Article Text

Abstract
Aims: To assess prevalence of the insulin resistance syndrome (IRS: obesity, abnormal glucose homoeostasis, dyslipidaemia, and hypertension) in obese UK children and adolescents of different ethnicities and to assess whether fasting data is sufficient to identify IRS in childhood obesity.
Methods: A total of 103 obese (BMI >95th centile) children and adolescents 2–18 years of age referred for assessment underwent an oral glucose tolerance test, measurement of fasting lipids, and blood pressure determination. Main outcome measures were prevalence of components of IRS by modified WHO criteria, with IRS defined as ⩾3 components (including obesity).
Results: There were 67 girls (65%). BMI z-score ranged from 1.65 to 6.15, with 72% having a z-score ⩾3.0. Abnormal glucose homoeostasis was identified in 46% (hyperinsulinism in 40%, impaired fasting glucose in 0.8%, impaired glucose tolerance in 11%). No subjects had silent type 2 diabetes. Dyslipidaemia was identified in 30% and hypertension in 32%. Thirty one per cent had obesity alone, 36% had two components, 28% had three, and 5% had all four components. Birth weight, BMI, and family history of IRS were not associated with risk of IRS. Higher age increased the risk of IRS; however the syndrome was seen in 30% of children under 12 years. The use of fasting glucose and insulin data for identifying IRS had a sensitivity of 88% and specificity of 100%.
Conclusions: One third of obese children and adolescents have the IRS; however type 2 diabetes is rare. Obese children with the IRS may form a high risk group to whom scarce intervention resources should be targeted. Further work is needed to develop appropriate screening programmes for IRS components in significantly obese children.
- BMI, body mass index
- IRS, insulin resistance syndrome
- OGTT, oral glucose tolerance test
- cardiovascular risk
- insulin resistance syndrome
- metabolic syndrome
- obesity
- type 2 diabetes
Statistics from Altmetric.com
Obesity in childhood and adolescence has been shown to increase the risk of the insulin resistance syndrome (IRS)1 and cardiovascular mortality in adult life.2 The clustering of major IRS components, including obesity, hypertension, dyslipidaemia, and atherosclerosis, has been shown in children and adolescents3,4 and tracks strongly into adult life.5 This tracking has been shown to increase with increasing age and obesity.5 Many studies have shown that individual IRS components such as insulin resistance, dyslipidaemia, and hypertension are highly inter-correlated and significantly more common in obese children than in those of normal weight.6–9 However the prevalence of IRS in obese children and adolescents has been poorly documented. Epidemiological data from the USA suggest that the clustering of obesity with two or more of hyperinsulinaemia, dyslipidaemia, and hypertension is seen in 20% of obese children and adolescents.8 However, this data is drawn from a historical cohort of US white and black children, did not use modern more restrictive definitions of obesity,10 and did not use a standardised definition of IRS (for example, the WHO definition).11 The prevalence of the syndrome in contemporary obese UK children of different ethnicities is not documented.
Identification of obese children with additional IRS components may define a high risk group within the obese child population. There is little consensus on which obese children require treatment, as available guidelines focus on assessment in primary care12 and there are no accepted definitions of extreme or morbid obesity in childhood. Given the scale of the problem, the paucity of effective interventions,13 and the lack of available clinical resources, there is an urgent need to identify high risk groups who require treatment within the obese child population. Additionally, little guidance is available for clinicians on the appropriate investigations required for children and adolescents with obesity. Guidance has been published on screening for lipids and blood pressure,14 but with little information available on screening for glucose and insulin abnormalities, particularly as to whether fasting samples alone or an oral glucose tolerance test (OGTT) are required to identify abnormal glucose homoeostasis. In adults, there is increasing evidence that measurements of fasting glucose do not pick up many subjects with impaired glucose tolerance,15 particularly in certain ethnicities.16
We assessed the prevalence of the major components of IRS in a clinical sample of obese UK children and adolescents of different ethnicities using two definitions of obesity. We then examined whether demographic, clinical, and laboratory factors were associated with increased risk of IRS. Finally we explored whether fasting insulin and glucose are sufficient to screen for abnormalities in glucose homoeostasis in childhood obesity.
