Article Text

Abstract
Simplified guidelines for the emergency care of children have been developed to improve the triage and rapid initiation of appropriate emergency treatments for children presenting to hospitals in developing countries. The guidelines are part of the effort to improve referral level paediatric care within the World Health Organisation/Unicef strategy integrated management of childhood illness (IMCI), based on evidence of significant deficiencies in triage and emergency care. Existing emergency guidelines have been modified according to resource limitations and significant differences in the epidemiology of severe paediatric illness and preventable death in developing countries with raised infant and child mortality rates. In these settings, it is important to address the emergency management of diarrhoea with severe dehydration, severe malaria, severe malnutrition, and severe bacterial pneumonia, and to focus attention on sick infants younger than 2 months of age. The triage assessment relies on a few clinical signs, which can be readily taught so that it can be used by health workers with limited clinical background. The assessment has been designed so that it can be carried out quickly if negative, making it functional for triaging children in queues.
- emergency triage
- guidelines
- developing world
Statistics from Altmetric.com
Improving the initial emergency management of severely ill children has received substantial attention and resources in developed countries, where many clinicians have been prepared to deliver rapidly standardised emergency management by undertaking training courses such as the advanced paediatric life support (APLS1 and PALS2), and several nursing and paramedic3paediatric emergency curricula. In contrast, the initial triage of sick children arriving at hospitals in developing countries is often deficient, with severely ill children experiencing delays in the institution of life saving emergency treatment. A World Health Organisation study surveying hospital care in seven developing countries showed numerous, significant deficiencies in triage and emergency care—for example, no standardised assessment and treatment guidelines, understaffing (especially at night), poorly trained staff, little appreciation of the need for urgent treatment, inadequate facility organisation for triage, and inadequate drugs and supplies.4 The study paediatricians estimated that improving triage and emergency care would contribute substantially to reducing morbidity and mortality in infants and young children brought to hospital.
A study in the under fives' clinic in a large hospital in Malawi (J Robson, V Lavy, unpublished data, 1997) showed that children requiring emergency care are often not recognised promptly. The initial contact with sick children was by a nurse who observed the clothed child during weighing. Of 250 sick children presenting for care, nine were considered by an APLS trained doctor to require emergency care. The mothers of three convulsing or post ictal children and one child in severe respiratory distress alerted the staff directly; two others with respiratory distress were recognised as requiring emergency management only after waiting in the queue for weighing. The remaining three were weighed then sat in the routine queue for care—two with neonatal sepsis and one with severe dehydration. A separate study in the same institution examined the triage of 50 severely ill children who were ultimately admitted (45), died before admission (two), or were treated in the emergency room or absconded before admission (three). Only 13 of the 50 children were identified by a nurse as requiring urgent care; five were brought forward by the caretaker; and 32 waited in the queue. Key emergency drugs were also frequently out of stock.
Pneumonia, diarrhoea, malaria, measles, and malnutrition remain leading contributors to child mortality in developing countries. The WHO/Unicef initiative to improve the integrated management of childhood illness (IMCI)5 has so far concentrated on outpatient management. These guidelines assume that severely ill children are referred to hospital where this is feasible. Many deaths occur in the first 24 hours after arrival at hospital. Some arrive too late but some will benefit from more rapid institution of appropriate care.
Technical basis for the emergency triage assessment and treatment guidelines
As part of the WHO IMCI effort to strengthen referral level paediatric care, guidelines have been developed to improve the triage of all sick children arriving at the outpatient clinic, accident and emergency department, or directly to the ward, and to provide timely, appropriate emergency treatment. The technical basis for the emergency triage assessment and treatment (ETAT) guidelines were based on input from an expert group of clinicians within a project coordinated by the WHO division of child health and development with input from multiple WHO programmes and outside experts.
