Article Text

Abstract
Over the past 10 years there has been increasing evidence that particles generated by the combustion of fossil fuels adversely affect health. To what extent should paediatricians be concerned about particle pollution? This review assesses what we know, and what we still need to know about the health effects of fossil fuel particles.
- pollution
- PM10
- health effects
- AM, alveolar macrophage
- DEP, diesel exhaust particles
- PEF, peak expiratory flow
- PM, particulate matter
- TSP, total suspended particulate matter
- UF, ultrafine
Statistics from Altmetric.com
- AM, alveolar macrophage
- DEP, diesel exhaust particles
- PEF, peak expiratory flow
- PM, particulate matter
- TSP, total suspended particulate matter
- UF, ultrafine
Since the early 1990s there has been increasing evidence that particles generated by the combustion of fossil fuels adversely affect health. In January 2001, the UK government was sufficiently concerned to issue a warning when air pollution levels for particulates were forecast to be high across most of the UK.1 Hourly updates on particle levels across the country were, and still are available on the internet (www.environment.detr.gov.uk; accessed 1/12/01), or on a freephone number. The minister for the environment at the time, Michael Meacher, commented: “I have taken the precautionary step of making sure vulnerable people, such as those with heart and lung disease, are aware and can take appropriate measures to reduce their exposure”.1 Children were not specifically identified in this warning, but to what extent should paediatricians be concerned about particle pollution?
SOURCES OF PARTICLES
Polluted air is a complex mixture of vaporous, liquid, and solid components (fig 1). There are major qualitative and quantitative differences in this mixture, depending on emission sources, geographical location, weather conditions, time of day, and season. Irrespective of these variations, particles from internal combustion engines are a consistent contributor to the particle fraction of the pollutant mix. Although petrol engines emit particles, diesel engines, especially heavy duty engines, are a major emission source as they emit 100 times more particles than do petrol engines of corresponding performance. Diesel exhaust particles (DEP) are defined as “primary” particles—that is, they are emitted directly and are not formed in the atmosphere. DEP consist of a carbonaceous core (fig 2) onto which over 18 000 different high molecular weight compounds are adsorbed.2 DEP are regarded as the prototypic pollutant particle, but there are other types of particles, such as natural wind blown dusts, and sulphate from gas-to-particle interactions in the atmosphere (secondary particles). The health effects of the combustion of biofuels (wood, agricultural residues, and dung) are not discussed in this review, but they are a major source of particles in rural underdeveloped countries.

