Article Text

Abstract
OBJECTIVE To assess the usefulness of the indirect immunofluorescence antinuclear antibody test (FANA) using human laryngeal epithelial carcinoma cells as nuclear substrate, to screen for childhood rheumatic diseases.
STUDY DESIGN A review of all FANA tests performed on children at British Columbia’s Children’s Hospital between 7 March 1991 and 31 July 1995.
RESULTS FANA tests were positive at titres of 1:20 or greater in 41% of all subjects tested, and in 65% of all subjects in whom the diagnosis was obtained. FANA positivity occurred in 67% of those with a rheumatic disease, compared with 64% of those with a non-rheumatic disease (p=0.4). More girls had high titre FANA positivity than boys independent of whether or not they had a rheumatic disease (p=0.05). At a screening serum dilution of 1:40 a positive test has a sensitivity of only 0.63, and a positive predictive value of only 0.33 for any rheumatic disease. For systemic lupus erythematosus (SLE), mixed connective tissue disease (MCTD), or overlap syndrome at a screening dilution of 1:40 the test has a very high sensitivity of 0.98, but a very low positive predictive value of only 0.10, the test having slightly better characteristics for boys than girls.
CONCLUSION Although a negative FANA test makes a diagnosis of SLE or MCTD extremely unlikely, a positive test even at moderately high titres of 1:160 or higher is found so frequently in children without a rheumatic disease that a positive result has little or no diagnostic value. It is suggested that a screening serum dilution of 1:160 or 1:320 would increase the usefulness of the test, by decreasing false positive tests, without significantly increasing false negative tests for SLE or MCTD, and would have the potential for considerable cost savings.
-
Use of HEp-2 cells as substrate has resulted in a FANA (fluorescence antinuclear antibody) test that is too sensitive
-
Most children with positive FANA tests (using HEp-2 cells as substrate) do not have a rheumatic disease
-
It is probable that the FANA test (using HEp-2 cells) should be abandoned as a ‘screening test’ for rheumatic diseases
-
It is possible that it would be more efficient to request an anti-DNA as the initial test if a physician believes a child has systemic lupus erythematosus
- antinuclear antibody test
- rheumatic diseases
- test characteristics
- systemic lupus erythematosus
Statistics from Altmetric.com
Antinuclear antibodies occur frequently in the sera of children with a wide variety of rheumatic diseases, including systemic lupus erythematosus (SLE), juvenile rheumatoid arthritis, and juvenile dermatomyositis.1-4 Their presence is one of the American College of Rheumatology classification criteria for adult SLE,1 and a recent study validating these criteria in childhood SLE demonstrated the presence of antinuclear antibodies in 94% of patients.4 Because of this association with rheumatic disease the indirect immunofluorescence antinuclear antibody test (FANA) is frequently used as a screening test for childhood rheumatic disease by paediatricians and other physicians. However very little is known about the characteristics of the FANA as a screening test. Two recent studies have suggested that the presence of antinuclear antibodies in childhood is not invariably associated with the development of a rheumatic disease.5 6 Since the early 1980s mouse liver or rat kidney as tissue substrates for the test have been replaced by cultured human laryngeal epithelial carcinoma (HEp-2) cells. This substrate appears to be generally more sensitive than are animal tissue sections to the presence of antinuclear antibodies both in patients and in controls.3 7 It is our clinical impression that there is now a very high false positivity rate for antinuclear antibodies, and that makes interpretation of a positive test result very difficult.
The aim of this study was to investigate the characteristics of the FANA, as performed at our institution, in the diagnostic investigation of children with possible rheumatic disease.
