Article Text

Abstract
Objective To determine the proportion of children and young people (CYP) in England who are readmitted for the same condition.
Design Retrospective cohort study.
Setting National administrative hospital data (Hospital Episode Statistics).
Participants CYP (0-year-olds to 24-year-olds) discharged after an emergency admission to the National Health Service in England in 2009/2010.
Main outcome measures Coded primary diagnosis classified in six broad groups indicating reason for admission (infection, chronic condition, injury, perinatal related or pregnancy related, sign or symptom or other). We grouped readmissions as ≤30 days or between 31 days and 2 years after the index discharge. We used multivariable logistic regression to determine factors at the index admission that were predictive of readmission within 30 days.
Results 9% of CYP were readmitted within 30 days. Half of the 30-day readmissions and 40% of the recurrent admissions between 30 days and 2 years had the same primary diagnosis group as the original admission. These proportions were consistent across age, sex and diagnostic groups, except for infants and young women with pregnancy-related problems (15–24 years) who were more likely to be readmitted for the same primary diagnostic group. CYP with underlying chronic conditions were readmitted within 30 days twice as often (OR: 1.93, 95% CI 1.89 to 1.99) compared with CYP without chronic conditions.
Conclusions Financial penalties for readmission are expected to incentivise more effective care of the original problem, thereby avoiding readmission. Our findings, that half of children come back with different problems, do not support this presumption.
- Adolescent Health
- Epidemiology
- Health services research
Statistics from Altmetric.com
What is already known on this topic
In children and young people (CYP), recurrent admissions make up 41% of emergency admissions and 66% of bed days over a 2-year period.
The UK government has implemented financial incentives to decrease the number of 30-day readmissions as these are deemed to be avoidable failures of hospital care.
Research in adults found that 30%–50% of 30-day readmissions (depending on indication on index admission) were for a different primary diagnosis from the original admission.
What this study adds
Half the CYP who were readmitted within 30 days came back with a different primary diagnosis.
Emergency readmissions within 30 days occurred in 16% of patients with underlying chronic conditions, compared with 8% of patients without chronic conditions.
Our findings do not support the presumption that financial penalties for readmission incentivise more effective care of the original problem.
Background
A large proportion (32%) of children and young people (CYP) who have an emergency hospital admission will have at least one further emergency admission during the next 2 years.1 One in four of these patients are readmitted within 30 days of discharge.
Reimbursements for emergency readmissions within 30 days of discharge are restricted in the English National Health Service (NHS). The rule applies to all patients older than 4 years of age and was introduced in 2011/2012 to “encourage providers and commissioners to manage emergency admissions better through well-planned discharges, participation in preventative initiatives, and greater involvement of experienced clinicians earlier in the decision-making process”.2 Evidence from the USA shows that adult patients come back with different diagnoses, suggesting that not all readmissions might be preventable.3–5 A UK study of adults found similar results and deemed only 30% of readmissions to be potentially preventable.6
Previous studies focused on adult populations,7 hospital factors5 ,8 or specific conditions9–11 and therefore have limited applicability to hospital care for CYP.
We aimed to evaluate the hypothesis underlying the 30-day readmission rule that readmissions are often for the original problem, focusing on CYP. We assessed the proportion of CYP readmitted for the same problem within 30 days of discharge from a previous emergency admission.
Methods
Data source
We performed a retrospective cohort study using hospital administrative data for all inpatient admissions to NHS hospitals in England (Hospital Episode Statistics (HES)).12
Population
We defined a cohort of CYP who were discharged from an emergency hospital admission between 1 April 2009 and 31 March 2010, the year before the readmission rule was introduced, when they were 0 years old to 24-years old, and used the HES-ID unique patient identifier to track subsequent emergency readmissions over the next 2 years.13 For details on how we defined admissions, see online supplementary appendix B and previous reports.1 ,14
Supplementary appendix A
Supplementary appendix B
We extracted patient characteristics, including age group (<1 year, 1–4 years, 5–15 years and 16–24 years), ethnicity15 and area-level deprivation (measured by quintile of the index of multiple deprivation, IMD 200416 ,17), at index admission, or if missing, from any admission between 2009 and 2011. We classified all patients with a valid Code of General Practice (GP) practice as registered with a GP. If variables differed between admissions, we used the mode.
