Article Text

Abstract
Prolactin, a polypeptide hormone of anterior pituitary origin, has pronounced physiological effects on growth, reproduction, and osmoregulation. Increasing evidence indicates that prolactin also has an immunomodulatory influence on the immune system. The status of prolactin in patients with coeliac disease was investigated by obtaining serum samples from 48 patients with active and non-active coeliac disease. These were compared with samples from 20 children with familial Mediterranean fever and 65 normal controls. Serum prolactin in patients with active coeliac disease was significantly higher than in the other groups studied and reference values. Serum prolactin correlated well with the degree of mucosal atrophy and with the serum concentration of antiendomysial antibodies. Prolactin may play a part in immune modulation in the intestinal damage of coeliac disease and serve as a potential marker for disease activity.
- coeliac disease
- prolactin
Statistics from Altmetric.com
Coeliac disease is a disorder in which the immune response to ingested gluten, a water soluble storage protein of wheat, is accompanied by intestinal mucosal damage. The resulting atrophy of the villi of the proximal small intestine leads to the malabsorption of nutrients and diarrhoea. Symptoms and epithelial damage can be resolved by excluding gluten from the diet. Although a variety of pathogenic mechanisms has been suggested, most evidence suggests that the tissue damage occurs as a consequence of the immune response.1The involvement of both humoral and cellular immune pathways in coeliac disease indicates that the immune system plays a major part in the development of the disease. Evidence for humoral immune activation in coeliac disease is obtained from the increased production of antigliadin, antireticulin, and antiendomysial antibodies in active coeliac disease.2 The involvement of cellular immunity is implied by several findings such as an increase in the number of mitogen primed memory cytotoxic T cells (CD 45 RO+) in the atrophied intestine and in the percentage of T cells expressing γδT cell receptor subsets in the damaged mucosa.3 Coeliac disease exhibits many of the characteristics of an autoimmune disease, including polygenic inheritance, human leucocyte antigen linkage, target organ lymphocyte infiltration, restricted use of the T cell receptor, and its association with other autoimmune disorders.3 4 Coeliac disease may therefore be regarded as a disorder initiated in genetically predisposed subjects by an undefined trigger, in which the immune response, induced by ingested gluten, leads to organ specific tissue damage.
Prolactin has been implicated as an important in vivo modulator of cellular and humoral immunity. Experimental evidence suggests that sex linked hormonal factors influence the immune response and modify the expression of autoimmunity in animals and humans.5 6Prolactin is a polypeptide hormone of anterior pituitary origin which has pronounced physiological effects on growth, reproduction, and osmoregulation in a wide range of species.7 As both coeliac disease and prolactin affect humoral immunity, cell mediated immunity, and autoimmunity,2 8 we evaluated serum prolactin in patients with active and treated coeliac disease with respect to the severity and activity of the disease.
Patients and methods
Forty eight patients with coeliac disease who fulfilled the diagnostic criteria of the European Society of Paediatric Gastroenterology and Nutrition9 were divided into two groups. The first group comprised 26 children with active coeliac disease (mean age 11.3, range 5–18 years, ratio of girls to boys 1:1) receiving a diet containing gluten. The second group comprised 22 children with coeliac disease (mean age 9.0, range 4–15 years, ratio of girls to boys 1.2:1) in remission who had been receiving a gluten free diet for at least one year.
The patients with coeliac disease were compared with two other groups of 85 children. One comprised 65 normal schoolchildren who were seen at an outpatient clinic for routine check ups (mean age 11.5, range 5–18 years, ratio of girls to boys 1:1). The other group included 20 children with familial Mediterranean fever (an inflammatory disease) seen at a paediatric rheumatology immunology clinic (mean age 6.8, range 5–18 years, ratio of girls to boys 1:1). Informed consent was obtained from the parents and the study was approved by the hospital’s institutional review board.
All patients with coeliac disease underwent upper gastrointestinal endoscopy with a GIF-XQ-10 endoscope (Olympus, Japan). A small intestinal biopsy sample was taken from the third part of the duodenum and routinely processed for histological examination. The specimens were graded I–IV according to the degree of intestinal atrophy, as described previously.10
The basal concentration of prolactin was determined in all patients and defined as the prolactin concentration in the serum or plasma without stimulation.11 All blood samples were obtained in the mid-morning. Serum samples were collected and frozen at −70°C until analysis. The serum prolactin level was measured by immunoradiometric assay (Promed, Holland).12 Normal concentrations of prolactin ranged from 5 to 20 μg/l and hyperprolactinaemia was defined at >20 μg/l. The intra-assay coefficient of variance was 3% and the interassay coefficient of variance was 5%. None of the subjects with hyperprolactinaemia had been treated with drugs known to raise prolactin levels (such as chlorpromazine, metoclopramide). The results of thyroid, liver, and kidney function tests were normal in all patients.
