Article Text

Abstract
The relation between month of birth, sensitisation, and manifestations of atopy was assessed in 209 children who were followed from birth to 12–15 years. Children born during the tree pollen season were less likely to develop allergic rhinoconjunctivitis, IgE antibodies to pollen, or a positive screening test for IgE antibodies (odds ratio 0.28, 0.41, 0.35, respectively) than children born during the rest of the year. The prevalence of IgE antibodies to food and animal dander at 9 months and to atopic disease was higher in children born in the autumn and winter, that is, September to February, compared to the spring and summer (egg 20% v 6%; milk 10% v 2%). Thus sensitisation to pollen and allergic rhinoconjunctivitis is least common in children born in the spring, while birth in September to February is associated with an increased incidence of sensitisation to food and of atopic disease.
- hypersensitivity
- seasonal effect of birth
Statistics from Altmetric.com
Early infancy seems to be a period of particular susceptibility to sensitisation, as indicated by epidemiological1 2 and experimental studies.3 For example, the season of birth may affect the future development of allergy,1 2 4-12particularly in children with a propensity to atopic manifestations.7
We have previously reported the temporal relation between the appearances of IgE antibodies in serum and atopic disease in a prospective study of 324 children, most of whom were followed up from birth up to 12–15 years of age.13 Our aims in this study were to analyse the relation between the month of birth and sensitisation to inhalant allergens, as well as the appearance of atopic manifestations, during childhood.
Methods
STUDY GROUPS
Two groups of children were studied prospectively from birth up to 12 and 15 years of age, respectively.13
Group I comprised 125 children, 66 boys and 59 girls, born in Linköping between August 1972 and March 1974. They were followed up from birth up to 15 years of age. A history of atopic disease was present among two members of the immediate family (that is, parents or siblings) in 52 of them, while 38 children had one atopic family member and 35 children had no immediate family history of atopy. Clinical examinations were conducted by one of us (MK) four times during the first 18 months of life and on six occasions between 18 months and 15 years of age. Selected results from the first years of life have been published previously.14-16
Group II consisted of 84 girls born between August 1977 and August 1978 at the Central Hospital in Skövde. They had a random heredity for allergy and they were followed prospectively for 12 years. This group was originally recruited to a study of Rh immunisation17but was also subject to an extensive follow up with regard to the appearance of allergic disease and IgE antibodies.18-20
Among the 209 children in the two study groups, 58 had a double, 66 a single, and 85 no family history of atopic disease. Blood was drawn at 9 and 21 months, and at 4.5, 6.5, 9, and 12 or 15 years of age.
DIAGNOSTIC CRITERIA
Atopy was defined as the presence of circulating IgE antibodies against an allergen or the presence of atopic disease, or both.
The diagnosis of atopic dermatitis was based on the definition of Hanifin and Rajka, that is, a pruritic, chronic, or chronically relapsing dermatitis with typical morphology and distribution.21 Bronchial asthma was defined as three or more episodes of bronchial obstruction as verified by a physician at least once. Allergic rhinoconjunctivitis was defined as rhinitis and conjunctivitis appearing at least twice after exposure to a particular allergen and not related to infection. Urticaria was defined as allergic if appearing on at least two occasions within one hour after exposure to a particular allergen. Gastrointestinal allergy was defined as the appearance of diarrhoea, colicky pains, and/or vomiting after intake of a specific food on at least two occasions.
The clinical observations were made in two hospitals by two of us (MK, GH) over a long period. Therefore three of the investigators (MK, LN, NS) jointly scrutinised the diagnoses by studying case histories of patients selected at random from the two groups. This retrospective control of the diagnoses agreed well with the initial classification, as there were only minimal differences in opinion.