We excluded CYP who had missing information on sex (1410, 0.2%), IMD (13 027, 1.5%) or ethnicity (71 446, 8.3%) as these children were less likely to be linked longitudinally via their HES-ID. CYP with missing data could receive a different HES-ID on readmission, leading to missed matches. In the absence of patient identifiers, it is not possible to detect these patients.18 As missing data often occurred in multiple variables, we excluded 72 542 CYP in total (8.4%)
Primary diagnosis at admission
We used the primary diagnosis of the first (and in most cases the only) finished consultant episode recorded during the admission to indicate the clinical reason for the index admission. The primary diagnosis is determined and entered by professional NHS coders after discharge and is defined as the main condition treated or investigated during the relevant episode of healthcare.19 For statistical analysis, we defined six broad groups of International Classification of Diseases, version 10 (ICD-10) diagnostic codes recorded in the primary diagnosis: infection,20 chronic condition,14 injury,21 pregnancy related or perinatal related,1 sign or symptom (ICD-10 chapter 18) or other for all residual diagnoses. To determine the impact of the grouping of codes, we also grouped the primary diagnosis by 23 ICD-10 chapters (codes for groupings are listed in online supplementary appendix B).
Analysis
We stratified analyses by age group. We determined the proportion of patients who had an emergency readmission within 30 days or between 31 days and 2 years of the date of discharge of the index admission discharge, for whom the primary diagnosis was in the same group of ICD-10 codes (ie, same of six groups or ICD-10 chapters) at both the index admission and the recurrent admission. We only used the first recurrent admission, resulting in mutually exclusive 30-day readmission/<2-year recurrent admission groups. To limit the risk of disclosure, we only included the 10 most commonly recorded ICD-10 chapters for each age group, grouping the remainder of primary diagnosis groups in an ‘other’ category.
We used logistic regression to identify patient characteristics associated with 30-day readmissions, using information available on index admission (sex, age, indication, ethnicity, IMD quintile, underlying chronic conditions and GP registration). We determined underlying chronic conditions by assessing inclusion of codes for chronic conditions14 in any diagnosis code entered during an admission in the previous year (2008/2009). We did not include this variable for infants. We compared CYP who had a 30-day readmission with CYP who had no recurrent admission or a recurrent admission later than 30 days after index admission discharge. We used robust SEs for parameter estimates to correct for clustering by hospital.
We conducted a sensitivity analysis to determine whether the proportion of readmissions with diagnostic codes from a different group diminished when all 20 diagnostic fields (the mean number recorded is 2.9 diagnosis codes, SD: 2.2) were considered at the index admission.
All analyses were performed using Stata SE V.13.0. The interactive bipartite graphs were created using D3 block #9796212.22 The TreeMap was created using Google Charts.
Results
We included 866 221 children with at least one emergency admission. Emergency readmissions occurred within 30 days of discharge for 76 234 CYP (8.8% of index admissions) and between 30 days and 2 years for 193 988 CYP (22.4% of index admissions).
The primary diagnosis at index emergency admission varied by age (figure 1). Infections accounted for half of the primary diagnoses in infants and children aged 1–4 years. The prevalence of injury admissions increased with age.

Primary diagnosis at first emergency admission in 2009.
Fifty per cent (infants) to 60% (16-year-olds to 24-year-olds) of CYP who were readmitted within 30 days after index discharge had a primary diagnosis from the same broad coding group on both index and readmission (table 1). For later recurrent admissions, 35%–40% had a similar primary diagnosis. Similar results were found for the code groupings by ICD-10 chapter.
Proportion of recurrent admissions that have the same primary diagnosis as the index admission
Proportions of readmissions for the same primary diagnosis group as the index admission were similar to the overall findings (figure 2, see online supplementary appendix C). Young children (<1 year and 1–4 years) who had infection were more likely to come back with the same problem than was the case for other conditions (72% and 74%, respectively). Young women who had a pregnancy-related primary diagnosis at index admission came back with the same problem in 88% of 30-day readmissions.