Tests for the IgA antiendomysial antibody were performed by an indirect immunofluorescence assay as described previously.13 Serum samples were screened at serial dilutions and, if positive, the highest dilution yielding a positive reaction was reported.
The means were compared by one way analysis of variance.
Results
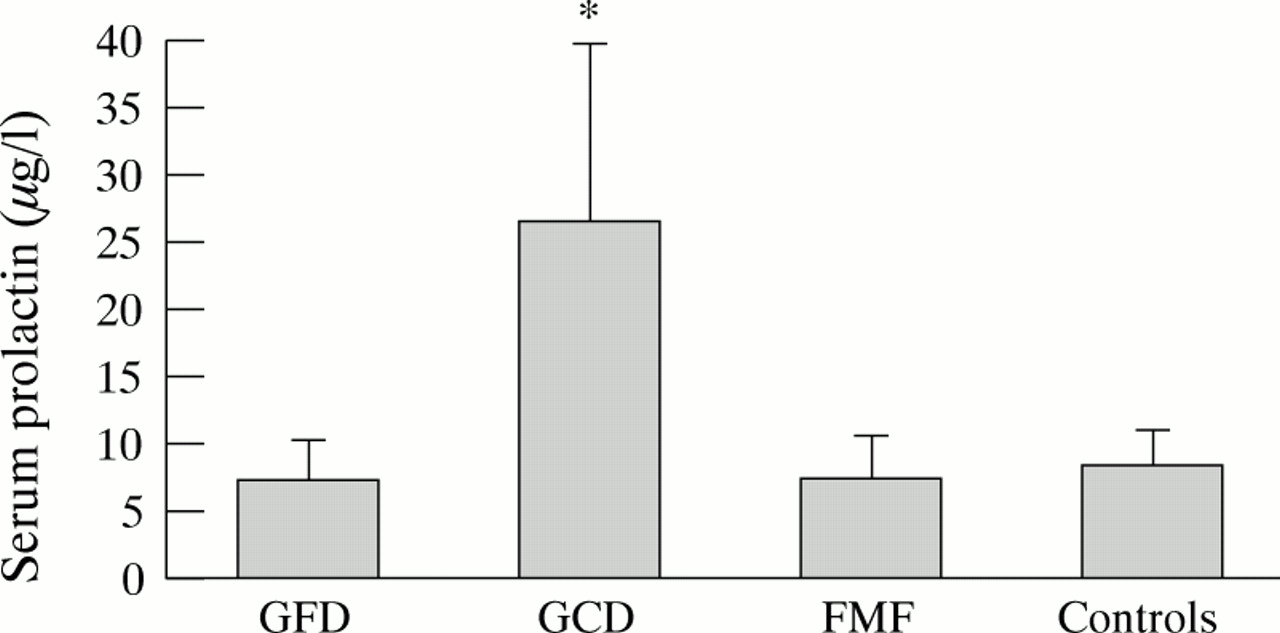
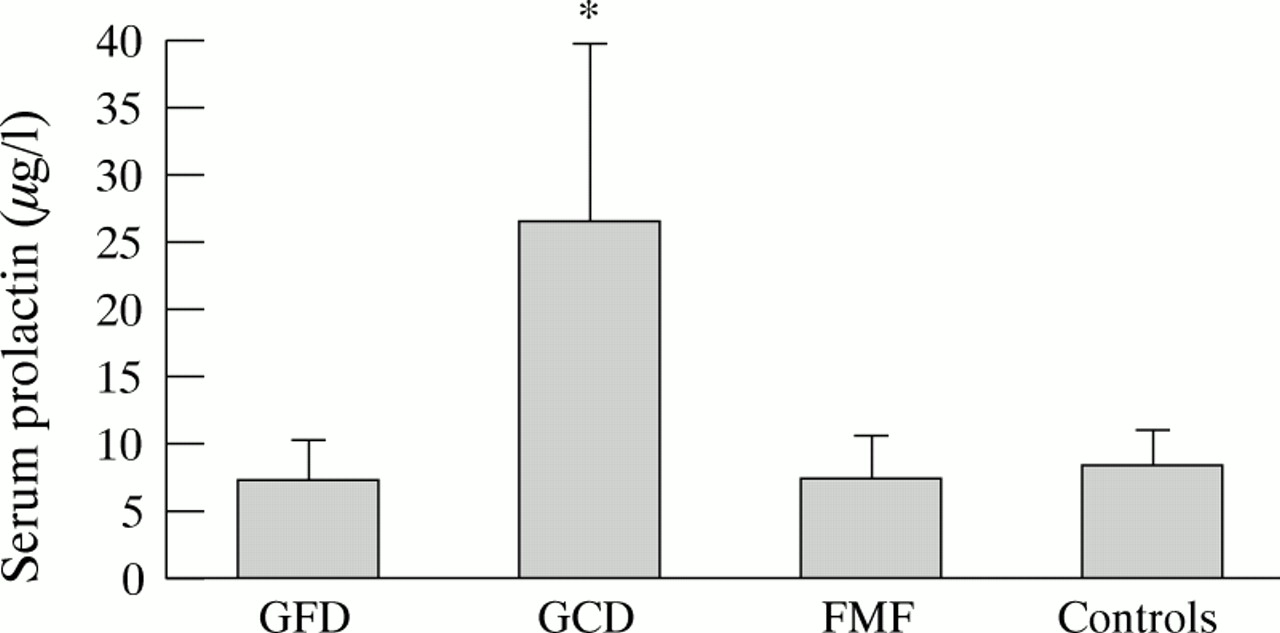
Mean serum prolactin concentrations were lowest in children with familial Mediterranean fever, those with inactive coeliac disease, and in the healthy children (fig 1), and highest in patients with active coeliac disease (p <0.01). Prolactin concentrations were higher than normal (> 20 μg/l) in seven of the patients with active coeliac disease. In the patients with coeliac disease on a gluten free diet, small intestinal biopsy specimens were histologically normal, whereas six patients with coeliac disease on a diet containing gluten had grade II atrophy, three had grade III atrophy, and 10 had total atrophy (grade IV). Antiendomysial antibodies were detected in all children with active coeliac disease. The antibody titre was widely distributed, ranging between 1:5 and 1:160. A close correlation was found between the grade of mucosal atrophy and the prolactin concentration: the higher the grade of mucosal atrophy, the higher the measured prolactin (p <0.004, r = 0.98). A positive correlation was observed between the levels of antiendomysial antibodies and prolactin (p <0.02, r = 0.91). No correlation was detected between the prolactin level and the patients’ age or sex.
{kind=link}
Mean (SD) serum prolactin concentrations (μg/l) in children with coeliac disease on a gluten free diet (GFD), children with coeliac disease on a gluten containing diet (GCD), children with familial Mediterranean fever (FMF), and normal controls. Asterisk indicates higher than GFD, FMF, and control group (p <0.01).
Discussion