The air pollution mixture (adapted from Health Effects Institute42).
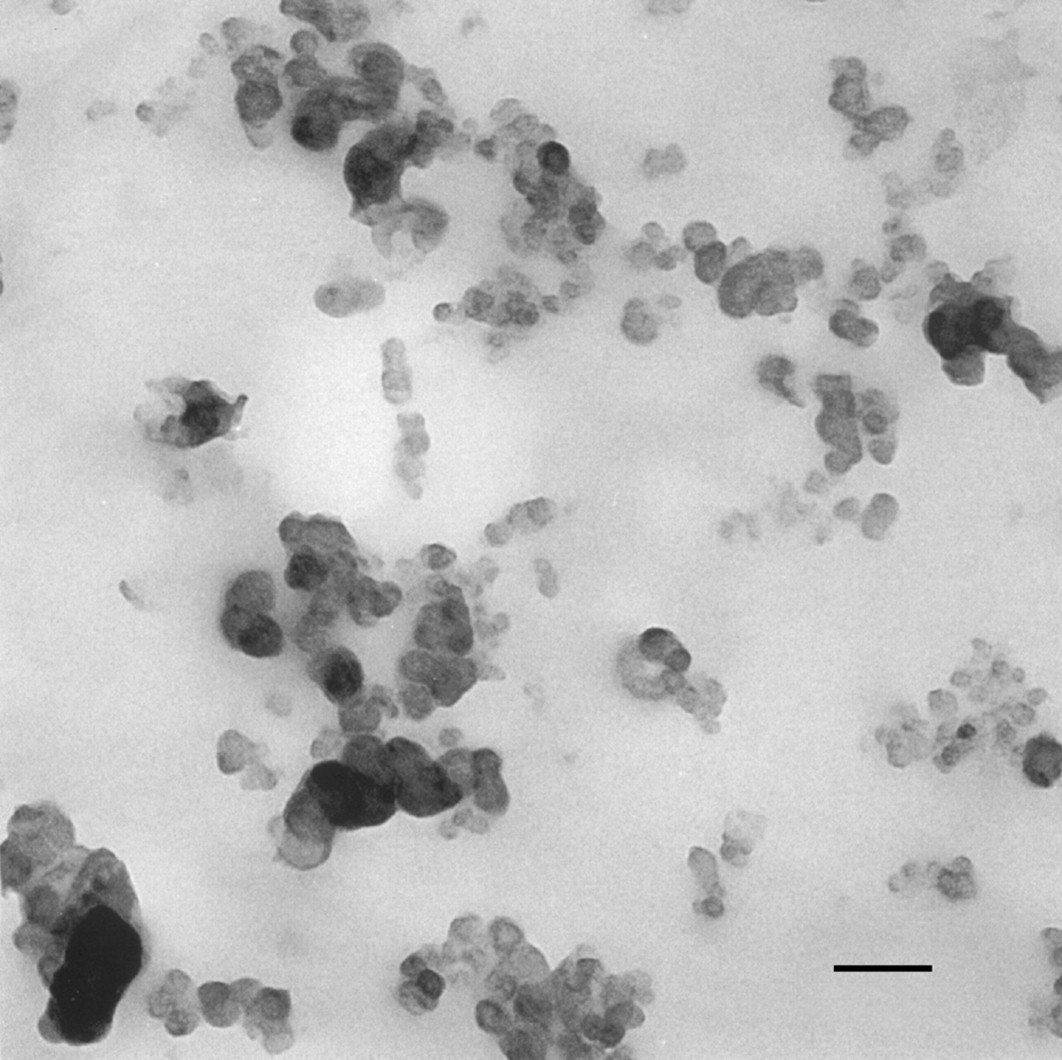
Diesel particles sampled from an exhaust pipe, and examined by electron microscopy. Single carbonaceous ultrafine particles and aggregates of ultrafine particles are present (scale bar 100 nm).
PARTICLE MEASUREMENT
Older monitoring devices for primary particles suck in a volume of air, and measure the total mass of suspended particles, irrespective of size. Current samplers determine the mass of particulate matter (PM) in diameters under 10 μm (PM10), and under 2.5 ℅ μm (fine particles, PM2.5). These measurements are more relevant to health effects as PM10 corresponds to the “inhalable” fraction, and PM2.5 is the size that is most likely to penetrate deepest into the airways. Another important component of PM10 in terms of number but not mass, are ultrafine (UF) particles of less than 0.1 μm in diameter3; 109 UF particles have the same mass as one “coarse” particle of 10 μm diameter, and readily penetrate into houses through walls.4 In general, the “naturally” generated particles such as wind blown soils fall into the coarse fraction of PM10 (less than 10 μm and greater than 2.5 μm), whereas fossil fuel combustion is the major source of smaller particles (PM2.5 and UF).5
TOXICITY AND PARTICLE SIZE
Although particle concentrations in ambient air may change in parallel to gaseous pollutants such as nitrogen dioxide, it is possible to identify the independent effect of PM10 in large studies.6 By contrast, there is a high degree of intercorrelation between the coarse, fine (0.1–2.5 μm), and UF particles, and it is difficult to pinpoint which fraction of PM10 is the most toxic. From a public health perspective this may not be a problem, as long as the emission source can be identified. However, vehicle manufacturers need to know the size and composition of the most toxic fraction. Reducing one particle size fraction by changing combustion conditions may paradoxically lead to an increase in the emission of another inhalable fraction. The more technologically advanced engines tend to emit more UF particles. For example, PM from turbocharged diesel engines contains a higher percentage of UF particles, and catalytic converters attached to petrol engines release a higher percentage of particles in the UF range.7 The studies that are most likely to address toxicity of specific size fractions are: time series analysis where small changes in the correlation between different size fractions can be exploited to find the best fit model for outcome (for example, daily lung function over a month), studies near industries that produce high levels of particles of uniform size, and laboratory inhalation experiments.