Supplementary appendix C

Primary diagnosis at index and readmission for infants (six broad groups). Small numbers (<10 patients) were rounded up to 10 to preserve patient anonymity.
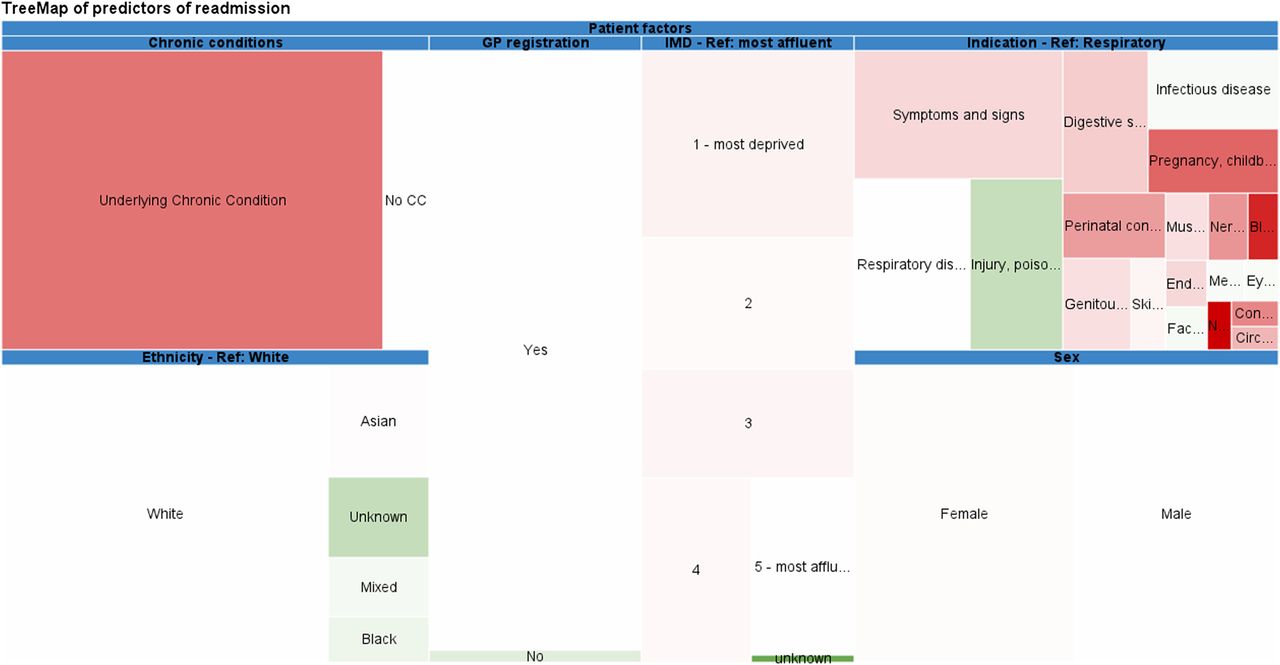
Readmission within 30 days was more likely in CYP with underlying chronic conditions (OR: 1.93, 95% CI 1.89 to 1.99, figure 3 and eTable 2 in online supplementary appendix A), girls (OR: 1.04, 95% CI 1.02 to 1.05) and more deprived CYP (most deprived compared with least deprived, OR: 1.06, 95% CI 1.03 to 1.09, eTable 2 in online supplementary appendix A). Readmission was less likely in CYP who were not registered with a GP (OR: 0.88, 95% CI 0.84 to 0.93) or had unstated ethnicity (OR: 0.60, 95% CI 0.55 to 0.63). Similarly, CYP with missing data on IMD or ethnicity were less likely to be readmitted (data not shown).

{kind=link}
{kind=link}
{kind=link}
TreeMap of predictors of 30-day readmissions—size reflects prevalence of different patient factors, colour represents estimated effect size of risk factors that increase (red) or decrease (green) the likelihood of readmission, calculated using multivariable logistic regression. Details on prevalence (eTable 1) and effect size (eTable 2) are available in online supplementary appendices (Interactive version—bit.ly/treemap_readmission). CC, chronic conditions; IMD, index of multiple deprivation.