A link between the neuroendocrine and immunological systems has been established.14 Endocrine and autocrine mediators and receptors of the immune and endocrine systems may explain changes in immune function in response to environmental stimuli perceived by the central nervous system.15 Prolactin may play a part in the regulation of both humoral and cell mediated responses.15Although both T and B lymphocytes contain prolactin binding sites, the growth promoting properties of prolactin are more evident in populations of T cells.
Prolactin participates in the immune regulation and stimulation of autoimmunity in human autoimmune disease. High serum prolactin concentrations were reported in male patients with systemic lupus erythematosus and in autoimmune thyroid disease.15 16 No correlation has been found between the activity of the disease in patients with systemic lupus erythematosus and prolactin values, however.17 Furthermore, in an abstract describing increased prolactin concentrations in an untreated man with coeliac disease,18 a possible trophic effect of prolactin in patients with coeliac disease has been suggested.
In this study higher serum prolactin concentrations were found in patients with active coeliac disease on a diet containing gluten than in patients with coeliac disease on a gluten free diet. No difference in prolactin concentrations was found between the control group and patients with familial Mediterranean fever, suggesting that prolactin may play a part in the subgroup of patients with active coeliac disease. Familial Mediterranean fever was chosen as a control group because of its inflammatory nature, although we accept that a more appropriate control group might have been children with Crohn’s disease.
The significant correlation between the effect of serum prolactin on the degree of intestinal damage and the activity of serum antiendomysial antibodies further substantiates the relevance of our observations. As intestinal pathology and levels of antiendomysial antibodies are reliable markers for coeliac disease, serum prolactin concentrations may serve as an additional marker of disease activity.
The higher prolactin serum concentrations in gluten induced enteropathy may play a primary part in the immune modulation of intestinal damage or may represent a secondary phenomenon.