Article Text

Abstract
Objectives: To determine the prevalence of knowledge about and participation in asphyxial games, sometimes called “the choking game”, and how best to raise awareness of this risk-taking behaviour and provide preventive education.
Design: Questionnaire; collaborative research model; lay advocacy group/university researchers.
Setting: 8 middle and high schools in Texas (six) and Ontario (two). A recent death from playing the choking game had occurred in one Texas school, and two other fatalities had occurred within the state.
Subjects: Students in grades 4–12, aged 9–18 years.
Intervention: None.
Outcome measures: None.
Results: Of 2762 surveys distributed, 2504 (90.7%) were completed. The mean (SD) age of the responders was 13.7 (2.2) years. 68% of children had heard about the game, 45% knew somebody who played it, and 6.6% had tried it, 93.9% of those with someone else. Forty percent of children perceived no risk. Information that playing the game could result in death or brain damage was reported as most likely to influence behaviour. The most respected source of a preventive education message was parents for pre-adolescents (43%) or victim/victim’s family (36%) for older adolescents.
Conclusions: Knowledge of and participation in self-asphyxial behaviour is not unusual among schoolchildren. The age of the child probably determines the best source (parents or victim/victim’s family) of preventive education.
Statistics from Altmetric.com
Asphyxial games are a recognised thrill-seeking behaviour among youths. Pressure or constriction is applied to the neck or chest to restrict oxygen flow to the brain, creating a brief euphoria or “high” feeling before loss of consciousness, and a “rush” from the surge of blood flow that follows release of the obstruction. The sensations are perceived as pleasurable and promote the (thrill-seeking) behaviour. For decades, children at home, in schoolyards and at summer camps have engaged in this risk-taking behaviour known by many different names, among them “the choking game”, “blackout”, “suffocation roulette”1 and “space monkey”. Versions of the game are reported as occurring at least 50 years ago. These asphyxial games may be played in groups or alone. If the constriction is not removed in time, permanent brain injury or death may occur.2–4
In the USA, a recent report from the Center for Disease Control indicates that between 1995 and 2007, there were 82 deaths of children that probably resulted from the choking game.5 In Canada in 2006, there were 193 deaths of 10–19-year-olds by hanging, strangulation and suffocation, 175 (91%) of which were considered “intentional” (possible misdiagnosis of choking game deaths) and 18 of which were considered “accidental”.6 A recently published abstract using data from the Canadian Hospital Injury Reporting and Prevention Program database reports 74 cases (average five per year) of emergency department admission to one of 10 paediatric or four general hospitals for injuries sustained during asphyxial games. This database does not include children who died or children admitted to other hospitals in Canada.7
In 2001, we reported the risk of death from playing the choking game by hanging from a roller towel dispenser.2 This report led parents who had lost children to write to us, prompted some coroners and medical examiners to question their certifications of such deaths as suicide, and generated media interest resulting in the Canadian Broadcasting Corporation airing a documentary called The choking game. After this broadcast, more parents questioned the certification given them on their children’s death. In addition, several parents whose children had died asked us to assist them with a study they were undertaking to determine how best to raise awareness of the choking game in order to prevent further deaths and injuries.
The principal goals of this parent study were to determine the prevalence of knowledge about, and participation in, asphyxial games, and how youth might be effectively discouraged from participating in this thrill-seeking behaviour. Their secondary goal was to provide coroners and medical examiners with more knowledge about asphyxial games among youth. In this context, they were encouraged by the National Association of Medical Examiners (NAME) to undertake the study, as the NAME Board of Directors agreed that the information it would provide would more thoroughly inform decisions about the appropriate certification of cause and manner of death in children who succumb during solitary, self-induced acute asphyxiation (personal communication, 26 June 2006). We were asked by the parents to refine their questionnaire and analyse and report their data.