For infants, chronic conditions were the strongest predictor for 30-day readmissions among the six primary diagnosis groups (OR: 3.31, 95% CI 2.96 to 3.71), while overall perinatal-related/pregnancy-related primary diagnoses were the strongest predictor (OR: 3.02, 95% CI 2.92 to 3.11). Admissions with injury-related primary diagnoses were least likely to result in a 30-day readmission across all age groups. Overall, effect estimates were consistent across age groups, apart from sex which was reversed in infants and children aged 1–4 years where girls were less likely to have a readmission (OR: 0.88, 95% CI 0.85 to 0.90 and OR: 0.96, 95% CI 0.93 to 1.00, respectively).
Sensitivity analysis
When all diagnostic fields were included for the index admission, the rates of recurrent admissions with the same indication as index admission increased to 71%–77% for <30-day readmissions and 49%–56% for later recurrent admissions for the broad groupings. For groupings by ICD-10 chapter, the proportion of readmissions with similar primary diagnoses increased to 59%–70% for <30-day readmissions and to 28%–42% for later recurrent admissions (ranges reflect different age groups, eTable 3 in online supplementary appendix A).
Discussion
Overall, 8.8% of CYP who had an emergency hospital admission between 1 April 2009 and 31 March 2010 were readmitted within 30 days. CYP with an emergency readmission had the same primary diagnosis at readmission and index admission in 50%–60% of 30-day readmissions (infants and 16-year-olds to 24-year-olds, respectively). In recurrent admissions that happen between 30 days and 2 years after index admission discharge, 35%–40% of CYP had the same primary diagnosis.
We found that children aged 1–4 years were less likely than older children to have readmissions for the same indication as index admission, supporting the exemption from the 30-day readmission rule for children up to age 4 years. However, the difference with older age groups was small. This suggests that extending the age exemption to older age groups or abolishing the penalty tariff would not have a significant effect on the number of readmissions for similar diagnoses.
Our findings are consistent with studies in adults: in a US study using Medicare data on patients aged 65 years and older, only 40%–50% of patients had a similar indication on readmission compared with their index admission.23 In addition, two US studies found that rates of readmission varied by condition, with rates ranging from 21% to 86%.7 ,24 The latter estimate is closer to our estimate of 66%–75% when considering all diagnoses recorded at index admission.
A UK study on readmission found that 30% of readmissions were broadly related to the previous admission.6 Their estimate is likely lower than our finding of 50% as they also included elective index admissions and used a different classification method.
Several studies have found increases in readmission rates associated with children with chronic conditions:25 ,26 a US study found that patient had chronic conditions in 78% of readmissions.27
Strengths and limitations
We found that CYP who had missing data on ethnicity and/or IMD were less likely to be readmitted compared with CYP without missing data on these variables. This may be associated with incomplete or erroneous identifiers, thereby reducing the chance of linkage to a subsequent admission.16 ,28
Our results are likely to overestimate the proportion of CYP who are readmitted with the same problem because of our relatively broad groupings and hospital coding practices. For instance, patients who have been admitted with an infection as a primary diagnosis on original and readmission are classified as having the same problem, while in fact they could have had two unrelated infections (eg, an urinary tract infection and a lower respiratory tract infection). Although we expect this limitation to affect the grouping by ICD-10 chapter to a lesser extent, it could still apply (eg, admissions for acute tonsillitis (J03) and asthma (J45) which would both be classified as diseases of the respiratory system).
In addition, we performed sensitivity analyses where we included all diagnoses entered during index admission. However, our results were very similar, indicating that readmissions are often for reasons not recorded on index admission, either as primary or subsidiary diagnosis.
Coding from a previous admission could have influenced primary diagnosis code entry at a subsequent readmission as hospital coders often have access to information from previous hospital visits or the full medical record upon data entry (personal communication with University College London Hospital clinical coding department). As financial reimbursements favour certain high tariff diagnoses, coders could favour similar primary diagnosis codes that attract high tariffs, for instance, in patients with chronic conditions. Similarly, if coders are aware of the rules for readmission penalties, this could influence coded diagnoses. However, there are strict rules in order to ensure consistent and fair coding.