Methods
FANA TESTS
In the fall of 1996 we undertook a retrospective review of all FANA tests performed on sera from children by the clinical service haematopathology laboratory at British Columbia’s Children’s Hospital (the main tertiary care hospital for children in the province of British Columbia), from 7 March 1991 to 31 July 1995. From 7 March 1991 to 31 July 1993 the test used was supplied by Kallestad Diagnostics (Montreal), and from 1 August 1993 to the end of the study, the test kits were from Helix Diagnostics (Sacramento). For most of the time period of the study the initial serum dilution used was 1:20; from January 1995 the dilution was increased to 1:40. If the test was positive at the initial dilution, the serum sample was tested to endpoint with doubling dilutions. With each batch of tests there was a positive and negative control, and the test was performed as recommended by the manufacturers of the kit. If a serum sample was equivocal at the initial diagnosis the serum was retested.
DIAGNOSES
In order to obtain the most likely diagnoses on the children the following procedures were undertaken:
(1) Each physician ordering the test was contacted by letter asking for the most likely diagnosis, and in particular whether the physician believed that the child might have SLE or another connective tissue disease. In the letter the physician was also asked to state whether or not he/she believed that the FANA test was helpful in either diagnosing or excluding the diagnosis of SLE, and for any other comments he/she might have about the perceived usefulness of the test.
(2) The diagnoses of all children attending the paediatric rheumatology service who had a FANA performed during this period were obtained from a regularly updated computerised clinical database.
(3) The hospital records were searched for all children admitted with either a diagnosis of SLE or mixed connective tissue disease (MCTD) during this time period, so as to try and ensure that no cases of these diseases were missed.
(4) Charts were obtained from the health records department and were reviewed. These charts consisted of all children with high titre FANA results (⩾1:160), and a randomly selected number of charts of children with negative or low titre results.
All subjects with a diagnosis of SLE fulfilled the American College of Rheumatology classification criteria.1 A diagnosis of MCTD was made in those subjects with combined features of SLE, dermatomyositis, and/or scleroderma with negative anti-DNA antibodies, but positive antiribonucleoprotein (anti-RNP) antibodies. Overlap syndrome was diagnosed if a subject had features of a systemic connective tissue disease and had other antiextractable nuclear antigen antibodies in addition to anti-RNP without DNA antibodies and not fulfilling American College of Rheumatology criteria for SLE.
Rheumatic disease was considered to be any chronic inflammatory arthropathy, connective tissue disease (SLE, MCTD, overlap syndromes, juvenile dermatomyositis, scleroderma, etc), or vasculitis. Non-rheumatic disease was considered to be any other diagnosis. For the purposes of this study, transient arthropathies such as transient synovitis of the hip, osteomyelitis, or septic arthritis were considered non-rheumatic.
DATA ANALYSIS
The data were entered on a computerised database (Access, Microsoft). The test characteristics of the FANA for the diagnosis of ‘rheumatic disease’, and for SLE, MCTD, or overlap syndrome combined, were then calculated for different serum titres. If a subject had more than one FANA test performed during the study time period only the first test result was used.
Test characteristics were calculated and were based on the number of subjects with a known diagnosis, rather than the total number of subjects tested. The following characteristics for each serum dilution were calculated: sensitivity (true positive rate), specificity (true negative rate), positive predictive value (the probability that the disease is present with a positive test), negative predictive value (the probability that the disease is not present with a negative test), and receiver operator characteristic (ROC) curves (relationship of true positive rate to false positive rate).
STATISTICAL METHODS
The χ2 test was used to compare disease prevalence (rheumatic v non-rheumatic diseases) between the sexes. The joint effects of both FANA titre and disease on the sex distribution were examined using logistic regression. The ability of the FANA test to diagnose rheumatic disease, and SLE/MCTD/overlap disease was compared between boys and girls with the ROC Analyzer program of Centor and Keightley (R M Centor, J Keightley, version 5.01, unpublished) which uses the methods of Hanley and McNeil8to compare the areas below the ROC curves.
Results
During the study period there were 1369 individual children tested of whom 558 (41%) were positive at a titre of 1:20 or greater. In those 699 subjects with a known diagnosis FANA positivity occurred in 454 (65%).