METHODS
Questionnaires designed empirically by the parents contained basic questions on age, gender and knowledge about, and/or participation in, the choking game, and the following open-ended questions: what would make you stop if you were doing it? who would you be most likely to listen to about not playing the game? The questionnaire was refined by a researcher experienced in questionnaire design and evaluated by a school librarian through discussion in an open forum with children in grades 3–8 in a school not involved in the study. It was determined that children at this grade level had sufficient reading skill and understanding to respond appropriately to the questions. Regional School Boards (Canada) and Inspectors of Schools (USA) had been approached by the parents organising the study for permission and direction about study conduct; they approved the questionnaires. Two schools participated in Ontario and six in Texas. There had been a recent death of a child while playing an asphyxial game in one Texas school, and two other deaths had occurred in other communities elsewhere in the state.
Subjects were the children in grades 4–12 (age 9–18 years) in the participating schools. The parents conducting the study distributed envelopes of questionnaires to the schools, which then distributed the envelopes to the teachers. Each teacher received sufficient questionnaires to distribute one to each member of the class. Teachers also received written instructions on how to conduct the survey to ensure appropriate and consistent methods. They instructed the children that they were not to put their names on the questionnaires, and did not have to complete them if they chose not to. As directed by the School Boards/Inspectors of Schools, the survey was an in-class activity that was not scheduled in advance, so that the cohort of children was not biased by inclusion of children who chose to be absent because of prior knowledge that the survey was to take place. The schools were a convenience sample, and were selected by involved parents and the School Boards. Table 1 shows socioeconomic data on the US schools. Comparable data were not available for the Canadian schools.
At each school, prevention/educational presentations were made by parents and/or police to assemblies of children immediately after completion of the questionnaires.
The University of British Columbia Behavioral Ethics Research Board approved the analysis of the data for publication. Data were entered into a Microsoft Excel spreadsheet, responses to the open-ended question were content-coded, and data were analysed using descriptive statistics.
RESULTS
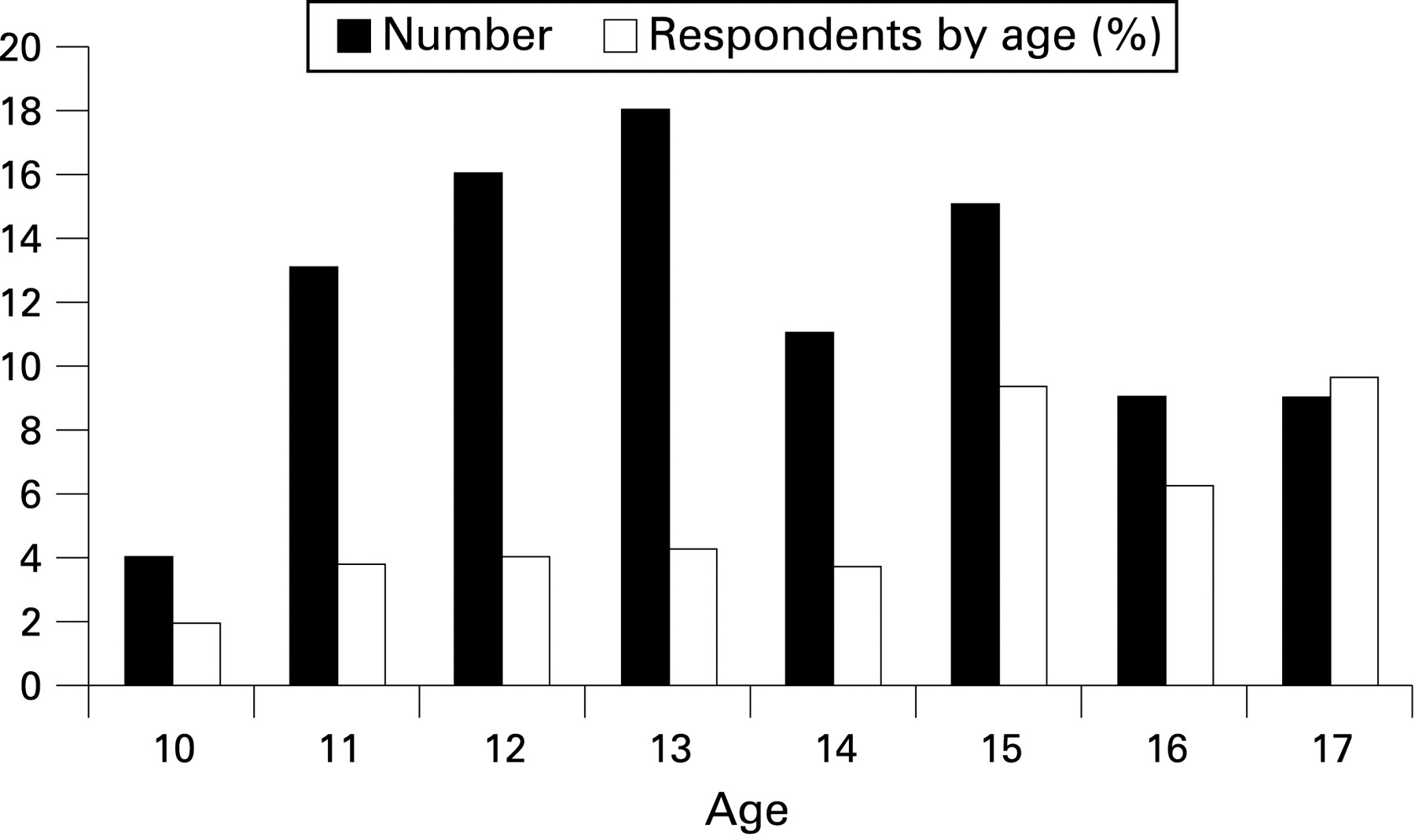