LEVELS OF EXPOSURE
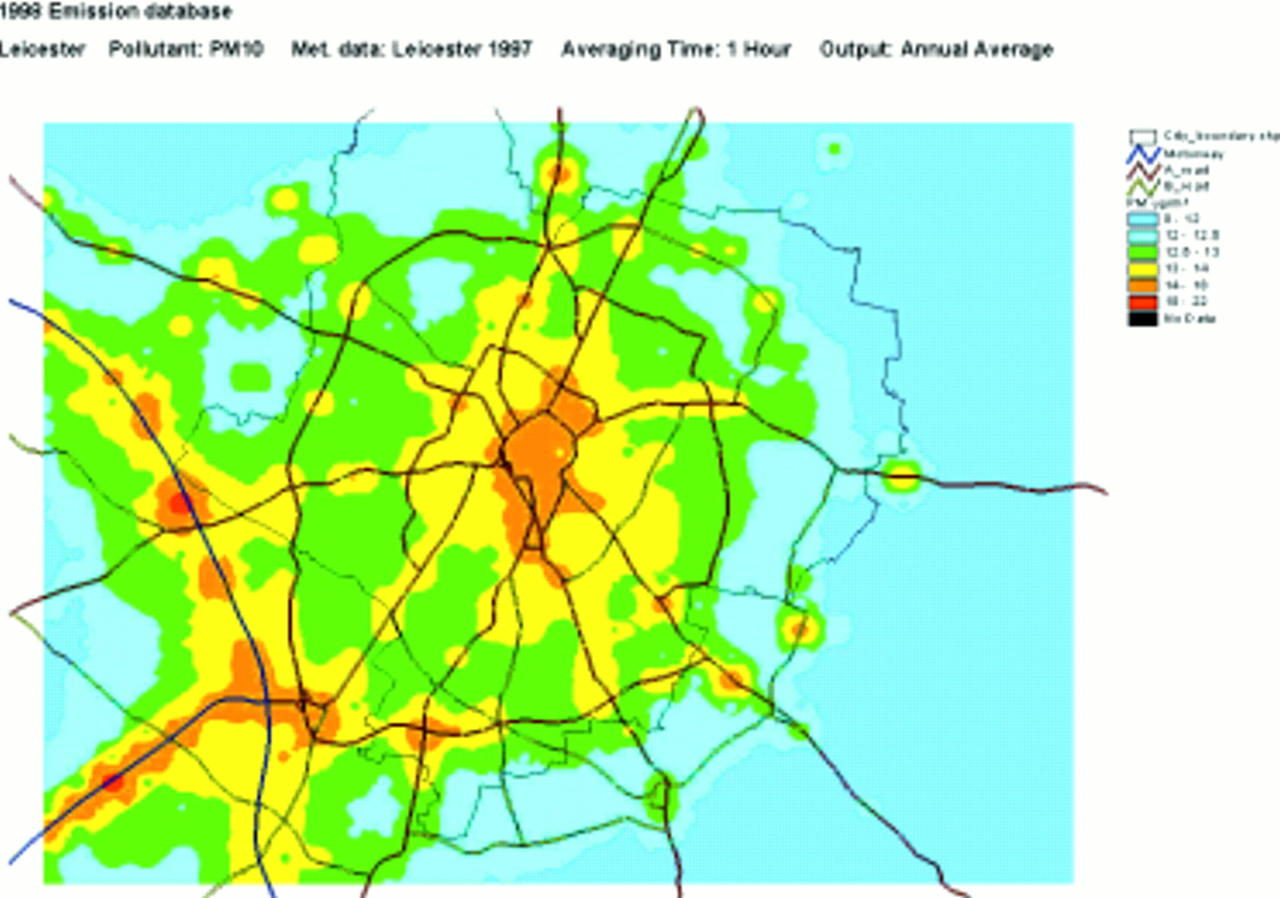
Exposure of children to fossil fuel derived particles varies substantially across countries. The European Union annual guideline for exposure to total suspended particulate matter (PM10 + mass of particles >10 μg) was 80 μg/m3 in 1995. This level was exceeded in most of the world's megacities, with Delhi reporting the highest levels of total suspended particulate matter at four times the EU guideline, followed by Beijing, Tianjin (China), Calcutta, and Mexico City.8 The source of fossil fuel particles in the world's megacities varies, with coal burning a feature in China and India, and diesel in South America. The current upper limit recommended by the UK National Air Quality Strategy for PM10 is a 24 hour mean of 50 μg/m3, with the objective that this will be the 99th centile by 2005.9 Although means are important for regulatory purposes, levels can vary widely, even when the mean exposure is relatively low (fig 3).
