Removal of rods during medication has in some cases resulted in decreased values (fig 2). There are no reports of changes of DXA values in larger groups of untreated patients with severe OI, although Plotkin et al reported a significant decrease in lumbar DXA values over a one year period in their historical control group of six patients with a mean age of 10.7 months at the start of observation.29
Fracture rate is difficult to assess without frequent x rays, which is not recommended for patients with OI, as the increased fracture rate can lead to high accumulated doses of radiation over time. Furthermore, the observed increase in mobility can increase the risk of fracture. We chose not to investigate fracture rate. However, most of the children or their parents reported a decrease in symptoms indicative of fissures or fractures during treatment.
It is well known that children with OI generally sweat more than normal. Most parents report a decrease in sweating during treatment. This might be because of a decrease in microfracture rate.
Pain is sometimes difficult to estimate in the more severe forms of OI. As these children have had fissures, compressions, and fractures since the neonatal period, they are used to a certain amount of skeletal pain, regarding this as normal, so tend to complain only when they suffer larger fractures. The mother of a 1 year old immobilised girl said that her daughter never had pain, but after two to three treatments she noticed that the girl moved in a quite different way when reaching for objects and soon started to turn around in her supine position. It is likely that this girl had previously experienced constant pain on gently moving her extremities. One 16.3 year old boy, with type IV OI, said that before treatment every movement was an effort, but now he felt as though he had “power steering” of his movements. It is clear that the intensity of pain is an essential part of the feeling of wellbeing. However, it is evident that a total absence of pain does not result in maximal wellbeing in all cases. We have therefore chosen to present both pain and wellbeing variables (table 1). Many children and adolescents with a severe form of OI do not take any analgesics as they do not experience a satisfactory effect at the standard recommended doses. The reduction in pain that occurs early in treatment permits more effective physiotherapy, which also positively affects mobility and might also affect fracture rate.22 Early body weight bearing with the aid of plastic orthoses, mobility devices, and intramedullary rodding provides stress to the lower limb bones and is of the utmost importance to avoid additional osteoporosis caused by immobilisation.22,36 Mechanical use of the skeleton in standing and walking also stimulates new bone formation.36 These positively interacting factors lead to an overall beneficial effect on the patients.
Our study shows that before APD treatment, most children with more severe OI were unable to benefit maximally from these other treatment modalities. Bisphosphonate therapy in children with OI should be used alongside physiotherapy, occupational therapy, and surgery to correct skeletal deformities. It does not replace rehabilitation and supportive care.
So far no other treatment for children with OI has shown this dramatic beneficial effect with improved quality of life. We advise comparing different studies regarding different types of bisphosphonates, forms of administration, doses, and dose intervals in order to find the optimal treatment that interferes as little as possible with the patient's normal life. Oral treatment would be the treatment of choice if an adequate preparation regarding intake, side effects, and dosage could be available.
Acknowledgments
This study was supported by grants from the Norrbacka Eugenia Stiftelsen, RBU, Stiftelsen Samariten, and Sunnerdahls Handikappfond. A grant from the Socialstyrelsen supported establishment of the multidisciplinary specialist team for osteogenesis imperfecta at the Astrid Lindgren Children's Hospital. We especially thank our collaborators in this team.