The ETAT guidelines have many similarities to the initial approach to paediatric medical emergencies taught in APLS and other paediatric emergency courses. They are based on standardised emergency management by health workers involved in the initial triage and emergency treatment and use a rapid ABCD (airway,breathing,circulation,disability) approach. Although systematic improvements in emergency medical services, including an ABCD approach to initial assessment, started with adult trauma and cardiac care in the 1970s, specific initiatives to improve the emergency management of children were active in the US and UK by the early 1980s and are now widespread in developed countries.6
There are several significant differences based on resource limitations and the epidemiology of severe paediatric illness and preventable death in developing countries with raised infant and child mortality rate. In these settings, it is important to address the acute management of diarrhoea with severe dehydration, severe malaria, and severe malnutrition, conditions which are uncommon in developed countries. Bacterial pneumonia is still much more important than bronchospasm as a cause of respiratory distress and death in most developing countries. Special attention also must be paid to young infants under 2 months of age because of the substantial proportion of death which occurs in this age group in developing countries.
As with outpatient case management guidelines for diarrhoeal disease, acute respiratory infections (ARI) and IMCI, simplified guidelines allow a broader range of staff with less training to learn and implement effective case management. This is of crucial importance for teamwork and for understaffed referral facilities, particularly in settings where a doctor may only be on premises during the morning.
Emergency triage assessment
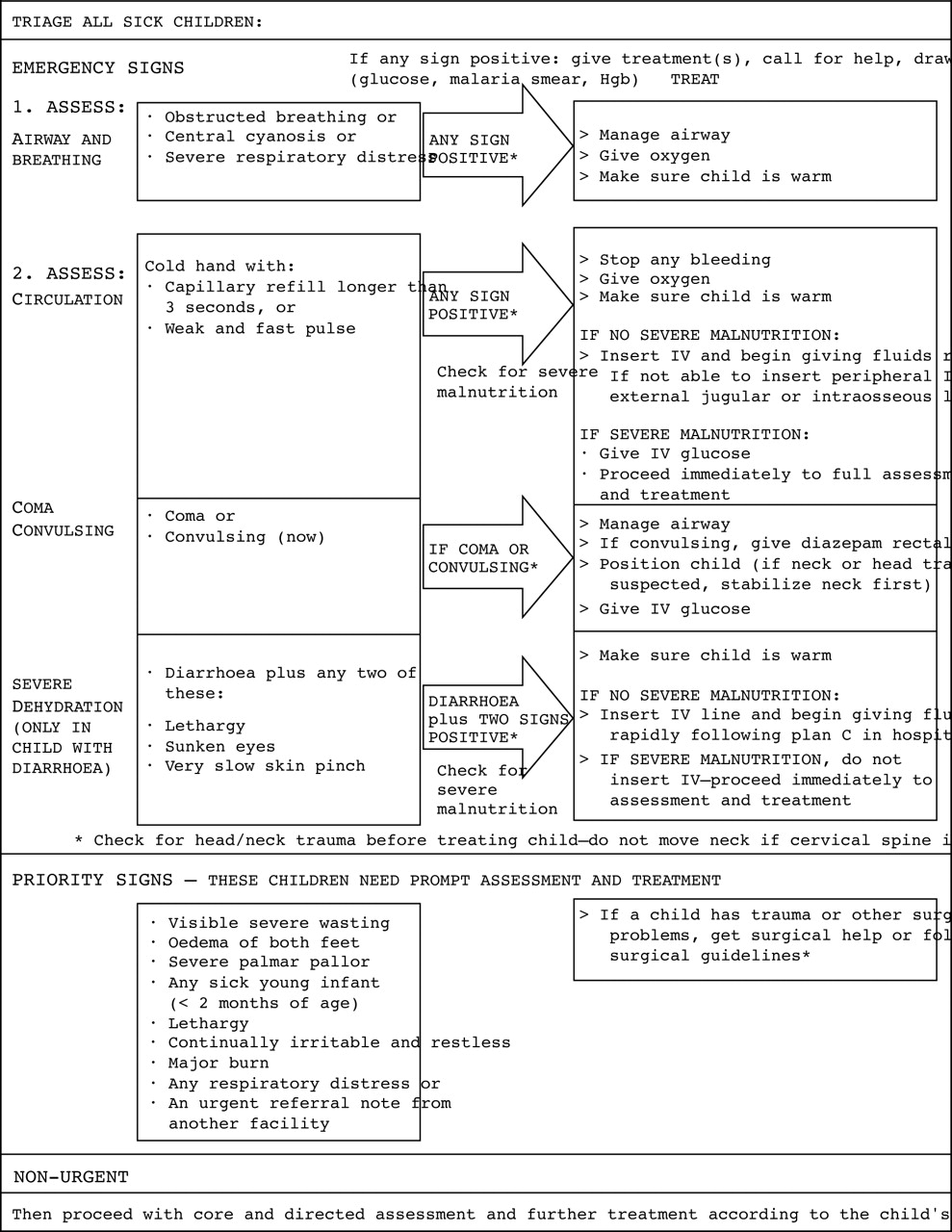
All sick children are classified either as: having an emergency sign which requires immediate emergency treatment; having a priority sign which requires prompt full assessment and treatment; or as a non-urgent case, which can wait for assessment and treatment (fig 1).