LABORATORY METHODS
All serum samples were kept at −20°C until analysed. In all, 6274 IgE antibody determinations were done on 1079 blood samples, employing Pharmacia CAP system (Pharmacia Diagnostics, Uppsala, Sweden (n = 4351) or the Phadebas RAST (Pharmacia) (n = 1923) for the detection of IgE antibodies against defined allergens, and a multiallergen test, the Phadiatop Paediatric (Pharmacia) test (n = 1079). The same laboratory technician performed all the analyses. Serum samples in group I were analysed with the CAP system, and in group II employing RAST. Values of 0.35 kU/l and 0.35 PRU/ml, corresponding to CAP/RAST class 1, respectively, were considered to be positive. The same allergen source was used for CAP and RAST and the results correlate closely with each other.22
Serum samples from children aged 18 months and older were analysed for IgE antibodies against animal dander, birch pollen, house dust mite (Dermatophagoides pteronyssinus), and wheat (in order of priority). Antibodies against timothy grass were included from age 4. For the detection of IgE antibodies to animal dander, group I serum samples were analysed with cat, dog, and horse allergens and the group II serum samples were analysed with an animal mix containing allergens from cat, dog, and horse (Pharmacia).
An analysis of IgE antibodies to egg white and cows’ milk was done in all children up to 18 months of age and had a higher priority than the determination of antibodies to inhalant allergens and wheat up to that age. Serum samples from children older than 18 months were analysed for IgE antibodies against egg white or cows’ milk only if antibodies had been detected against these foods in the previous sample.
STATISTICAL ANALYSIS
The χ2 test (with Yates’s correction when n < 100) was employed for categorical variables, and the Fisher’s exact test was used when the expected frequency for any cell was less than 5. Multiple logistic regression analysis was employed when assessing the combined predictive value of several indicators of future atopic manifestations.
ETHICS
The parents of all participating children gave their informed consent. The studies were approved by the human research ethics committees of the medical faculties at the Universities of Linköping and Göteborg.