METHODS
Subjects were children and adolescents 2–18 years of age who underwent assessment of obesity in our joint paediatric and adolescent endocrine service between 1999 and 2002. Subjects were referred by their GP or local paediatrician for medical assessment of obesity. Subjects assessed prior to June 2002 were identified through a retrospective examination of hospital records. Subjects from July 2002 onwards had data collected prospectively. Only those who had had secondary or known genetic causes of obesity excluded were included in this analysis. Obesity was defined in two ways: firstly, as body mass index (BMI) ⩾95th centile for age and sex according to the UK 1990 growth reference;17 secondly, we defined extreme obesity as BMI z score ⩾3.0 (⩾99.86th centile) as there are no standard definitions of extreme obesity in childhood.
Subjects were assessed after a 12 hour overnight fast. Subjects underwent an OGTT (1.75 mg glucose/kg) with plasma insulin and blood glucose concentrations measured at 0, 30, 60, and 120 minutes. Plasma insulin was estimated by the Abbott AxSYM method. Fasting serum lipid concentrations (total cholesterol and triglycerides) were measured. Clinical policy meant that HDL cholesterol was measured in all adolescents but only in those children with abnormal total cholesterol or triglycerides. Blood pressure was measured in the recumbent position using an oscillometric method with an appropriate sized cuff for arm diameter. Data are reported as the average of two consecutive readings. Birth weight, ethnicity, pubertal status, presence of acanthosis nigricans, and family history of components of IRS were recorded or obtained from hospital records.
Abnormal glucose homoeostasis and IRS were defined following modified WHO criteria11 adapted for children (table 1). Hyperinsulinism was defined from norms for pubertal stage:18 prepubertal ⩾15 mU/l, mid-puberty (stages 2–4) ⩾30 mU/l. Post-pubertal hyperinsulinism was defined as per adult WHO criteria (⩾20 mU/l).11 Hypertension was defined as systolic blood pressure ⩾95th centile for age and sex.19 Abnormal fasting lipids were defined from normative data.20 IRS was defined as having three or more IRS components.11
Definition of components of the IRS11
Insulin sensitivity from fasting samples was estimated using the Homeostasis Model Assessment (HOMA-IR),21 the Quantitative Insulin Check Index (QUICKI index),22 and fasting insulin:glucose ratio (FIGR).23 HOMA-IR was calculated as fasting insulin (U/l) × fasting glucose (mmol/l)/22.5 (higher values indicate greater insulin resistance). QUICKI was calculated as 1/(log fasting insulin (U/l) + log fasting glucose (mg/dl)) (higher QUICKI values indicate greater insulin sensitivity). FIGR was calculated as fasting insulin (U/l)/fasting glucose (mg/dl). The homoeostasis model assessment was used to estimate pancreatic β cell function (HOMA-B%) and was calculated as 20 × fasting insulin (U/l)/(fasting glucose (mmol/l) − 3.5).21
Analysis
The χ2 test or ANOVA with Bonferroni post-hoc test were used to assess differences between groups where appropriate. The diagnostic yield of using only fasting insulin and glucose values compared to full OGTT data was examined by sensitivity analysis. Factors associated with risk of IRS were examined by logistic regression. Data were analysed using SPSS 10.
RESULTS
A total of 103 children and adolescents aged 2.3–18 years underwent assessment (36 males, 35%). Mean age was 11.9 years (SE 0.4) (males 12.9 (SE 0.6) years; females 11.2 (SE 0.5) years). BMI z-score ranged from 1.65 to 6.15 (mean 3.48), and all but five subjects had BMI z-score >2.35 (>99th centile). Seventy two per cent were extremely obese (BMI z-score ⩾3.0). There was no sex difference in mean BMI z-score or extreme obesity. Thirty nine (38%) were prepubertal, 27 (26%) were in mid-puberty (breast, genital stages 2–4), and 37 (36%) were post-pubertal. Acanthosis nigricans was noted in 45/82 subjects (55%). Data on ethnicity was available for 93 subjects (90%): white 54 (58%), black 8 (9%), south Asian 27 (29%), and other or mixed ethnicity 4 (4%). Fifty subjects (49%) reported a family history of any IRS component in the first or second generation. Mean birth weight was 3.51 kg (SD 0.82, range 1.45–5.56 kg).