{kind=link}
{kind=link}
{kind=link}
Annual mean exposure to PM10 across Leicester (UK), generated by the Leicester City Council air pollution model. Areas of the highest exposure to PM10 are in red and orange; these track with heavily used roads and motorways.
PARTICLES AND ADULT MORTALITY
In a landmark study published in 1993, Dockery and colleagues10 reported the findings from a cohort of 8111 adults in northeast and midwest USA followed for 14–16 years. They found that ambient levels of fine (PM2.5) particles in the most polluted cities were associated with a 26% increase in mortality from all causes compared with the least polluted (a difference in particles of 19 μg/m3), and that increased levels of fine particles were associated with increased mortality from cardiovascular disease. Heavy criticism was directed at the study by industry groups, which lead to a recent reanalysis of the original data by the Health Effects Institute, a non-profit organisation based in Cambridge, Massachusetts. This replicated the original findings and concluded that all PM fractions (PM10, PM10–2.5, and PM2..5) were associated with both respiratory and cardiac hospital admissions, and with mortality from all causes.11 Whether high levels of PM10 hasten death in adults by a few days, or whether they appreciably shorten the life span of vulnerable individuals, remains unclear. There are few studies into the effects of the UF particle fraction per se on mortality. Wichmann and colleagues12 in Erfurt, Germany, found effects on adult mortality, both for the mass of fine particles (0.1–2.5 μm) and for the number of UF particles, indicating that UF particles have a toxic effect in their own right.
MORTALITY IN CHILDREN
Associations between PM10 and mortality in children have been reported, challenging the assumption that PM effects are limited to older adults who may not have long to live. Woodruff and colleagues13 analysed a cohort of 4 million USA infants born between 1989 and 1991 in 86 metropolitan areas. After adjusting for other covariates, the odds ratio for total postneonatal mortality for high exposure (versus low exposure) was 1.1 (95% confidence interval 1.04 to 1.16). In normal birth weight infants, high PM10 exposure was found to be associated with sudden infant death syndrome, and with mortality as a result of respiratory causes. A similar association was reported by Bobak and Leon,14 who showed a consistent association between the concentration of atmospheric particles and post neonatal death in all births in the Czech Republic from 1989 to 1991. These, and data from Mexico City showing an association between PM2.5 and total infant mortality,15 indicate that there is a causal relation between particle exposure and infant mortality.