Results
Atopic disease appeared in 105/209 children (50%) during the follow up period. Atopic dermatitis was the most common manifestation (72/209, 34%), followed by allergic rhinoconjunctivitis (54/209, 26%), food allergy/urticaria (33/209, 16%), and bronchial asthma (25/209, 12%).
Atopic disease was more common among children who were born in the autumn and winter compared to the spring and summer (table 1), independent of the family history of allergy. This was particularly obvious early in life. Thus the risk was about threefold at 9 months (p < 0.001).
Estimated probabilities of atopic disease at various ages in relation to season of birth and family history of atopic disease
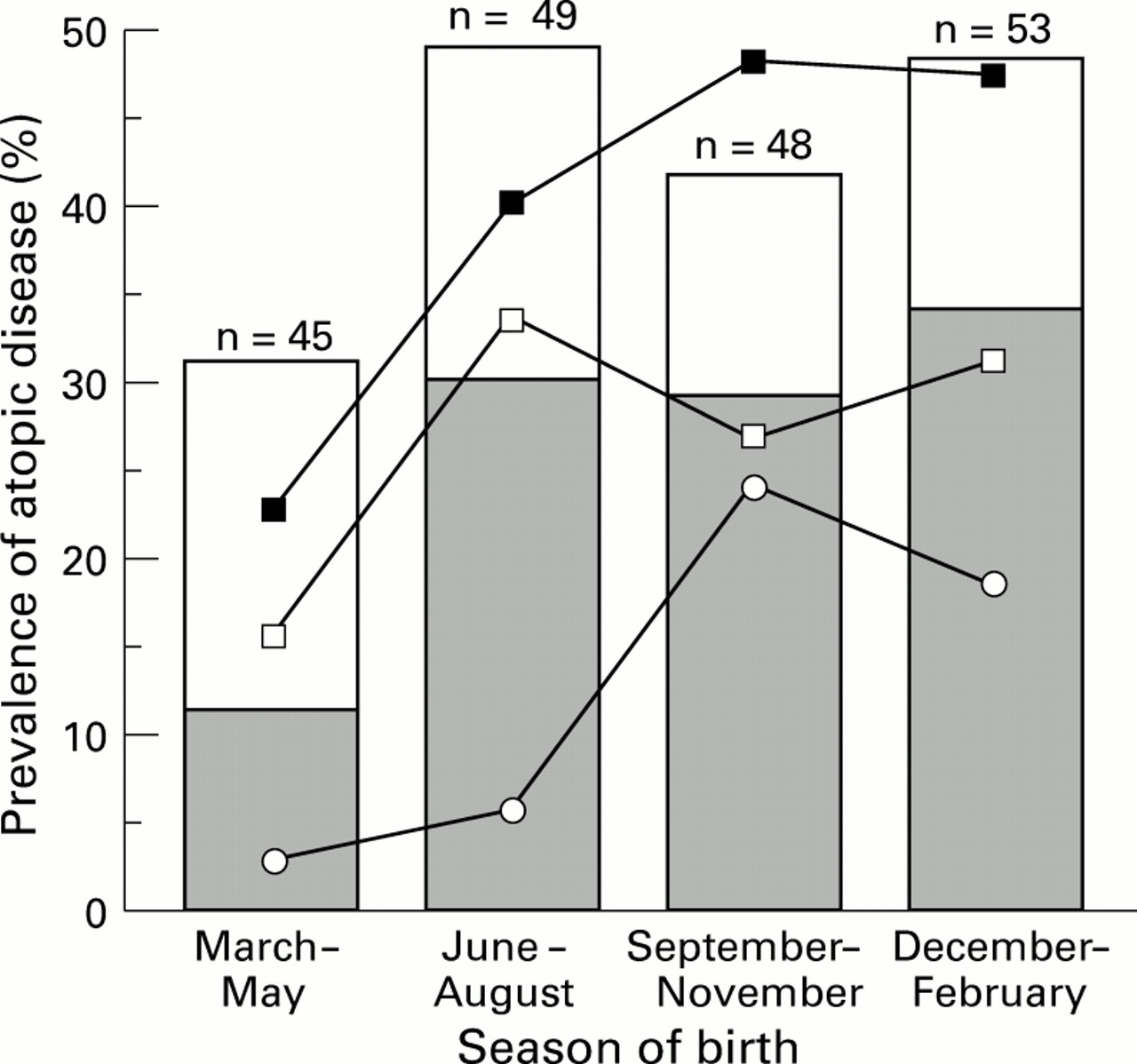
The prevalence of allergic rhinoconjunctivitis was 11% at 12 to 15 years of age among children who were born between March and May, as compared to a rate of 29-34% among children born during any of the other seasons (p = 0.008, fig 1). A positive multiallergen test was also less common at all ages among children born between March and May (fig 2) (p = 0.01 to 0.05, compared to the other seasons). The seasonal influence was even more obvious in children who were born between April and June, compared to the other seasons. Thus the prevalence rate of allergic rhinoconjunctivitis was 0/40 and 18/159 (11%) respectively at 4.5 years (p = 0.03), 1/39 (3%) and 24/163 (15%) at 6.5 years (p = 0.05), and 3/39 (8%) and 49/157 (31%) at 12-15 years of age (p = 0.003).

Prevalence (%) of any atopic disease at 12–15 years of age (whole columns) and allergic rhinoconjunctivitis (shaded columns), and presence of circulating IgE antibodies against a mixture of allergens (filled squares), pollen (empty squares), and egg white (empty circles) in relation to season of birth in 209 children. Levels of statistical significance for differences in prevalence between children born between March and May as compared to the other months of the year: atopic disease NS (p = 0.06); allergic rhinoconjunctivitis p = 0.008; multiallergen test, p = 0.006; pollen, p = 0.04; egg white, p = 0.05.

