Article Text

Abstract
Objective To compare the effectiveness of a 2-year camp-based family treatment programme and an outpatient programme on obesity in two generations.
Design Pragmatic randomised controlled trial.
Setting Rehabilitation clinic, tertiary care hospital and primary care.
Patients Families with at least one child (7–12 years) and one parent with obesity.
Interventions Summer camp for 2 weeks and 4 repetition weekends or lifestyle school including 4 days family education. Behavioural techniques motivating participants to healthier lifestyle.
Main outcome measures Children: 2-year changes in body mass index (BMI) SD score (SDS). Parents: 2-year change in BMI. Main analyses: linear mixed models.
Results Ninety children (50% girls) were included. Baseline mean (SD) age was 9.7 (1.2) years, BMI 28.7 (3.9) kg/m2 and BMI SDS 3.46 (0.75). The summer-camp children had a lower adjusted estimated mean (95% CI) increase in BMI (−0.8 (−3.5 to −0.2) kg/m2), but the BMI SDS reductions did not differ significantly (−0.11 (−0.49 to 0.05)). The 2-year baseline adjusted BMI and BMI SDS did not differ significantly between summer-camp and lifestyle-school completers, BMI 29.8 (29.1 to 30.6) vs 30.7 (29.8 to 31.6) kg/m2 and BMI SDS 2.96 (2.85 to 3.08) vs 3.11 (2.97 to 3.24), respectively. The summer-camp parents had a small reduction in BMI (−0.9 (−1.8 to −0.03) vs −0.8 (−2.1 to 0.4) in the lifestyle-school group), but the within-group changes did not differ significantly (0.3 (−1.7 to 2.2)).
Conclusions A 2-year family camp-based obesity treatment programme had no significant effect on BMI SDS in children with severe obesity compared with an outpatient family-based treatment programme.
Trial registration number NCT01110096.
- Obesity
- Metabolic
- RCT
- Family-based treatment
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What is already known on this topic?
Family based treatment of childhood obesity is well documented and established.
Observational studies of camp-based immersion treatment of childhood obesity have shown promising results.
Few previous studies included a control group, only one had a randomised design and parents were not actively involved.
What this study adds?
A family camp-based immersion treatment programme—including parents with obesity—had no significant effects on BMI SD score (BMI SDS) or parents’ BMI.
The camp-based immersion treatment programme was costly; the incremental cost per family was €5902 compared with the outpatient-based treatment programme.
The small treatment effects of the camp-based programme do not justify the high extra treatment costs compared with lifestyle support alone.
Introduction
A recent meta-analysis of 20 randomised controlled trials (RCTs) addressing family-based lifestyle interventions (including dietary intake, physical activity and behavioural strategies) demonstrated only small effect sizes (Hedge’s g=0.47, 95% CI 0.36 to 0.58).1 Importantly, only 3 of the 20 studies had more than 1-year follow-up.2–4 In addition, a recent review concluded that camp-based immersion treatment of childhood obesity has shown promising results.5 However, few of the reviewed observational studies included an adequate control group, and only one had a randomised controlled design.6 Furthermore, to the best of our knowledge, no study has assessed the effect of including one or more parents with obesity together with their child during the immersion treatment stay. It has been suggested that targeting both parent and child may enhance treatment effectiveness compared with child-only interventions7 ,8 and, moreover, it might improve the cost-effectiveness of treatment by reducing obesity in both children and their parents.
Accordingly, we aimed to assess the effectiveness of a 2-year camp-based immersion treatment programme as compared with an outpatient family treatment programme. We hypothesised that children and parents in families undergoing the immersion treatment would reduce their obesity measured as body mass index (BMI) and BMI SD score (BMI SDS, children) to a greater extent than the children and parents in families receiving the outpatient treatment. Secondary end points were changes in various anthropometric measures, body composition, physical capacity, biochemical parameters and treatment costs.9
Patients and methods
Study design and setting
The Family Based Intervention in Childhood ObesitY was a pragmatic two-armed RCT conducted at two tertiary care centres in Norway. Data collection started in April 2010 and ended in June 2013.