{kind=link}
Paediatric emergency triage assessment and treatment (ETAT) draft flowchart. Clinical signs added after the Brazil validation study are indicated in italics.
The assessment uses a minimum number of clinical signs (fig 1, table 1) and is designed to be carried out within 15–20 seconds unless emergency signs are identified which require further assessment and treatment. If all emergency signs are negative, their assessment consists only of rapid visual inspection for breathing, respiratory distress, cyanosis, coma, lethargy, irritability or restlessness, and convulsions; feeling the child's hand for warmth; and a question to the mother on diarrhoea. Further examination for the priority signs involves looking for visible severe wasting (including a visual inspection of the arms and legs and a quick glance under the child's shirt to exclude severe marasmus which can be missed if only the face is examined); checking for oedema of both feet; checking the palms for severe pallor; and identifying those with a major burn, with an urgent referral note, or under 2 months of age.
Assessment for emergency conditions requiring immediate treatment
Signs were chosen which are relatively easy to teach to health workers of various clinical backgrounds and do not require equipment. The need for adequate specificity and sensitivity in identifying emergency conditions for immediate institution of emergency treatment, even in the absence of a doctor, informed the choice of signs and led to the validation studies, one of which is reported in an accompanying paper.7
AIRWAY AND BREATHING
Acute lower respiratory infections, mostly bacterial pneumonia, are usually the first or second cause of death in developing countries,8 so care must be taken to assure prompt, effective treatment of pneumonia. Respiratory distress is based on a qualitative observation of laboured breathing (not getting enough air into the lungs) accompanied by distress. The accompanying manual clarifies that a child who is talking, drinking or feeding comfortably, or who appears happy, does not have respiratory distress. The quick assessment for breathing (look for chest movement, listen for breath sounds, feel for the breath) is skipped if the child is alert, active, talking, or crying. Cyanosis is based on examining the lips and, if these are blue, the tongue and inside of the mouth. If any of these emergency signs are present, airway management and oxygen treatment are immediately implemented. Further assessment and treatment of the child with respiratory distress involves counting the respiratory rate, observation for lower chest indrawing and the other signs; the differential diagnosis is considered and treatments instituted (antibiotics, rapid acting bronchodilators, etc) as described in the referral care manual.9 Experience with ARI and IMCI training10 has shown that examination for lower chest wall indrawing, an important sign of severe pneumonia, is difficult to teach and requires careful positioning and calming of the child. Hence it is not included in the rapid triage assessment.
CIRCULATION
For most children, only a rapid check that their hand is warm is required. If it feels cold, capillary refill is checked. If this is prolonged or the pulse is fast and weak, the child is treated for shock. Prolonged capillary refill is defined in these guidelines as 3 seconds or longer (rather than 2 seconds) to increase specificity, given concerns about the performance of this sign.11 12Since the child must be in a warm environment for prolonged capillary refill to perform adequately,13 the training materials indicate that the pulse should be relied on if the room is cold. The radial pulse is initially felt; if it cannot be felt or if it feels weak, a more central pulse is checked.
COMA AND CONVULSIONS
If the child is not awake and alert, the health worker tries to rouse him or her by talking and then shaking the arm. If the child does not respond, the mother is asked whether the child has been abnormally sleepy or difficult to wake. If she confirms that the child is not just sound asleep, the child receives emergency treatment for coma. This same examination determines whether the child is lethargic (responds to voice but remains drowsy and does not show interest in what is happening around him/her). These are modifications of the AVPU scale (awake; responds tovoice; responds only topain;unconscious) for triage use. Emergency treatment for convulsions is limited to those characterised by loss of consciousness and obvious “uncontrolled, jerky movements”. Convulsions from severe malaria are usually tonic-clonic.