FANA ENDPOINT TITRES BY DIAGNOSTIC GROUPING
The FANA titres in the different diagnostic groups (rheumatic, non-rheumatic, and SLE/MCTD/overlap) are shown in table 1. The relatively low numbers of subjects with FANA positivity of 1:20 is probably due to the fact that for the last few months of the study subjects who would have been positive at a titre of 1:20 were negative because they were screened at an initial dilution of 1:40.
FANA titres by disease category
Forty one subjects had a diagnosis of either SLE, MCTD, or overlap syndrome. Thirty six had SLE. Four had MCTD and all had FANA titres of 1:1280, one had an overlap syndrome with a FANA titre of 1:160. Only two of the 41 subjects were not known to the authors. Three other subjects not listed in table 1 as having SLE were diagnosed by their physicians as possibly having SLE (FANA titres of negative, 1:40, and 1:320 respectively). They did not fulfil classification criteria for SLE.
FANA TITRES BY GENDER
More girls (59%) were tested for antinuclear antibodies than boys (41%). There were significantly more girls (66%) in the known diagnosis group than in the unknown diagnosis group (p=0.0001).This is probably due to the fact that whereas children seen by the paediatric rheumatology service comprised only 15% of all subjects tested, they comprised 29% of the group with a known diagnosis, and therefore the known diagnosis group is weighted towards individuals with musculoskeletal complaints, who are more frequently girls.
Irrespective of diagnosis group the proportion of girls to boys increases as the FANA titre increases (p=0.05) (table 2), suggesting that female sex, independent of diagnostic group, is a risk factor for antinuclear antibodies production. As some patients with non-rheumatic disease may have an autoimmune disease (children with diabetes mellitus, thyroiditis, chronic active hepatitis, etc) we compared children with possible autoimmune, non-rheumatic with children with non-autoimmune, non-rheumatic disease. The frequency of FANA positivity did not differ between the groups (data not shown), again suggesting that antinuclear antibodies production is correlated with female sex independent of disease category.
Relationship of FANA titre to gender by diagnosis; values are boys: girls (% girls)
Test characteristics of FANA as screening test for rheumatic diseases (boys and girls combined)
TEST CHARACTERISTICS
Based on the results from the 699 subjects with a known diagnosis, the test characteristics, using different cut off levels for a positive test for a rheumatic disease, or for SLE/MCTD/overlap are shown in tables 3-5. It can be seen that the test for rheumatic disease at low cut off titres has both poor sensitivity and specificity, with low positive and negative predictive values even at high titres. For SLE/MCTD, at low cut off titres the test has a high sensitivity and high negative predictive value, but the specificity and positive predictive value is very low; at high titres although the specificity and negative predictive values are high, the sensitivity and positive predictive values are low. The test characteristics being somewhat worse for girls (table 4) than for boys (table 5). In other words a negative test virtually rules out the diagnosis of SLE/MCTD but low titres occur commonly in children who have no evidence of an inflammatory rheumatic disorder. Also, even though the great majority of children with SLE/MCTD have titres of 1:160 or higher, these levels are found as commonly in children who do not have a rheumatic disease, with only titres of 1:1280 or greater being associated with a higher frequency of rheumatic disease relative to non-rheumatic disease.