Table 2 shows the prevalence of individual components of IRS by sex. Impaired fasting glucose was identified in only one subject (0.8%), impaired glucose tolerance in 11 (11%), and no subjects had silent diabetes. Hyperinsulinism was identified in 41 (40%) subjects. Overall, abnormal glucose homoeostasis was identified in 46 (45%) and was not associated with sex, ethnicity, or pubertal status. High total serum cholesterol concentrations were noted in 18 (18%), high serum triglyceride concentrations in 20%, and low HDL in 4 (10%) of the 40 (39%) subjects who had HDL measured. Overall, dyslipidaemia was identified in 31 (30%) with no significant differences by gender, pubertal status, or ethnicity. Mean systolic blood pressure z-score was 1.25 (SE 0.13; range –1.34 to 3.36). Hypertension was noted in 33 (32%) with no significant differences by sex or pubertal status. Hypertension was significantly more common in white young people (47%) than black (14%) or Asian (20%) young people (χ2 = 8.1, p < 0.05).
IRS components by sex
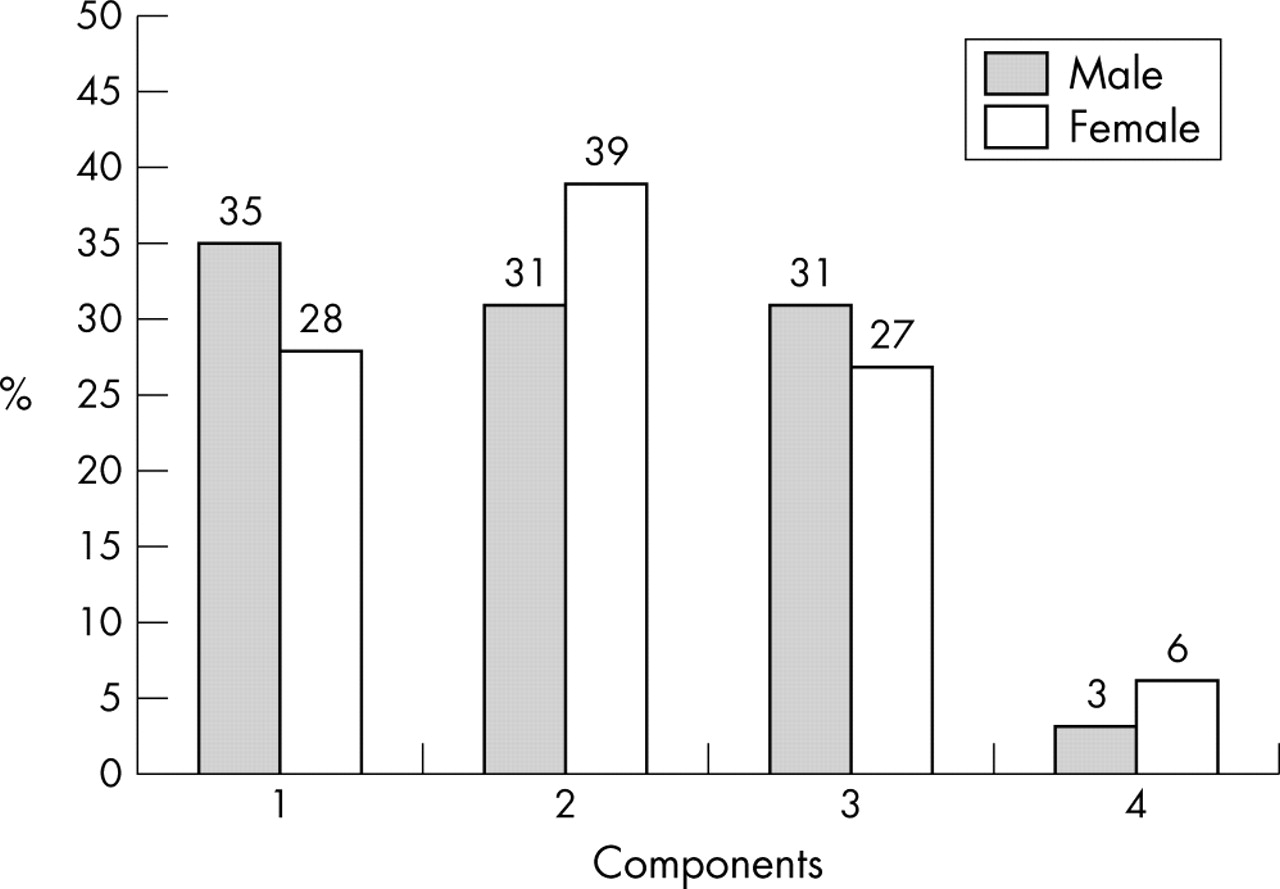
The prevalence of IRS components by sex using the definitions in table 1 is shown in fig 1. Thirty two subjects (31%) had obesity alone (one component). Two components were identified in 37 (36%), three components in 29 (28%), and all four components in five (5%). IRS, defined as ⩾3 components, was found in 34 (33%), with a non-significantly higher rate among adolescents aged 12–18 years (36%) than among children aged 2–11 years (30%). There were no significant differences in the prevalence of IRS by sex or pubertal status. There was a trend for IRS to be more common among white (37%) than black (13%) or Asian (22%) young people (χ2 = 6.6, p = 0.08). While IRS was slightly more common among the extremely obese (35%) compared with the simply obese (28%) (z-score <3.0), this difference was not significant.