A total of 2762 surveys were distributed to the classes (on the basis of class enrolment). Of these, 2504 (90.7%) were completed and included in the analysis. The remainder represents some children who were absent that day, some who declined to participate, and those whose forms were excluded because fewer than three fields were completed. These groups were not quantified, but “absence” was due to coincidence not choice to avoid participation, as the survey was an unannounced class activity, and there was no coercion. The mean (SD) age of respondents was 13.7 (2.2) years (fig 1) (median 13, interquartile range 12–15). Just over half (1277; 52%) were female. A large proportion (1703; 68%) of the children reported having heard about the game and 58% of these were male. Of those surveyed, 926 (37%) had heard about it a year or more previously (ie, before a choking game fatality in their community, or television or press coverage on the subject). The mean (SD) age at which children reported having learned about it was 12.4 (2.5) years (fig 2).


A total of 1127 children (45%) knew somebody who played asphyxial games, and 164 (6.6%) admitted participating; of the latter, 90 (55%) were male. Of those who had played the game, 154 (94%) had done so with someone else present; all of the girls who had tried it, had done so with someone else present. Ten (11%) male respondents reported playing it alone. Ninety-five (58%) of the children who had played the game reported “still doing it”. The percentage of children still participating varied with age (fig 3), with the highest percentage (6–10%) among those aged 15–17.

It was thought by 1002 children (40%) that there was no risk in playing the game; 47% of these were male. Among those who reported that they believed there was no risk in playing the game, 69 (8%) had tried it, and 18 (2%) still played. Among those who reported that they believed there was a risk, 96 (8%) had tried it, and 35 (2.7%) reported still playing.
In assessing what information would discourage children from participating in the game, the most common response (given by 1071 (57%) of 1871 who answered) to the question “what would make you stop doing it” was that “you could die or have brain damage”. Knowledge of this fact was reported by all age groups to be likely to change behaviour. Approximately 5% of responses incorporated phrases such as “factual information” or “rate of death” or “how many children die from it”, indicating that statistics or data on the level of risk would be of value.
Of the remaining responses, the majority indicated that respondents had never played the game, had never heard of it, or believed that it was “stupid”. Fifteen children (0.8%) responded with statements such as “nothing anybody said would make me stop”, or “only death would make me stop”. Seven (0.3%) indicated that photographs of the bodies would stop them, and another four (0.2%) indicated that it would take a severe event (eg, “someone dying by my hand or my friend’s hand”) to get them to stop.