Participants
Families with at least one obese child (BMI ≥ iso-BMI 30, International Obesity Task Force),10 aged between 7 and 12 years and at least one obese parent (BMI ≥30 m/kg2), were recruited through primary healthcare facilities (>75%), media and from regular referrals in 2010 (n=39) and 2011(n=55). Exclusion criteria were syndromal obesity, other medical conditions associated with weight gain or not being able to participate in either of the treatment programmes. Written informed consent was provided from all participants, and the study was performed in accordance with the Declaration of Helsinki. The study was approved by the Regional Committee for Medical and Health Research Ethics (2009/176). All expenses including work absenteeism compensation were covered by the national health and welfare system.
Interventions
The summer-camp and the lifestyle-school programmes are described in figure 111 and in the appendix (interventions—additional details).

Graphical depiction of interventions and measurements for the two treatment groups in the FamilY study. Adapted from Perera et al.11
Briefly, the summer-camp participants underwent an initial 2-week programme at a private rehabilitation institution with four follow-up weekends (2 days at 6, 12, 18 and 24 months). The lifestyle-school group attended 4 days (23 hours) in the outpatient clinic over a period of 4 weeks. In addition, all participants were offered monthly primary care follow-up for 2 years by a public health nurse. All interventions focused on healthy choices in terms of nutrition and physical activity, and were based on behavioural techniques.12–14
Outcomes
The primary outcome was the 2-year change in BMI SDS. In addition, the 2-year changes in BMI were compared, and the children were categorised into those achieving a reduction in BMI SDS of ≥0.25 and 0.50 versus those who did not (participants with missing data were classified as unsuccessful).
All participants underwent a semi-structured interview and clinical examination at baseline. Anthropometric characteristics and bioimpedance measures were registered at baseline, 1 year (only children) and 2 years (range 24–28 months). Venous blood samples were drawn at baseline and 2 years.
Height was measured to the nearest 0.1 cm using Heightronic Digital Stadiometer. Weight and body composition were measured using a bioimpedance body composition analyser (BC-418, Tanita, Tokyo, Japan). BMI was converted to age-adjusted and sex-adjusted BMI SDS according to the WHO reference chart,15 using the WHO growth reference tools for SPSS.16 Waist circumference was measured at the midpoint between the upper part of the right iliac crest and the lower part of the lateral rib cage using a standard anthropometric tape.
Blood pressure and resting heart rate were measured in a sitting position after 5 min of rest using digital oscillometric devices, Dinamap ProCare or Scan-Med CAS 740.
A 6 min walk test17 was undertaken by both the children and adults, based upon a lap of 30–50 m on flat, hard ground.
Blood samples
All blood samples were taken after an overnight fast and stored at −70°C until thawed and thereafter analysed using accredited methods (table 1, see online supplementary appendix table A4).
Baseline demographics, clinical and biochemical characteristics of the 90 children included in the analysis
supplementary appendix
Insulin resistance was calculated by the homeostasis model assessment of insulin resistance (HOMA-IR) equation: (fasting insulin (mU/L)×fasting glucose (mmol/L))/22.5.
Intervention costs
Summer-camp cost was calculated by taking per diem cost per family multiplied by the number of days (14 plus 2×4=22). Per diem cost was collected from the price list for the private rehabilitation institutions. Lifestyle-school cost was based on a microcosting method,18 taking number of hours spent by personnel categories according to the schedule and multiplying by price per hour according to wage level, and thereafter by dividing the average number of participating families. Costs are presented in 2012 Euro applying a depreciation rate NOK/Euro of 7.47.
Sample size
The sample size was calculated based on an anticipated clinically meaningful mean difference in BMI SDS of 0.1 between the two groups after 2 years assuming a SD of 0.15 in both groups. Given a significance level of 5% and keeping statistical power to >80%, at least 37 children in each group were needed to complete the study.