RESPIRATORY DISEASE IN CHILDREN
In women, effects of PM10 have been detected that could influence the respiratory health of their children. Ritz and colleagues16 reported a 20% increase in preterm birth for every 50 μg increase in ambient PM10 levels during the six weeks before birth. Susceptibility to the adverse effects of PM10 in older children (>6 years) is increased in asthmatics, but associations between PM10 and respiratory disease (bronchitis) have also been reported in non-asthmatic children.17 To date, objective studies into the respiratory effects of PM10 have used lung function as an outcome. Some have been performed in environments where the majority of PM10 is not from traffic. For example, a fall in peak expiratory flow rate (PEF) of 0.55 l/min was detected in asthmatic children (10–12 years) living in a Canadian pulp mill community for every 10 μg/m3 increase in PM10.18 In this study, no association was found between increased PM10 and decreased PEF for children with no pre-existing respiratory disease.18 Where traffic emissions are the main source of particles, correlations between PEF and PM10 (over the preceding four days) have been observed for children with asthma.19 These short term changes in lung function might be clinically significant. A Seattle study of asthmatic children found that for every 11 μg/m3 increase in PM10, there was an 1.15 increase in the relative risk for asthma related emergency department visits.20 Another concern is that long term exposure to high levels of PM10 may lead to abnormal lung development. In a prospective study of 12 cities in Southern California set up in 1993, children exposed to the highest concentrations of PM10 over four years were estimated to have a cumulative deficit of 6.1% in a lung function measurement of small airway function compared with those exposed to the lowest levels of PM10.21
These epidemiological data suggest that the short term effects of PM10 are probably small in healthy children, but are amplified in children with ongoing respiratory symptoms and chronic disease. However, small effects at the individual level will translate into a large effect in a population, as most children are exposed to fossil fuel derived PM10 (table 1).22 In addition, the increased prevalence of wheeze in young children over the past decade,23 has resulted in an increased population with pre-existing symptoms, and thus more children at risk from the adverse effects of PM10. Whether the magnitude of the effects of PM10 on children has been underestimated remains a matter of debate. Too much “noise” from confounding variables may be one explanation for the finding of the PEACE study, a European collaborative study of children aged 6–12 years with respiratory symptoms. This study found no consistent association between PM10 and peak expiratory flow, respiratory symptoms, or medication use over a two month period.24 The study designers, in retrospect, have suggested that the study period was too short.25 When the Dutch contributors extended the study to three winter periods, clear effects of PM10 on >10% decrements in PEF, and increased lower respiratory tract symptoms were detected.26
Health effects of traffic related particle pollution on paediatric respiratory health across three European countries
Most published studies have extrapolated individual exposure to PM10 using data generated from widely spaced monitoring stations. The true heath effects in children could therefore be much larger if individual exposure had been accurately assessed. The number of vehicles on the road outside the home is one way of estimating individual exposure, at least for traffic PM10. In a cross sectional analysis in over 100 Dutch children, those who lived within 100 metres of a heavily used road reported significantly more cough, wheeze, and doctor diagnosed asthma.27 Edwards and colleagues28 also found that preschool children living in areas with high traffic flow were more likely to be admitted to hospital with asthma. However, other studies have found no such links. Wilkinson and colleagues29 assessed traffic volumes outside homes from a UK road traffic model, and found no association between traffic flow and the risk of hospital admission for asthma or respiratory illness among 7844 children aged 5–14 years. Why do these studies produce differing results? Firstly, other potential risk factors and confounding factors have not been controlled for to the same extent as in other epidemiological studies. Secondly, the burden of PM10 associated respiratory disease in children in the UK may fall on general practitioners, rather than hospital paediatricians. What is urgently needed to resolve these areas of uncertainty, is a large prospective study of a birth cohort which combines the best measure of individual particle exposure with respiratory and other health data. Such a study will provide information on the independent effect of PM10 on respiratory disease causation, in addition to disease exacerbation.
DISEASE CAUSATION
Two studies in adults do suggest an association between exposure to road traffic levels and atopic sensitisation to pollen assessed by skin prick test,30,31 but give conflicting results on whether road traffic and symptoms of allergy are linked. There are no similar data in children. The low prevalence of atopic sensitisation to aeroallergen in the heavily polluted environment of the former East Germany32 could suggest that particle pollution is unlikely to cause atopic asthma. However, data from the former East German town of Erfurt, have shown that while industrially emitted PM10 has fallen since reunification, traffic associated UF levels have increased dramatically.33 One explanation is that the larger (less inhalable) particles act as a “sink” for the UF fraction. Therefore an increase in UF particles has not been ruled out as a contributing factor for the recent increase in atopic disease.