In addition, our sensitivity analysis, where we included all diagnoses codes recorded on index admission rather than just the primary diagnoses, showed similar results to the main results, although with slightly higher proportions of similar diagnoses. This strengthens our overall finding and suggests that hospitals do not ‘game’ readmission reimbursements by entering similar primary diagnoses for both the index and subsequent readmissions.
Due to the nature of HES data, we were unable to determine whether children were admitted to paediatric wards or observation units.
Finally, we have limited our analyses to emergency admissions and first readmissions, excluding CYP who had elective index admissions or multiple readmissions, as this was beyond the scope of this paper.
Policy context
Policy makers need to balance potential benefits and harms of using tariffs to disincentivise hospital readmissions. The NHS England engagement documents for the 2015/2016 National Tariff announced that they will review the 30-day readmission penalty (as well as the marginal rate rule, which sets a baseline level of emergency admissions above which providers are paid 30% of the national price for admissions) for subsequent years.29 The NHS in England is one of many healthcare systems to use tariffs to disincentivise hospital readmissions. Our results suggest that reduction in payments for readmissions may penalise provision of care which is not directly amenable to intervention during the index admission. However, further research on more recent data after the introduction of this rule is needed to confirm this. In addition, these penalties may impact most on children with chronic conditions. Our findings likely reflect the variety of health problems occurring in children, although further evaluation is needed in non-NHS settings.
Implications for policy and practice
Our findings, that around half of readmissions are for a different condition, suggest that indiscriminate penalties for all readmissions are poorly supported by evidence. The variation in proportion of readmissions that occur for the same reason as on index admission across different conditions found in various studies further suggests the evidence available does not support unselective policy measures. For healthcare providers, the findings suggest that services need to address holistic care needs in addition to the problem at the index admission to reduce the frequency and severity of subsequent episodes of ill health. However, whether more effective and holistic care should be measured in terms of reduced (re)admissions or should be delivered in the community or hospital is far from certain. Undoubtedly, reduced readmissions reduce healthcare costs but are not clearly linked to improved quality of care in children.30 There is also a lack of evidence for effective interventions to reduce readmissions.31 A recent systematic review on interventions to reduce 30-day readmissions identified 43 studies testing various predischarge and postdischarge interventions as well as interventions that bridged the transition from hospital to primary care, none of which were consistently associated with a reduced risk for 30-day readmissions.32 This review excluded studies involving children. A few interventions aimed at CYP,33 such as structured discharge procedures for asthmatic children,34 clinical pathways for infants with bronchiolitis35 or a transition care programme for young adults with type 1 diabetes,36 have achieved reductions in readmission rates. However, these interventions included small patient groups and have limited reproducibility.37
Given the uncertain evidence, policy makers should prioritise evaluation of the 30-day readmission rule and reconsider disincentivising hospital readmissions until the benefits of the policy can be established.
Acknowledgments
We would like to thank members of the Policy Research Unit for the health of children, young people and families: Terence Stephenson, Catherine Law, Amanda Edwards, Steve Morris, Helen Roberts, Cathy Street, Russell Viner and Miranda Wolpert.
References
Supplementary materials
Interactive Figure
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter Follow Linda Wijlaars at @epi_counts Pia Hardelid (@PHardelid), Ronny Cheung (@CheungRonny), Jenny Woodman (@jlwoodman1)
Contributors RG and LPMMW conceived the paper and the statistical analysis plan. LPMMW cleaned and analysed the data, and drafted and revised the paper. RG acquired the data and is guarantor. PH contributed to the design of the study, interpretation of results and revised the paper. JW, JA and RC helped interpret the data and revised the paper. All authors commented on the analyses and report, and read and approved the final manuscript.
Funding LPMMW and JW were supported by funding from the Department of Health Policy Research Programme through funding to the Policy Research Unit in the Health of Children, Young People and Families (grant reference number 109/0001). This is an independent report commissioned and funded by the Department of Health. The views expressed are not necessarily those of the Department. We also acknowledge the support from the Farr Institute of Health Informatics Research (MRC Grant Nos: London MR/K006584/1).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional data can be accessed in the online supplementary appendices. Source data can be accessed by researchers applying to the Health and Social Care Information Centre for England. Copyright © 2015, Reused with the permission of the Health and Social Care Information Centre. All rights reserved.