Test characteristics of FANA as screening test for SLE/MCTD/overlap syndrome (girls)
Test characteristics of FANA as screening test for SLE/MCTD/overlap syndrome (boys)
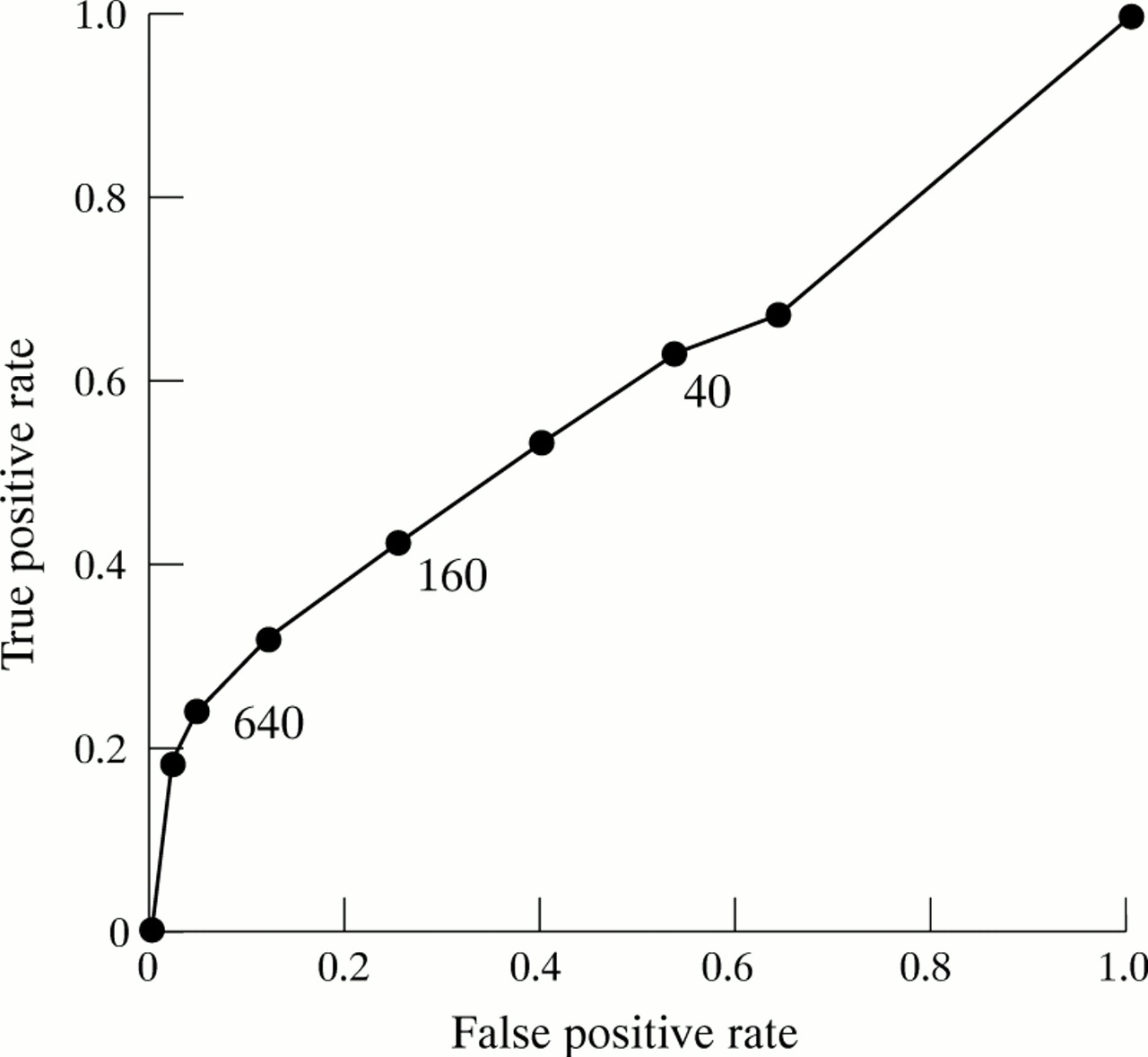
The ROC curves for the FANA test as a screening test for rheumatic disease, and for SLE/MCTD/overlap syndrome, are shown in figs 1-3. The larger the area under the curve (that is, the squarer it is towards the coordinates x=0, y=1) the better the test discriminates. It can be seen that the test is extremely poor for discriminating rheumatic from non-rheumatic disease. There is no difference between boys and girls (data not shown). For SLE/MCTD, a titre somewhere between 1:160 and 1:320 appears to be the titre with the most ‘efficient’ screening characteristics, having the best combination of high sensitivity and high specificity. There is a significantly larger area under the curve for boys compared with girls (p=0.001), suggesting that the FANA is somewhat better for diagnosing SLE/MCTD in boys than girls.