To assess the most effective source of “risk” information, children were asked to whom they would be most likely to listen about not participating in the game. The responses varied with age (fig 4), with younger children indicating that they were most likely to listen to their parents, and older children indicating that near-victims, members of a victim’s family, or peers would be most likely to influence future behaviour.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
This study exemplifies a collaborative model of research. The study was initiated by a lay advocacy group and completed with the guidance of qualified researchers. The lay group obtained approval and direction regarding consent from School Boards (Canada) and Inspectors of Schools (USA), organised implementation of the survey with the schools, and completed data collection. The university-based researchers provided refinement of the wording and ensured comprehension of the questionnaire, and conducted the independent data analysis and interpretation.
In the population surveyed, almost half the children knew somebody who had participated in an asphyxial “game”, 7% admitted that they had done so themselves, and 10 boys described doing it as a solitary behaviour. Although one of the schools surveyed had experienced a recent death from the choking game and five were in a state where two fatalities had recently been reported, a considerable number of the children (95) were still participating in asphyxial games when surveyed, and more than one-third of children reported knowing about this form of risk-taking behaviour 1 year earlier (before major television coverage, a local tragedy or press coverage on the topic). The data on participation in asphyxial games from our study is consistent with that obtained subsequently in the 2007 Ontario Student Drug Use and Health Survey reported by the Canadian Centre for Addiction and Mental Health.8 In that survey, a random half of 6323 students in grades 7–12 were asked the question “Have you ever been choked by someone or tried to choke yourself on purpose … in order to “get high” …?” About 7% of students responded “yes”.
Preventive education appears important because of the number of children admitting to playing asphyxial games and the particularly high risk posed for those who play alone. Furthermore, 40% of the children surveyed indicated that they perceived there to be no risk associated with this activity. Importantly, more than half the children surveyed indicated that they would be discouraged from playing asphyxial games if they knew that the risks of doing so included the possibility of death or significant brain damage.
Our survey data support the provision of preventive education through the school system. Schools promote acquisition of lifelong attitudes to risk-taking behaviour relevant to injury prevention,56 and can positively influence future behaviour through involvement of informed adults and influential peers. Furthermore, participation in asphyxial games is known to occur in schools, and explicit material exists on the internet. Both situations require acknowledgement and provision of perspective. Students can be made aware of the extreme consequences possible with this form of risk-taking behaviour, especially when it is a solitary activity or involves constriction of the neck with a ligature of some sort. In addition, our survey asked how the impact of such education could be optimised. Responses indicated that the effect of such information will be greatest if the message is delivered by parents in lower grades, and by peer survivors or families of victims at higher grades. We recognise that, even with broad knowledge of the consequences of such behaviour, it is unlikely that all deaths from asphyxial games will be eliminated. However, children are entitled to the information they need in order to be able to make informed decisions, a view strongly endorsed by parents who have lost children through the choking game.
