Article Text

Abstract
There is renewed interest in the phase of partial remission in recently diagnosed diabetes because of the potential for pharmacological and immune intervention to preserve β cell function. 95 children younger than 10 years were investigated to assess the influence of age, sex, diabetic ketoacidosis (DKA), admission at diagnosis, and ethnicity on the frequency of remission and insulin requirements during the first two years after diagnosis. Partial remission was defined as a requirement of insulin < 0.5 U/kg body weight/day. There was partial remission in 41 patients, with no differences for children aged 2–4 years and those aged 5–9 years. None of the five children aged < 2 years remitted. Forty five of 95 children were admitted to hospital at diagnosis, of whom 26 of 45 had DKA (blood pH < 7.25). In this number of children we were unable to show a statistical difference in the rate of remission with respect to DKA, admission to hospital at diagnosis, sex, or South Asian ethnic background. There were no differences in insulin requirements between the different groups by the end of two years and at that time seven of the children required insulin < 0.5 U/kg/day. The results suggest that even in preschool children there is potential for attempting to preserve β cell function.
- diabetes
- remission phase
- age
Statistics from Altmetric.com
Despite its acute clinical onset, type 1 insulin dependent diabetes mellitus (IDDM) develops as the culmination of a prolonged preclinical phase of progressive destruction of the pancreatic islet cells.1 After diagnosis a large proportion of recently diagnosed children and adults with IDDM pass into a phase of partial remission,2 characterised by continuation of endogenous insulin secretion, reduced exogenous insulin requirement, and good metabolic control.3-5
There is renewed interest in remission, or spontaneous β cell recovery, because it has important implications in terms of potential pharmacological intervention and immuno modulation.6Moreover, it has been suggested that admitting children to hospital at diagnosis (and intermittently thereafter) to initiate intensive intravenous insulin treatment might induce a longer remission phase.7 ,8 This suggestion is linked to the hypothesis that insulin administered before clinical diagnosis might prevent or delay the onset of IDDM.9 It is also believed that the preschool child with diabetes is less likely than older children to demonstrate complete or partial remission,10 ,11 based on the premise that younger children are more likely to present with ketoacidosis, and are considered to have more β cell failure, with a more aggressive autoimmune disorder.12 ,13
The aim of our study was to assess the frequency of partial remission in younger children, particularly because of the potential to sustain the remission phase and thus attain better long term metabolic control.
Study population and methods
We reviewed notes on 110 children diagnosed with IDDM under the age of 10 years during the years 1981–91 who had been notified to the Leicestershire Diabetes Register. We abstracted data for the first two years after diagnosis at 1, 3, 6, 12, 18, and 24 months, recording height, weight, insulin requirement, glycated haemoglobin (HbA1) concentrations, length of history of symptoms, ethnic origin (particularly children of Indian subcontinental South Asian extraction), duration of admission to hospital, and presence of diabetic ketoacidosis (DKA) at diagnosis.
We defined partial remission as insulin requirement < 0.5 U/kg/day, and DKA as blood pH < 7.25.
STATISTICS
We analysed data using the SAS statistical software package, calculating proportions, means, Fischer’s exact tests, and χ2 tests of independence as appropriate. The confidence interval analysis (CIA) software was used to estimate 95% confidence limits for proportions and their differences.14
We compared differences in insulin requirements between subgroups over the study period by the method of summary measures. For each child we calculated the area under the curve for insulin requirement over time using the trapezium rule and standardised the result by dividing by the study period.15 We then compared these summary measures using the Student’s t test or the Mann-Whitney U test as appropriate.
Results
Of 110 patients potentially available for study, we included 95 (86.3%). We excluded 15 children because hospital records were not available for six, four had moved from Leicestershire, and five had moved into Leicestershire after the diagnosis. All 95 patients received insulin at diagnosis and have continued to do so.
Table 1 describes the initial characteristics and subgroups of patients at entry and summarises the remission results. A total of 41 patients showed some period of partial remission during their first 24 months. We observed similar remission rates in those aged 2–3, 4–5, 6–7, and 8–9 years at diagnosis. None of the five children aged less than 2 years at diagnosis showed partial remission (three of these were admitted to hospital with DKA). More boys than girls and more white than South Asian children showed partial remission, but differences were not significant (sex: χ2 = 0.896 1 df, p = 0.33; ethnicity: Fischer’s exact test (two tailed), p = 0.34).