PHYSICIAN PERCEPTION OF ROLE OF FANA TESTING
Forty two physicians responded to the questions about the usefulness of FANA testing to diagnose or to exclude SLE as a diagnosis. The answers indicated some major differences in opinion about the value of the test. The majority of respondents felt that the FANA was useful in the exclusion of SLE as a diagnosis, with 16 physicians stating that the test was useful to both diagnose and to exclude SLE, 11 stating that the test was useful to exclude the diagnosis of SLE but were unsure of the test’s value to diagnose SLE, and six stating that the test was useful to exclude, but not useful to diagnose SLE. Three physicians felt that the test was useful to diagnose but not useful to exclude SLE, and rather surprisingly (given that they had ordered the test) six physicians felt that the test was neither useful to exclude nor to diagnose SLE.
Discussion
The FANA test has become a standard test in the work up of children for possible rheumatic diseases. However the evidence for the usefulness of the test to either diagnose or to exclude the diagnosis of a rheumatic disease, in particular SLE, is rather limited. Some justification for the use of the test was provided by a study by Chudwin et al.9 They stated that most children with a positive FANA test had ‘readily diagnosable autoimmune disorders’. However this conclusion was based on 138 children with a positive FANA test out of a total of 1442 patients who had been referred to a specialist paediatric immunology/rheumatology clinic at the University of California. Therefore referral bias would certainly influence their findings. Even despite this bias one third of the FANA positive patients did not have a definite autoimmune disease. It is of note that the FANA positive rate in their immunology/rheumatic disease population of 9.5% is much lower than our study result of 41%. The reason for this may in part be due to the fact that in their study the FANA was performed on a rat kidney substrate rather than on a HEp-2 cell substrate as in our study. The frequency of FANA positivity in normal childhood sera (from children undergoing plastic surgery), has been reported by Arroyave et al.10 In their study more children were positive using HEp-2 cells as substrate than using mouse kidney substrate at each dilution tested, with only 0.4% positive at a screening dilution of 1:20 using mouse kidney substrate compared with 0.8% positive using Hep-2 cells at the same dilution.
Perhaps the study that most closely resembles our own is a study from Albania reported in 1992 by Sulcebe and Morcka.11 This study reported on the results of sera tested for antinuclear antibodies using a rat liver substrate and a screening serum dilution of 1:10. Sera were sent to the Immunology Laboratory of Tirana. Although most sera were from adult patients, the range of patients who were tested would seem to be somewhat similar to ours in that the sera were from patients seen at outpatient clinics, and rheumatic and internal medicine hospital divisions from all of Albania, as the laboratory is the only centre for antinuclear antibody testing in the entire country. Although the data were not reported in this form, based on their figures it would appear that about 26% of all sera tested were positive for antinuclear antibodies. If a Hep-2 cell substrate had been used the positivity rate would perhaps have been even higher.
Another study that is similar to ours, but which has only been published in abstract, is that of Slater and Shmerling.12In this study of adult patients from a teaching hospital, Beth Israel Hospital in Boston, 157 (16%) of 994 patients on whom a FANA test was performed using a HEp-2 cell substrate, were positive at a titre of at least 1:40. Only 16 of those were diagnosed with SLE, and only another 31 patients were diagnosed with other rheumatic diseases. The authors calculated a positive predictive value for rheumatic disease of only 30%, and for SLE of only 10%. Among the 16 patients with FANA titres of ⩾1:640, five (31%) had no rheumatic disease, and only six (38%) had SLE.