{kind=link}
{kind=link}
Period prevalence of sensitisation (Sens), as judged by a positive multiallergen test in relation to season of birth and period prevalence of allergic rhinoconjunctivitis (ARC) in 209 children who were followed up prospectively for 12 to 15 years. The p values refer to comparisons of the prevalence of sensitisation and atopic manifestations in children born during March to May compared to other times of the year. Black columns and circles denote infants born March to May, white symbols infants born June to August, dark grey columns and squares: infants born September to November, and light grey columns and triangles: infants born December to February.
Immunoglobulin E antibodies to egg white, milk and wheat were more often encountered in children who were born between September and February, compared to those born between March and August, (for egg, p < 0.001 and for milk, p = 0.01) and they more often had atopic dermatitis (p = 0.04). Sensitivity to egg white was particularly common in children who were born in October and November as compared to the rest of the year, p = 0.005). Similarly, 17/152 children (11%) with IgE antibodies against animal dander at 4.5 years were born between September and February, as compared to 5/137 children (4%) born during the other six month period (p = 0.02).
Discussion
The size of the study groups allowed us to detect an association between manifestations of atopy and season of birth. Thus we found an increased sensitisation rate to egg white and milk and a higher prevalence of atopic disease among children who were born between September and February. The study was not intended to be epidemiological, as children with a family history of allergy were greatly over-represented and the children were not randomised for the comparisons. The children included in the study were those whose parents had, at the time of the birth, an interest in having their child followed up in this prospective study. Hence children included in the study were born throughout all seasons.
Increased sensitisation to egg white among children born in the winter has previously been observed in a Dutch study4 and by us in another cohort of children.8 In the retrospective Dutch study including 78 000 blood samples obtained from children for clinical reasons, the highest prevalence of IgE antibodies to egg white was recorded in patients who were born in September to February. In our recent prospective study,8 the increased risk was limited to children born between October and December. Reasons for this increased risk among children born in late autumn and winter remain unexplained.
Several previous studies have indicated that children born in the months before the pollen season more often develop sensitivity to pollen and allergic rhinoconjunctivitis than children born during the pollen season6 9-11 although this was not always the case.23 In the large Finnish study by Björksténet al the highest risk for sensitivity to birch was seen among children born in the months preceding the pollen season.6 Similarly, the highest prevalence of sensitisation to mugwort was seen in children born in April and May, that is, some months before the mugwort pollen season, and the lowest prevalence was seen among children born in July and August.6 An explanation for this seasonality could be that mothers develop IgG antibodies to pollen during the pollen season which would suppress sensitisation, as indicated by experiments in rats.24 This possibility is supported by a very recent observation that the IgG antibody levels to the major birch antigenBet v1 in cord blood tended to be lower in babies who were born to atopic mothers outside the pollen season (MC Jenmalm et al, unpublished data). The seasonality of pollen sensitisation seems to be more evident in countries with a cold climate.25 Possibly, seasonal differences are not observed in countries where the major allergens are perennial.
The relation between season of birth and the development of allergy to seasonal allergens is further complicated by a Finnish study suggesting that weaning during the birch or grass pollen seasons was associated with a reduced risk for later development of allergic manifestations.26
In conclusion, infants born in the autumn and winter more often had IgE antibodies to egg white, milk, and wheat than children born in the spring and summer, and they more often developed atopic disease. In contrast, sensitisation to inhalant pollens and allergic rhinoconjunctivitis were less common in children born in the spring as compared to the other seasons. The phenotypic expression is influenced by genetic factors, maternal immunity (through the placenta and breast milk), time and dose of exposure, and adjuvant factors. The main reason for the seasonal effects found in this study remain to be clarified.
Acknowledgments
The study was supported by grants from the National Association for the Prevention of Asthma and Allergy (RmA), the Swedish Medical Research Council (No 7510) and Faculty of Health Sciences, University of Linköping. The IgE analyses were supported by grants from Pharmacia Diagnostics, Uppsala, Sweden.