Patient characteristics, remission details, and 95% confidence intervals (CI) for differences
Fewer children presenting with DKA and admitted to hospital had a remission than those admitted with no DKA or those not admitted, but these differences were not significant (χ2 = 3.02 2 df, p = 0.22).
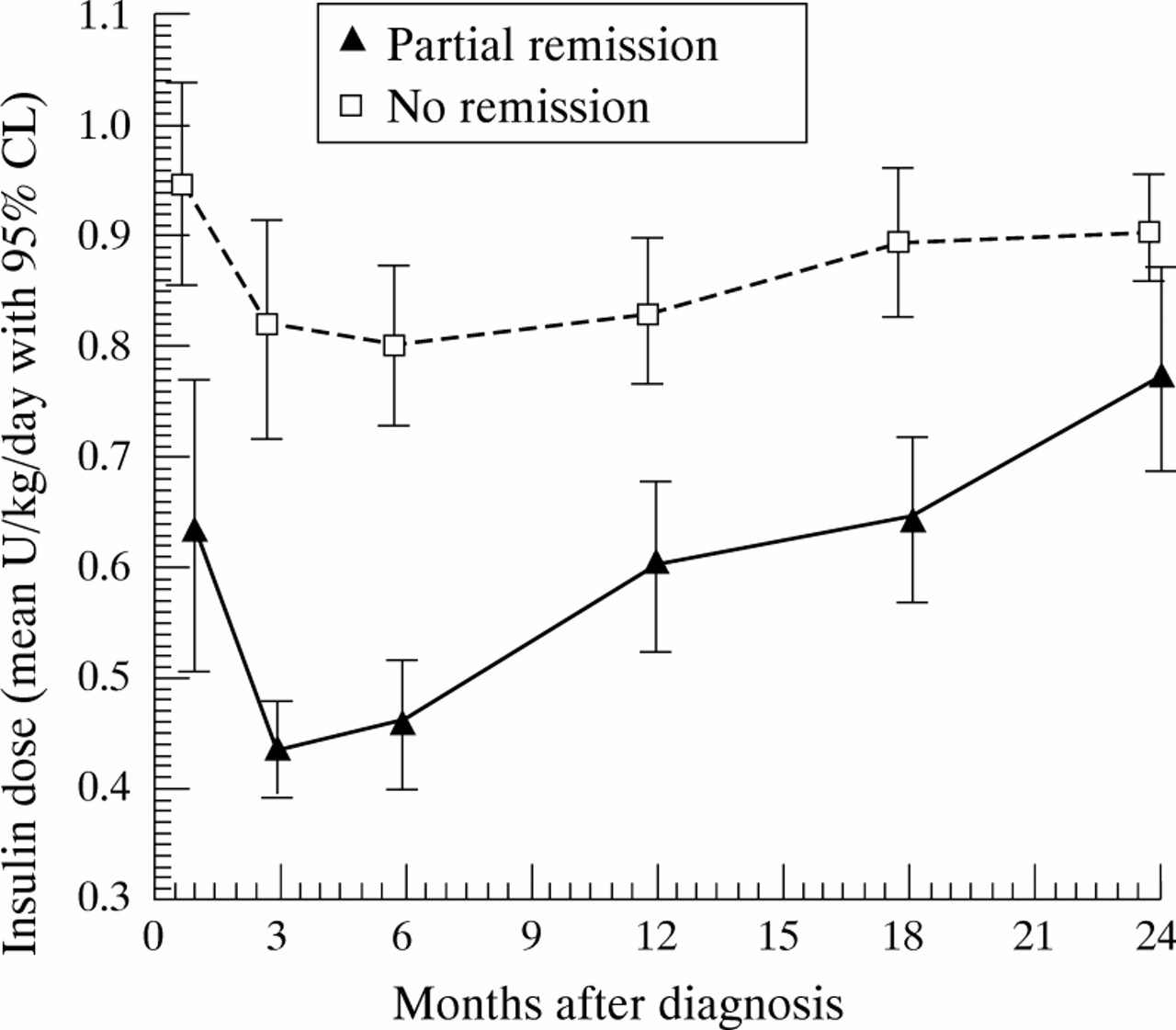
At three months after diagnosis, 29 of the cohort were in remission (about one third each of children < 5 years at diagnosis and of those aged 5–9 years). By 12 months these figures had fallen to 4 of 36 and 11 of 64 in the younger and older age groups, respectively; by 24 months these figures had fallen further to 1 and 6, respectively. Throughout the two years the mean insulin requirement was less for those diagnosed aged 5–9 years compared with the younger age group but the differences were not significant (p = 0.13) and mean insulin requirement for boys was ∼ 8% lower than for girls (not significant, p = 0.14). For children showing any period of remission the insulin requirements were significantly lower from the first data collection point at one month through to 24 months compared with children not showing remission (fig 1; p < 0.01).