{kind=link}
Number of IRS components by sex (including obesity).
Logistic regression showed that the only clinical or demographic factor associated with risk of IRS was higher age (OR controlled for pubertal status 1.13, p = 0.04, 95% CI 1.09 to 2.60). Birth weight, BMI and BMI z-score, the presence of acanthosis nigricans, and family history of IRS were not associated with risk of IRS.
We assessed the usefulness of fasting insulin and glucose values for assessing IRS by comparing the prevalence of IRS using only fasting information to define abnormal glucose homoeostasis (either fasting hyperinsulinaemia or impaired fasting glucose) with the prevalence previously derived from full OGTT data. Using the fasting definition, 33 (32%) had one component, 40 (39%) two components, 25 (24%) three components, and five (5%) had all four components. The prevalence of the full syndrome (⩾3 components) was 29% using this “fasting” definition.
Table 3 shows the diagnostic power of using only fasting insulin and glucose for IRS. Sensitivity analysis for the relations between the fasting definition of IRS and the OGTT definition (taken as “actual disease”) showed the following: specificity, 69/69 = 100%; sensitivity, 30/34 = 88%; positive predictive value, 30/30 = 100%; negative predictive value, 69/73 = 95%.
Diagnostic power of fasting compared with OGTT definitions of IRS
We further investigated whether using calculated fasting indices of insulin sensitivity or secretion improved the diagnostic yield of fasting samples, particularly in terms of identifying patients with impaired glucose tolerance but not either fasting hyperinsulinaemia or impaired fasting glucose. Of the 11 subjects with impaired glucose tolerance, four had normal fasting insulin and glucose and did not have abnormal glucose homoeostasis by the “fasting” definition. However the same four subjects also had values for HOMA-IR, HOMA-B%, FIGR, and QUICKI within 1 SD of means from normal weight children.24 In multivariate analysis controlling for age, sex, and pubertal status, fasting glucose, insulin, HOMA-IR, QUICKI, and FIGR were not predictive of impaired glucose tolerance.
DISCUSSION
We found 33% of obese children and adolescents of different ethnicities to have evidence of IRS as defined by ⩾3 of obesity, abnormal glucose homoeostasis, dyslipidaemia, and hypertension. A further third of our sample had one additional IRS component in addition to obesity. As epidemiological evidence suggests that the clustering of IRS components tracks strongly into adult life and greatly increases cardiovascular risk,5,25 these observations in children raise the possibility that obese children with two or more additional IRS components might form a high risk group within the obese child population.