DIARRHOEA
The emergency assessment for severe dehydration has been simplified, based on substantial experience with the WHO diarrhoeal disease control14 and IMCI guidelines. Only three signs are assessed—sunken eyes, very slow skin pinch, and lethargy—only two being required for treatment for severe dehydration. Excluding an assessment of the child's ability to drink speeds the examination and would be expected to increase the specificity in classifying dehydration as severe. If the child is severely malnourished (based on visible severe wasting or oedema of both feet), an experienced clinician is requested to make an immediate complete assessment and decision on fluids, given the difficulty in diagnosing dehydration and hypovolaemic shock in a severely malnourished child and the need for modified fluid recommendations.
LABORATORY TESTS
Only three emergency laboratory tests are assumed to be available: haemoglobin, blood smear for malaria, and dipstick for blood glucose.
Emergency treatments
ETAT provides guidance for the initial 5–15 minutes of care for severe medical illness and refers to other guidelines for trauma or surgical management. The treatment recommendations for airway management, positioning, and the administration of intravenous fluids, glucose, and rectal diazepam15 have been simplified (table2), and are based on a very limited number of drugs. These should be immediately administered by nursing and paramedical staff based on the presence of a few key clinical signs, despite lack of a specific diagnosis, while a more senior clinician is called to carry out a further assessment, make a differential diagnosis, and institute additional life saving treatments such as parenteral antimalarials, antibiotics, and rapid acting bronchodilators.
ETAT emergency treatments
The ETAT guidelines assume no cardiopulmonary resuscitation or intubation as part of emergency management since intensive care units and mechanical ventilation are often unavailable. Although the use of intraosseous infusion16 will be new to many clinicians, it is an effective way to administer fluids when a peripheral intravenous line cannot be inserted rapidly,17 provided the needle is inserted with strict aseptic technique and removed within eight hours to prevent infection. If an intraosseous needle is not available, a 21 gauge intravenous needle or a large gauge spinal needle can be substituted.
The rapid fluid replacement for children with diarrhoea and severe dehydration who do not have signs of shock is identical to the WHO diarrhoeal disease11 and IMCI guidelines.18Only children with diarrhoea with severe dehydration are treated with intravenous fluids; children with some dehydration are treated with oral rehydration therapy, whereas APLS and PALS guidelines assume intravenous treatment for these children.
Field testing and the further development of interventions to improve emergency case management
A series of studies were planned to validate the guidelines and to evaluate feasibility and constraints to their implementation.
The first validation study was carried out in Pernambuco State, Brazil.7 A similar validation study is now being completed in Malawi. Training, facility reorganisation to facilitate prompt attention to sick children on initial arrival, and improvement in the supply of emergency drugs are all necessary to implement the ETAT guidelines. It is essential that the drugs required for emergency treatment are immediately available without requiring parental purchase. It is also important to continue efforts to encourage prompt careseeking by families when children develop danger signs and to overcome financial and logistical barriers to seeking referral care. ETAT is only one of many interventions to reduce mortality at the referral level.
The need to train both nurses and paramedical staff as well as doctors in ETAT came from a recognition of limited small hospital staffing in many settings, particularly in the afternoon and at night, and the fact that severely ill children may arrive at several hospital locations— in the outpatient queue, in the accident and emergency department, or directly to the ward. Health workers at small hospitals or health centres in developing countries are usually multipurpose and have a wide range of basic and clinical education. Training in ETAT for a range of staff is necessary to assure adequate triage and emergency care around the clock and in all relevant hospital locations. Simplified guidelines in similar format are in development for the initial emergency obstetric and medical care of adults.
Acknowledgments
The WHO IMCI referral care project included staff and contractors working for WHO Child Health and Development (CHD), Malaria Unit of the Special Programme for Research and Training in Tropical Diseases (TDR) and Control of Tropical Diseases (CTD), UNAIDS, Reproductive Health (RHT), Nutrition (NUT), and the Expanded Programme on Immunization (EPI). These designations apply to the WHO headquarters structure as it was at the time of the study.