VULNERABILITY OF YOUNG CHILDREN
Particle induced pulmonary disease may be more severe in younger children. The London fog of 1952 resulted in larger increases in mortality in infants less than 1 year of age than in older children,34 and it is interesting that the lungs of adults who died during the fog contain mainly aggregates of UF soot that are compatible with DEP (Dr Andrew Hunt, personal communication). Few studies have addressed this question of vulnerability in children exposed to the modern pollutant mix. Braga and colleagues6 looked at paediatric hospital admissions and air pollution in Sao Paulo, Brazil, and found the largest effect in very young children younger than 2 years of age. Whether this reflects more severe pulmonary disease (caused by increased particle deposition, or an increased inflammatory response), or a lower admission threshold, remains unclear.
MECHANISMS OF DISEASE
There is good experimental data to support a causal association between DEP and exacerbations of asthma. For example, intranasal DEP in adults with ragweed allergy, greatly enhances the production of ragweed specific IgE.35 Furthermore, exposure of atopic asthmatics to 300 μg/m3 DEP for two 60 minute periods is associated with a significant increase in airway hyper-responsiveness to methacholine at 24 hours.36 The origins of paediatric bronchitis have been less extensively investigated. One possibility is that bronchitis is an exaggerated reaction to viral lower respiratory tract infection, and there are experimental data to show that particles interact with viruses. For example, pulmonary consolidation is more pronounced in mice exposed to DEP for three months prior to inoculation with influenza virus.37 There are no studies of the lower respiratory tract of children exposed to PM10, but Mexican children exposed to high concentrations of PM10 (as well as gaseous pollution), but not to cigarette smoke, have nasal ciliary dyskinesia, and a transudate between epithelial cells, that is not seen in an age matched low exposure group.38
At the cellular level, increased release of interleukin 1 (IL-1), IL-6, IL-8, monocyte chemoattractant protein 1, tumour necrosis factor α, and granulocyte–macrophage colony stimulating factor has been reported in different lung cells exposed in vitro to a range of DEP concentrations for various time periods.39 Without knowledge of the size distribution, composition, and concentration of particles that reach specific respiratory tract cells in vivo, these “pro-inflammatory” effects are difficult to interpret. To address this problem, we looked at which particles reached paediatric alveolar macrophages (AM) under ambient exposure conditions. We showed that AM from normal children contained only UF carbonaceous particles (no natural dusts), and that these particles had a morphology typical of DEP.40 For AM experiments, UF carbon may therefore be an appropriate surrogate for DEP. Experiments using UF carbon black have shown that it can stimulate lung cells. For example, UF carbon exposure of macrophages induces a greater calcium influx into cells than the same mass of fine carbon black.41 The increased reactivity of UF carbon is either a result of its very large surface area, increased particle number per unit mass, or a combination of both.41 Future experiments will need to assess the response of AM using a concentration of UF carbon that reproduces particle loading of paediatric AM in vivo.
SUMMARY AND FUTURE RESEARCH
The evidence that fossil fuel particulates adversely affect the health of children is strong. Particles stimulate lung cells to produce proinflammatory mediators in vitro, are present in the distal lung of children, and are associated with paediatric respiratory disease when crude estimates of individual exposure are used. Important questions remain about the true size of the effects and the most toxic fraction. The challenge is to identify the most toxic particle fraction of PM10, to determine how particles interact with respiratory viruses, and perhaps most importantly to discover whether particles are implicated in causing asthma.
Acknowledgments
I am grateful to Adrian Russell and Neil Cooper of the Leicester City Council pollution group for generating the PM10 exposure map, and to Dr David Dinsdale and Dr Tim Smith of the Medical Research Council Toxicology Unit, Leicester, for the electron micrograph of DEP. The PM10 map is © Crown copyright Ordnance Survey, all rights reserved (NC/01/504).