Randomisation
The participants (families) were randomly assigned to one of the two parallel groups in a 1:1 ratio. Blocked randomisation (block sizes of four and five participants) with stratification of treatment centre was computer-generated by technical staff using an internet-based device. Randomisation was performed 2 days after the baseline measurements. Allocation was concealed from both participants and trialists. Participants and healthcare personnel were not blinded to treatment.
Statistical analyses
Differences between pairs of continuous and categorical variables were assessed using independent samples t-test, Mann-Whitney U test, Wilcoxon test or Fisher’s exact test as appropriate.
Selected outcome measures collected over time were analysed using a linear mixed model19 with an unstructured correlation matrix, incorporating all subjects for whom baseline data were available according to the intention-to-treat principle, taking any random baseline differences into account. Fixed effects were treatment, time and treatment-time interaction. All models (except for biochemical analyses) were adjusted for treatment centre. We estimated mean changes from baseline to 2 years, and the overall differences taking all three measurements (baseline, 1 year and 2 years) into consideration. Furthermore, we performed three sensitivity analyses, first an ‘as-treated’ analysis including all participants who underwent at least two measurements, second, the standardised effect sizes (Cohen's d) of main outcomes20 and third, analysis of covariance (ANCOVA) of main outcomes. We also included a sensitivity analysis comparing the proportions of children in each group categorised into those achieving a reduction in BMI SDS of ≥0.25 and 0.50 versus those who did not, assigning fail to those missing in the summer-camp group and success for those missing in the lifestyle-school group, and then reversing the direction of the missing assumption.
All tests were two-sided. p Values <0.05 were considered statistically significant. However, no adjustments for multiple secondary outcomes were applied and particular attention should be directed towards p <0.01.
All analyses were performed with SPSS V.21.0 (IBM, Armonk, New York, USA) and STATA V.13 (StataCorp, College Station, Texas, USA).