Injury prevention is not limited to education. Legislation and technological improvement are other components that may contribute to injury prevention. Legislation has been introduced in our province regarding cloth towel dispensers, which were used in a series of asphyxial incidents. These towel units must now either be mounted at a lower height or incorporate a safety shield (a technological modification). Both measures are intended to make it difficult or impossible to wrap a towel loop around the neck as an asphyxial ligature.2
The secondary objective of our survey was to provide data for parents, educators and health professionals on the incidence of asphyxial games and the number of children aware of this risk-taking behaviour. This information could then contribute to inclusion of this topic in family conversation and health education and better distinction between accidental and non-accidental strangulation. Accidental strangulation occurs in various situations to toddlers and preschool aged children,7 but in adolescents it usually results from unsafe play.24 However, asphyxial games appear to represent a form of unsafe play that is not appropriately recognised by parents, teachers, coroners or doctors. Reports of deaths from asphyxial games are rare in the medical literature,13 and are more often reported in the lay press.9 Hanging is a common method of suicide among adolescents,10 and in older male adolescents autoerotic behaviour involving partial strangulation is a recognised, usually-solitary, act that may be mistaken for attempted suicide. Neither should be confused with asphyxial games, which have no overtones of suicidal behaviour or sexuality.1
Hanging deaths in pre-adolescent and adolescent boys have been identified as a problem needing further investigation in England and Wales.11 In Canada and the USA, re-examination of strangulation deaths previously described as suicides has been prompted by reports of deaths attributed to asphyxial games. A recent report3 examining 24 cases of hanging in young children and adolescents (18 (75%) male) described a profile of youth engaging in this behaviour that differs substantially from the typical historical and investigative profile of youth suicide. Coroners and/or medical examiners have not traditionally received or expected information on asphyxial games in such cases. The lack of sufficient data has led, in an undefined proportion of cases, to an erroneous certification of suicide as the manner of death.3
Key points
Children (pre-teens and adolescents) play asphyxial games, but the incidence is unknown.
Deaths due to this risk-taking behaviour are often deemed to be suicide.
There is a high incidence among children of knowledge about (68%), and participation in (7%), asphyxial games.
Coroners and medical examiners should consider certifying deaths occurring in such circumstances as “accidental”.
Education has the potential to inform and reduce participation in this risk-taking behaviour.
In response to media coverage, particularly the broadcast of the documentary The choking game, we received considerable correspondence, much of it from older adults describing participation in asphyxial games when they were children (one correspondent was 65, and reported playing it when she was 12). This correspondence was almost equally distributed between males and females, and consistently related that it was someone’s hands or arms that were used to achieve the altered sensation, and never a form of mechanical constriction. One example reads: “My girl friends and I used to play a similar game … in the school bathroom. We would take turns helping each other ‘faint’. It started with deep breathing until we were dizzy, then, with arms around the abdomen from the rear; someone would squeeze you until the next recollection was waking up with a tingling sensation all over your body, on the bathroom floor, completely disoriented.… I was surprised that young pre-teens risk their lives with this secret game and how it is now responsible for so many deaths, mistakenly claimed as suicides… I am writing this to help educate as many people as it will reach that this is a very old ‘secret game’ that has evolved into something deadly”.
Limitations
The schools included were not randomly selected. The sample included one school at which a child had died in the recent past as a consequence of playing the choking game and others that were either geographically proximate to a death (two deaths in the same state) or linked to another school where a death had occurred (the high school associated with a middle school). Two of the schools had not had any deaths nor had there been any death in the community. This purposive sampling had the potential to significantly affect the data and its applicability to other schools and communities. However, in this context, our data on the incidence of participation in asphyxial games does agree with recent data from the Canadian Centre for Addiction and Mental Health.8
Our survey was facilitated by parents in an advocacy group promoting awareness of the dangers of asphyxial games and school officials made aware of the potential for tragic outcomes to result from this risk-taking behaviour, which again may have affected the data. In addition, although schools in both Canada and the USA were included, a limited spectrum of cultural and economic determinants of health was represented. Collection of additional data from more schools is desirable, but may be more complex to initiate.
IMPLICATIONS FOR PREVENTION
Our data suggest that children who know that asphyxial games can result in death or brain damage are likely to change their future behaviour. Our data also suggest that the age of the child probably influences whether a preventive message is best heard from parents, peer near-victims or the family of victims.
Acknowledgments
We remember the children who died playing this “game”, and thank their parents Sharron Grant, Kristen Orser, Debbie LaRocque, Carrie Draher, Sarah Pacette and Charlene Sandel for initiating the study and collecting the data. We refer other parents to their organisation: G.A.S.P. (Games Adolescence Shouldn’t Play) (www.GASPinfo.com). We thank Daniel Leppington, Keith Gagnon and Jonathan Cannon for entering the data.
Footnotes
Competing interests: None.