In contrast to concerns about the rising incidence of type 2 diabetes in obese children and adolescents,26,27 we found that none of our obese children or adolescents of any ethnicity had silent type 2 diabetes. This finding is similar to that of a recent US report which found silent type 2 diabetes in only 3% of very obese subjects 4–18 years of age.28 We also found low rates of pre-diabetic glucose abnormalities, with 11% having impaired glucose tolerance and 1% having impaired fasting glucose. These rates are lower than estimates of impaired glucose tolerance in the aforementioned US clinical sample (20–25%)28 but higher than those from an Italian clinical sample (4.5%).6 It is likely that these differences reflect the differing clinical and ethnic populations studied. Our findings of a high prevalence of IRS but a low prevalence of glucose intolerance and type 2 diabetes reflect the range of abnormalities of glucose homoeostasis associated with obesity in childhood. While increasing obesity may over time unmask type 2 diabetes in those genetically predisposed to β cell failure, insulin insensitivity is the earlier and predominant abnormality of glucose homoeostasis found in obesity.29
One aim of this study was to identify factors that clinicians could use to guide decisions on the medical investigation of obese children. We were unable to identify clinical factors that identified obese children at greater risk of IRS. While age increased IRS risk, the youngest subject with IRS was 4.0 years and IRS was seen in 30% of children under 12 years, suggesting that age based cut-offs are not useful in identifying those who require investigation. The lack of relation between BMI (either raw or z-score) and IRS almost certainly reflects the constricted range of BMI among the subjects, but also suggests that that higher BMI thresholds (for example, z-score ⩾3.0) are not clinically useful in defining a high risk group. We were surprised that neither ethnicity nor family history of IRS were related to risk of IRS, particularly given evidence of heritability of IRS components30 and variation in insulin sensitivity between children of different ethnicities.31–33 This undoubtedly relates in part to the size of the sample studied but suggests that family and ethnic background cannot be used in clinical practice to select obese children and adolescents for further investigations.
Our findings relate to obesity defined as BMI ⩾95th centile; however, all but five subjects (5%) were obese by the more restrictive newer International Obesity Task Force definitions, which relate to an adult BMI ⩾30 kg/m2.10 Of these five subjects, three had one IRS component, one had two components, and one had all four components. There was no significant difference in the prevalence of IRS when obesity was defined by either BMI centile or the international definition.
We also studied which measurements of glucose and insulin were most useful in screening for abnormalities in glucose homoeostasis associated with IRS. Insulin and glucose data from the OGTT identified abnormalities in 45% of subjects. In contrast, measurement of fasting blood glucose alone would have identified only one subject (1%) and measurement of blood glucose alone during an OGTT would have identified only 12 subjects. Thus screening for abnormalities in glucose homoeostasis in obese children using blood glucose alone, either fasting or during an OGTT, is likely to have extremely low yield and measurements of insulin and glucose are needed to identify the most prevalent abnormalities in glucose homoeostasis. Identification of all the abnormalities in glucose homoeostasis requires the subject to undergo an OGTT measuring glucose and insulin, as fasting insulin and glucose are thought to predominantly reflect insulin secretion and hepatic insulin sensitivity, whereas data from the later stages of the OGTT are thought to reflect peripheral as well as hepatic insulin sensitivity.34,15 However, we found that in our sample of obese children and adolescents, the use of raw fasting insulin and glucose data alone had high specificity and an acceptable sensitivity of 88% in identifying subjects with IRS, with only 4% of subjects with the syndrome missed if fasting values alone were used. We did not find that indices of insulin sensitivity (HOMA-IR, QUICKI, FIGR) or secretion (HOMA-B%) calculated from fasting values were useful in predicting risk of IRS over and above the fasting values themselves.
Limitations of these data
Data from clinical samples may not be representative of the general population and selection and referral bias may have inflated our estimate of the prevalence of IRS. However, this was a regional referral sample representing a population of major concern to clinicians and included significant numbers of children from white, Asian, and black ethnicities. Additionally, no subjects had been referred because of previously identified abnormalities of glucose homoeostasis, and hypertension had been previously identified in less than 5% of the sample. Our modifications of the standard adult IRS criteria may have affected our results. Our definition of hyperinsulinism by pubertal status produced a more conservative estimate of IRS prevalence than using the standard adult definition (data not shown). We used high total cholesterol in addition to high triglycerides and low HDL to define dyslipidaemia, as evidence suggests that high total cholesterol remains the best marker for cardiovascular risk during childhood and adolescence.35
Conclusions
Clinical concerns over obesity in childhood and adolescence should focus on the presence of additional IRS components, including abnormalities of glucose homoeostasis, hypertension, and dyslipidaemia. We suggest that clinicians should consider screening all significantly obese children and adolescents regardless of age, ethnicity, or pubertal status for IRS. Fasting measures have acceptable sensitivity and specificity if fasting insulin is measured as well as glucose.
Those with three or more IRS components may form an appropriate group for intervention, which may include medical therapy for hyperinsulinaemia,36 dyslipidaemia, or hypertension as well as multidisciplinary weight control programmes. The value of such interventions needs to be assessed by formal clinical trials with long term follow up of outcome.
REFERENCES
Linked Articles
- Perspectives