Results
Participant flow chart is shown in figure 2. A total of 90 families were available for the intention-to-treat analysis. After randomisation, 18 families refused participation and 6 families withdrew during the first year, leaving 69 for inclusion in the ‘as-treated’ analysis.
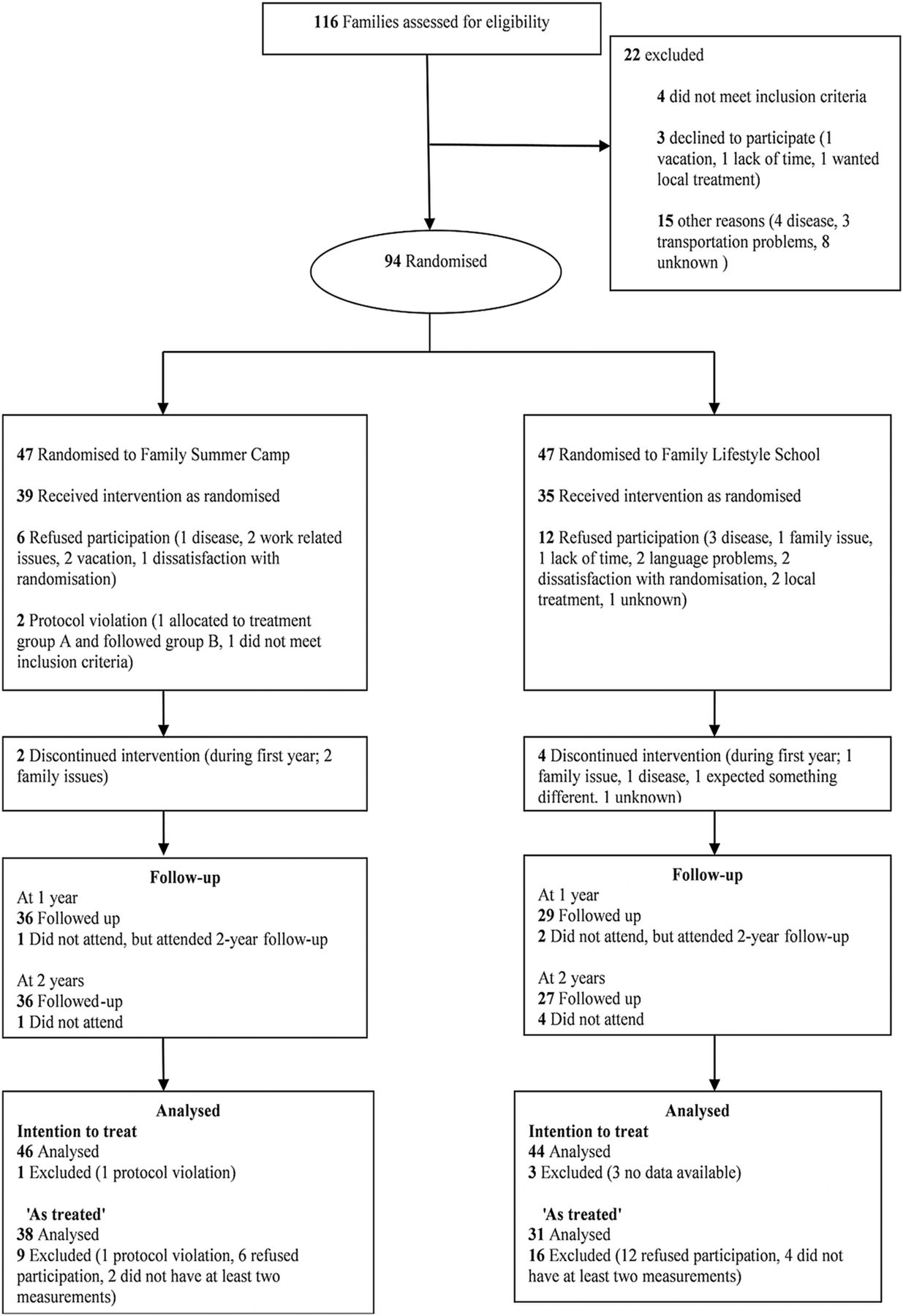
Participant flow chart: families with obesity assessed for eligibility, randomisation, intervention and follow-up.
The 90 children (50% girls) had a mean (SD) age of 9.7 (1.2) years, BMI 28.7 (3.9) kg/m2 and BMI SDS 3.46 (0.75). Baseline characteristics did not differ significantly between groups, except for small differences in resting heart rate, HOMA-IR and gamma glutamyl transferase (table 1). The parents had a mean (SD) age of 40.7 (5.0) years and BMI 37.0 (4.6) kg/m2. Other baseline characteristics of parents are shown in online supplementary appendix table A2.
Main outcomes
The mean (95% CI) reduction in BMI SDS did not differ significantly between groups, −0.11 (−0.49 to 0.05). In contrast, compared with children in the lifestyle-school group, the summer-camp children had a significantly lower 2 years increase in BMI, −0.8 (−3.5 to −0.2) kg/m2 (table 2). Furthermore, the summer-camp and lifestyle-school completers did not differ significantly at 2 years in the baseline-adjusted BMI, 29.8 (29.1 to 30.6) vs 30.7 (29.8to 31.6) kg/m2 and BMI SDS, 2.96 (2.85 to 3.08) vs 3.11 (2.97 to 3.24), between-group differences −0.9 (−2.0 to 0.3) and −0.14 (−0.32 to 0.03), respectively (ANCOVA). The standardised effect sizes between treatment groups in BMI SDS and BMI were 0.38 and 0.40, respectively. Both parent groups had small reductions in BMI (0.8–0.9 kg/m2), with no significant between-group differences; 0.3 (−1.7 to 2.2) (see online supplementary appendix, table A3).
Within-group changes and between-group differences in clinical outcomes of children from baseline to 2-year follow-up
Changes in anthropometric measures, body composition and physical capacity
Compared with children in the lifestyle-school group, the summer-camp children had significantly lower 2 years increases in fat mass (2.4 kg), and a larger decrease in waist-to-height ratio (table 2).