The frequency of FANA positivity in our study is nevertheless disconcertingly high. Several possibilities need to be considered to explain this. Firstly our population studied is rather heavily weighted towards children with rheumatic disease with 15% of the tests being ordered by the paediatric rheumatology service. However this cannot explain the high frequency, as 37% of tests ordered by physicians other than the paediatric rheumatologists were also FANA positive. Secondly it is possible that the test kits used by our laboratory were unusually sensitive. There is some evidence from our study that there are indeed differences in sensitivities between kits. During the period of time in which kits were provided by Kallestad Diagnostics the FANA positivity rate was 36%, whereas during the time the kits were from Helix Diagnostics the positivity rate was 47%, with a similar distribution between rheumatic and non-rheumatic disease groups, despite the initial screening dilution being raised to 1:40 for the latter part of this period. It is therefore possible that kits provided by other manufacturers might be less sensitive; however it seems unlikely that this would lower the positive rate very dramatically. A third possibility is that the haematopathology laboratory at British Columbia’s Children’s Hospital is unable to adequately interpret the FANA test. As this laboratory is accredited by the Diagnostic Accreditation Program of the Province of British Columbia, is at a tertiary care institution, and provides all the FANA testing for children as well as for adult patients from the British Columbia Women’s Hospital, this possibility seems extremely highly unlikely. In fact given the large number of tests performed a year, it is probable that our laboratory is more able to interpret tests accurately than many other smaller laboratories, who receive requests for many fewer tests per year.
This study could be criticised on the grounds that we have underestimated the number of children with SLE, because we have failed to obtain diagnoses for many of the subjects with negative or low titre positive FANA test results, and because some of the subjects who at present do not have a diagnosis of SLE might develop the disease if followed up for a longer period of time. We think this is unlikely for a number of reasons. Given the low incidence of childhood SLE,13 it is improbable that more than one or two children tested could develop the disease in the foreseeable future. We and others have shown that the vast majority of children who have positive FANA tests, but who do not have autoimmune conditions at initial diagnosis, will not develop an autoimmune disease later.5 6 Although it is possible that some children tested, on whom we do not have a diagnosis, could have SLE, this is unlikely; of all 36 children with SLE only two (who had FANA titres of 1:160 and 1:1280 respectively), were not known to us. We also randomly analysed the charts of 211 subjects who were FANA positive, but not diagnosed as having SLE or MCTD, to determine the number of American College of Rheumatology SLE classification criteria exhibited by each subject. The majority 131 (62%) had only one criterion (antinuclear antibody positivity), 76 (36%) had two criteria, and only four subjects had three criteria. For all these reasons, it seems unlikely that more than one or two subjects at most might develop SLE over the next few years, and improbable that we have missed subjects already known to have SLE. Almost certainly if we had a diagnosis on all subjects, the FANA test would have a slightly higher specificity but an even lower positive predictive value, for a rheumatic disease, for low titre positive results.
In conclusion the findings from this study indicate that a negative FANA test makes the diagnosis of SLE or MCTD extremely unlikely. However a positive test even at high titre is only a poor predictor of SLE or MCTD. Based on the test characteristics as demonstrated by the ROC curves, we would suggest that it would be reasonable to set the initial screening dilution for the FANA test at 1:160. At this titre there would be many fewer positive test results, without a significant increase in missed cases of SLE or MCTD. This would reduce parental and physician anxiety about whether or not the child might have a significant rheumatic disease. It would also have significant cost savings, due to a decrease in the number of sera that would have to be titred to endpoint, and due to a reduction in the number of extra tests such as anti-DNA antibodies and anti-ENA antibodies that would be ordered because of a positive test. Whether it would be more effective to abandon the FANA test, and only offer a test for anti-DNA antibodies cannot be answered by this report, but should be the focus of further study.
Acknowledgments
Study funded in part by a grant from The Children’s Program Endowment Fund of the Arthritis Society (BC and Yukon Division).
References

ROC curve for FANA as screening test for rheumatic diseases (boys and girls combined).

ROC curve for FANA as screening test for SLE/MCTD/overlap syndrome (girls).

{kind=link}
{kind=link}
{kind=link}
ROC curve for FANA as screening test for SLE/MCTD/overlap syndrome (boys).