
Abstract
Objective: Stewart's physicochemical approach to acid-base balance defines the aetiology of a metabolic acidosis by quantifying anions of tissue acids (TA), which consist of unmeasured anions (UMA) and/or lactate. We hypothesised that an increase in TA during metabolic acidosis would lead to a compensatory fall in the plasma chloride (Cl) relative to sodium (Cl:Na ratio) in order to preserve electro-neutrality. Thus, the Cl:Na ratio could be used as a simple alternative to the anion gap in identifying raised TA.
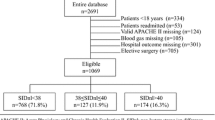
Patients: Two hundred and eighty two consecutive patients who were admitted to our Paediatric Intensive Care were enrolled in the study.
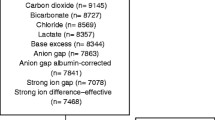
Interventions: We obtained 540 samples (admission n=282, 24 h n=258) for analysis of blood chemistry, lactate and quantification of TA and UMA. Samples were sub-grouped into those with metabolic acidosis (standard bicarbonate <22 mmol/l) either with or without increased UMA (>3 mEq/l).
Measurements and results: Metabolic acidosis occurred in 46% of samples, of which 52.3% (120/230) had increased UMA. The dominant component of TA was UMA rather than lactate, and these two components did not always rise in tandem. Our hypothesis of relative hypochloraemia was supported by a lower Cl:Na ratio (P<0.0001) but not a lower absolute Cl (P=0.5) in the acidotic subgroup with raised UMA, and by the inverse relationship between TA and the Cl:Na ratio. (coefficient of determination (r2)=–0.37, P<0.0001). The best discriminator for the presence of raised TA was the albumin-corrected anion gap (AGcorr), however, this could not track changes in TA with clinical accuracy. The Cl:Na ratio discriminated reasonably well, a ratio of <0.75 identified TA (positive predictive value (PPV) 88%) with a likelihood ratio (LR) similar to the AG (7.8 vs7.4). Conversely, a high ratio (>0.79) excluded TA (PPV 81%, LR 4.5). Base deficit (BD) and lactate performed poorly.
Conclusion: In metabolic acidosis due to TA, plasma Cl concentration decreases relative to sodium. The Cl:Na ratio is a simple alternative to the AG for detecting TA in this setting.
Similar content being viewed by others

Author information
Authors and Affiliations
Additional information
Final revision received: 11 January 2001
Electronic Publication
Rights and permissions
About this article
Cite this article
Durward, A., Skellett, S., Mayer, A. et al. The value of the chloride:sodium ratio in differentiating the aetiology of metabolic acidosis. Intensive Care Med 27, 828–835 (2001). https://doi.org/10.1007/s001340100915
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s001340100915