The majority of children had a BMI SDS >2 at 2 years (figure 3).15 There were differential group changes across time in body weight, BMI, BMI SDS, body fat percentage, fat mass and diastolic blood pressure (all p<0.01, figure 4). The mixed model ‘as-treated’ analysis confirmed the results from the main analysis (data not shown).

Individual line plots of body mass index SD score (BMI SDS) at baseline, 1 year and 2 years for the children. Summer-camp group in blue and lifestyle-school group in green.
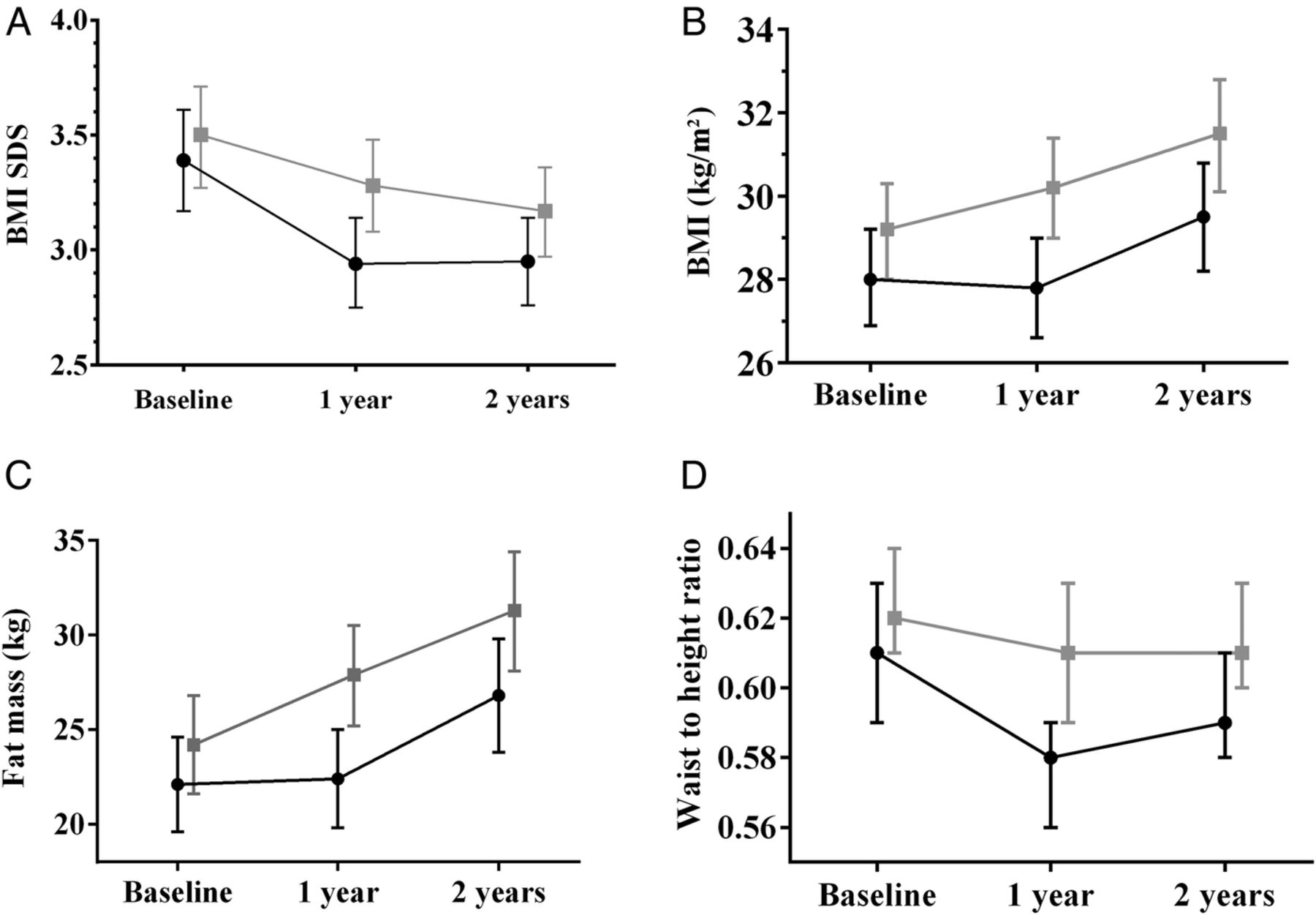
Children's body mass index SD score (BMI SDS), BMI (kg/m2), fat mass (kg) and waist-to-height ratio by treatment group at baseline, 1 year and 2 years. Values are presented as estimated means (95% CIs). Summer-camp group in black dots and lifestyle-school group in grey squares.