{kind=link}
Mean insulin requirement over time with 95% confidence limits (CL), by observed partial remission.
There were insufficient data on glycated haemoglobin to relate this to age groups and insulin dosage.
Discussion
We found statistically similar percentages of children showing partial remission in 2 year age bands from ages 2 to 10 years. However, two years after diagnosis, the exogenous insulin requirement was not significantly different between groups when related to previous remission, age, ethnicity, sex, admission at diagnosis, and initial DKA. No child diagnosed under the age of 2 years remitted and their insulin dosage over the two years was higher than older children.
Estimates of the incidence of remission in IDDM have varied widely, partly reflecting the use of different definitions. Drash described a large cohort in the age group 0–15 years using the same definition (insulin dosage < 0.5 U/kg/day) and found that 70% partially remitted, and that remission occurred more often in older children, in boys, and in those not presenting with severe ketoacidosis.10 He noted, as we did, a lower (10%) insulin requirement in boys.
In another large cohort (using the same definition), the remission rate at three months was 59% and at one year 36%, the remission period being identical in children diagnosed at < 5, 5–10, or 10–15 years of age.16
Applying a different definition—the fall in insulin requirement of at least 33% from dose at discharge from hospital—earlier small UK studies quoted 15–40% of remissions in various age groups.17 ,18
The major criticism of these clinical definitions is that they do not estimate the physiological basis of remission, namely endogenous insulin secretion, or the outcome in terms of glycated haemoglobin. Agner et al showed that C-peptide concentrations were higher and glycated haemoglobin concentrations were lower in the third of their patients under the age of 16 years who remitted.4 Unfortunately, in our cohort glycated haemoglobin measurements in the first 12 months after diagnosis were insufficient to provide valid data but we note that the group of children remitting had significantly lower insulin requirements within the first weeks after diagnosis (fig 1) and this is associated with clinically excellent glycaemic control. This is important because recent evidence from large multicentre studies suggests that good diabetic control achieved soon after diagnosis is more likely to be sustained (T Danne, unpublished data, 1998).19 The reverse is often observed—that poor control early on in diabetes is more likely to be associated with continuing unsatisfactory control thereafter.
Extensive clinical, genetic, and biochemical studies of the early months of diabetes after clinical onset in Finland have shown that in children diagnosed under the age of 2 years, DKA is more likely, partial remission is uncommon, and serum C-peptide concentrations are low.13 Our finding of no remission and higher insulin requirements in the infants < 2 years old is consistent with this. The intensity of β cell destruction is associated with genetic determinants, particularly HLA DR3/DR412 or DQB1 0302/0201 heterozygosity.20 Thus, the continuation of residual β cell function and partial remission may vary between different genetic subgroups in different countries.21
Perhaps of greater clinical importance in the UK and elsewhere is the fact that care of newly diagnosed children with IDDM is shifting towards domiciliary and community management.22 ,23Therefore, the suggestion that intensive insulin treatment at disease onset might prolong and deepen the remission phase8 causes some concern, especially as recent data from the diabetes control and complications trial (DCCT) tends to support this idea.19Our results do not contribute to this important debate partly because we were unable to document the relation between insulin dose, residual β cell function, and metabolic control. Therefore, it remains to be seen whether exogenous insulin before onset,9 or intensive insulin treatment afterwards,7 ,8 ,24 can appreciably preserve β cell function and alter the long term clinical outcome of children with diabetes.
We have shown that in children given conventional insulin treatment and often managed initially out of hospital, over 40% of preschool and older children go into a transient phase of partial remission. This is a higher figure than in some reports, but significantly lower than in others, and it will be important to test prospectively whether the differences are a result of genetic or pathophysiological dissimilarities, or whether more intensive insulin treatment at diagnosis might prolong the remission phase.
The partial remission phase should be reflected by glycated haemoglobin concentrations close to normal, and careful monitoring of these concentrations during the first two years after diagnosis might provide a useful audit of the success or failure of diabetes management in children.
We conclude therefore that the “honeymoon period” with continuation of endogenous insulin secretion continues to provide a window of opportunity for the evaluation of insulin treatment and potential new treatments in an attempt to preserve pancreatic β cell function and to establish a pattern of optimal metabolic control.