The summer-camp group had a decrease in BMI SDS during the first year of treatment, and then levelled off, while the lifestyle-school group showed a slower, steadier decrease. Accordingly, BMI was stable during the first year in the summer-camp group, while a continuous increase over the 2 years was registered in the lifestyle-school group (figure 4).
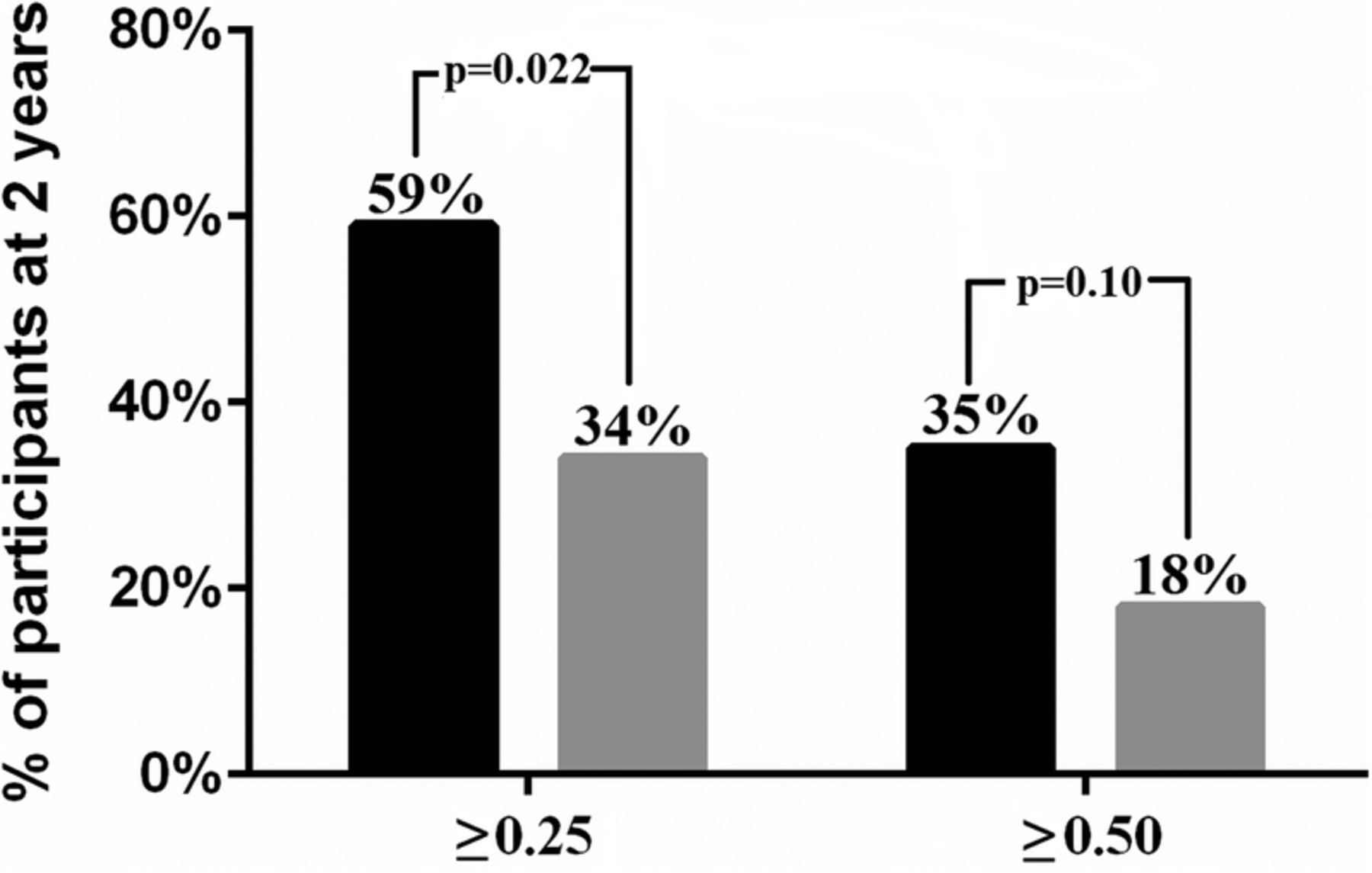
The percentages of children maintaining a reduction in BMI SDS ≥0.25 and ≥0.50 after 2 years were slightly higher in the summer-camp group than in the lifestyle-school group; 59% vs 34%, between-group differences 25% (5% to 45%) and 35% vs 18%, between-group differences 17% (−2% to 35%), respectively (figure 5). A sensitivity analysis assigning fail to those missing in the summer-camp group and success for those missing in the lifestyle-school group did not change the results significantly (data not shown).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Percentage of children (n=90) that achieved a reduction in body mass index SD score of ≥0.25 and ≥0.50 at 2 years, by treatment group. Children with missing data are classified as unsuccessful. Summer-camp group in black and lifestyle-school group in grey.
Parents in the summer-camp group had minor beneficial changes in some secondary outcomes compared with the parents in the lifestyle-school group (see online supplementary appendix, table A3).
Biochemical analyses
The summer-camp children had a lower adjusted mean increase in HOMA-IR (−2.5 (−4.4 to −0.7)), a lower reduction in high-density lipoprotein-cholesterol (0.2 (0.02 to 0.3) mmol/L) and a lower increase in triglycerides (−0.3 (−0.6 to −0.02) mmol/L) than those in the lifestyle-school group. In addition, the treatment groups had comparable reductions in low-density lipoprotein-cholesterol levels (within-group difference), 0.3 mmol/L (0.2 to 0.5) and 0.4 mmol/L (0.2 to 0.6), respectively. Other cardiometabolic variables did not differ significantly between treatment groups (see online supplementary appendix, table A1).
Treatment costs
The summer-camp and lifestyle-school treatment cost per family were €6513 and €611, an incremental cost per family of €5902.
Discussion
This 2-year randomised controlled study of children aged 7–12 years in families affected by obesity showed no significant long-term effect on the primary outcome; the BMI SDS changes did not differ significantly between groups. In contrast, the summer-camp children had a slightly lower increase in BMI units (0.8 kg/m2) than those who underwent the lifestyle-school. The parents had a small weight loss with no significant difference between treatment groups. In addition, the summer-camp children had slightly more favourable changes in some cardiometabolic risk factors, compared with the lifestyle-school group. The immersion treatment programme was costly.
To the best of our knowledge, this is the first RCT to explore the long-term effects of a camp-based intervention in which both children and parents with obesity undergo a long-term immersion treatment programme. Although a recent review5 reported on average 20% reduction of overweight at follow-up, the observational uncontrolled design and short follow-up of these studies may have inflated the results. Nevertheless, a Belgian randomised controlled study of children aged 7–16 years who participated in a healthy-eating lifestyle programme at a 10-day summer camp, demonstrated more than 10% reduction in percent overweight at 1-year and 5-year follow-up.6 ,21 This study did, however, implement national growth charts, making any appropriate comparison with our body weight outcomes difficult.
The children in the summer-camp group had a numerically lower mean baseline BMI and BMI SDS than those in the lifestyle-school group. These random baseline imbalances22 were, however, taken into account and adjusted for by using mixed models for repeated measures.
There is currently no consensus as to which thresholds to use for clinically meaningful change in cardiovascular risk factors in childhood, but suggestions for the minimum BMI SDS loss required over 1 year in order to improve metabolic health have been in the range of 0.1–0.5.23–27 Although a large proportion of children in both treatment groups had a clinically significant reduction in BMI SDS (≥0.25–0.50), we are concerned that most children still had a BMI SDS above 2 (obesity) at follow-up (figure 3). The children included in our trial should on average have gained <2 kg to achieve a non-obese state during the 2-year study period (given their observed growth in height),10 as compared with the observed weight gain between 10 and 20 kg (table 2). Accordingly, the focus on healthy eating seems to have been insufficient, and we suggest that a more specific calorie restriction should be tested in future trials.6 ,28
Both the summer-camp treatment cost and the incremental cost versus lifestyle-school were high, compared with previously published treatment cost estimates.29 It is possible that repeated annual intensive summer camps could show more lasting effects, but of course this would be more expensive.
Strengths and limitations
The pragmatic randomised controlled design and the 2-year follow-up strengthen the generalisability of our findings, which might be applicable in similar public healthcare settings. Limitations include the predominance of European white children and the lack of data on socioeconomic status and adherence to the follow-up in the municipalities. Unfortunately, the expected calculated standardised effect size was too high, reducing the actual power of the study.
The cost perspective was limited since only treatment costs were calculated. A societal perspective including productivity costs related to parental work absenteeism would have provided relevant cost information. This study did not include measurement of self-motivation, although we acknowledge that the support of the group in the summer-camp intervention might have resulted in higher self-motivation than the lifestyle-school group.
Conclusion
Our findings indicate that, compared with an outpatient programme, a 2-year family camp-based obesity treatment programme has only small long-term effects on BMI and some cardiovascular risk factors in children with severe obesity. Furthermore, most children remained obese after treatment. It seems unlikely that the high summer-camp costs can be justified given the modest effects.
Acknowledgments
We are grateful for the contributions of all healthcare professionals involved at the four centres and all the children and parents who participated in this study. We particularly wish to thank the former leader of the MOC paediatric section, MD Martin Handeland, study nurse Åshild Skulstad-Hansen and bioengineer Berit Mossing Bjørkås. Finally, we thank Matthew McGee for proofreading the manuscript. Treatment in the Norwegian public healthcare system is nearly free of charge for patients. None of the funding parties had a role in design or conduct of the study; collection, management, analysis or interpretation of the data or preparation, review or approval of the manuscript.
References
Footnotes
Contributors BB carried out the initial analyses, drafted the initial manuscript, reviewed and revised the manuscript and approved the final manuscript as submitted. SL coordinated and supervised parts of the data collection at one of the outpatient clinics, reviewed and revised the manuscript and approved the final manuscript as submitted. MCS gave advice on the statistical analyses, carried out the statistical analyses performed in Stata, reviewed and revised the manuscript and approved the final manuscript as submitted. JKH gave advice on data preparation, contributed to discussion, reviewed and revised the manuscript and approved the final manuscript as submitted. VH carried out the health economic analyses, drafted the health economic parts of the initial manuscript, reviewed and revised the manuscript and approved the final manuscript as submitted. RAØ designed the study and wrote the protocol, coordinated and supervised data collection at one of the outpatient clinics, reviewed and revised the manuscript and approved the final manuscript as submitted. JH designed the study and wrote the protocol, reviewed the initial manuscript, reviewed and revised the manuscript and approved the final manuscript as submitted. All authors approved the final manuscript as submitted and are accountable for all aspects of the work.
Funding Research relating to this article was funded by the Norwegian Ministry of Health and Care Services, the Norwegian Foundation for Health and Rehabilitation and GjensidigeStiftelsen. BB has been funded by a public research grant from the South-Eastern Norway Regional Health Authority.
Competing interests None declared.
Ethics approval The Regional Committee for Medical and Health Research Ethics; South-Eastern Norway (2009/176).
Provenance and peer review Not commissioned; externally peer reviewed.