Article Text

Abstract
Background Sudden cardiac death is the most common cause of mortality in young athletes. In some of these, the final pathway is arrhythmia. The authors aimed to identify the incidence, diagnosis and management of athletes undergoing investigation and intervention for cardiac arrhythmias.
Methods Retrospective analysis of all patients between 10 and 17 years presenting to a supra-regional paediatric cardiac unit for investigation and intervention for a cardiac arrhythmia. Elite athletes (county and national level) were identified from the departmental clinical and arrhythmia databases (October 1997–2007). Patients with significant congenital heart disease were excluded.
Results From 657 patients undergoing 680 interventions, 324 were excluded. From the remaining 333 we identified 11 elite athletes – football (n=3), martial arts (n=2), rugby (n=2), triple jump, netball, canoeing, and motor sport (n=1). Presenting symptoms included palpitations (n=8) and syncope (n=1). Two were asymptomatic and investigated following routine screening. Diagnoses included atrioventricular (AV) re-entry tachycardia (n=3), AV node re-entry tachycardia (n=4), complete heart block (n=1), sinus node dysfunction (n=1), vasovagal syncope (n=1) and pre-excited atrial fibrillation (n=1). Arrhythmia interventions included implantable loop recorder (n=2), diagnostic electrophysiology study (n=9), including radiofrequency ablation (n=5), cryoablation (n=2) and pacemaker implantation (n=2). Following intervention, 10 children returned to competitive sport. There were no deaths. No child required long-term medication post-intervention.
Conclusion Of the young competitive athletes identified from the authors' study, there was a high incidence of significant arrhythmias. Intervention is usually successful and most athletes return to elite sport without the need for long-term medication.
Statistics from Altmetric.com
Introduction
Although sudden cardiac death (SCD) in young athletes is highly publicised, it is a rare event with an estimated incidence of 1–3 per 100 000 person years.1 Cardiac screening to identify those at risk has gained acceptance in some countries, in particular Italy, and recent reports have demonstrated this is associated with a 90% reduction in athlete mortality from SCD suggesting that many deaths may be preventable.1,–,6 Management is dependent on the underlying condition, but many will be excluded from competitive sport.7,–,9 In the UK there is no national cardiac screening programme for young athletes. This may be due to the perception that current screening protocols have poor sensitivity and that more elaborate screening programmes are cost prohibitive.10,–,12 However, due to the steady increase in the number of SCDs among high-profile athletes,13,–,17 many medical and sporting governing bodies recommend preparticipation cardiovascular screening in athletes under 35 years of age.1 5 13 18,–,20 At a time when childhood obesity is common and increased childhood exercise is being promoted,7 it is relevant to consider whether the diagnosis of a cardiac abnormality in a child athlete will result in inevitable exclusion from sport.21
What is already known on this topic
▶ Sudden cardiac death (SCD) is the most common cause of death among young athletes.
▶ Identification of cardiac disease by screening programmes has been shown to decrease the incidence of SCD in young athletes.
▶ Interventional treatment of potentially dangerous cardiac arrhythmias is well established in the UK.
What this study adds
▶ Interventional treatment of some potentially lethal arrhythmias in young elite athletes can enable the majority to return to competitive sport.
▶ Successful intervention may allow athletes to return to sport without the need for long-term medication.
▶ Exclusion from sport is not necessary for all athletes with an identified cardiac arrhythmia.
Despite the popularity of cardiac screening programmes, few data have been published on the outcome of interventional treatments in elite child athletes presenting with cardiac symptoms. In this study, we have identified elite child athletes who have either presented with or who have been referred for investigation of ECG abnormalities or arrhythmia-like symptoms. We report on the management and outcome of these children with particular emphasis on return to competitive sport.
Patients and methods
Over the 10-year period from October 1997–2007, data were collected on all patients undergoing interventional investigation or treatment for arrhythmia-like symptoms at a single tertiary referral centre. Interventions included insertion of implantable loop recorders (ILRs), pacemaker insertion and electrophysiological study with or without ablation. Patient's age, presenting symptoms, diagnosis, medication, level of sport participation and arrhythmia intervention were extracted from the paediatric cardiac database (HeartSuite, Systeria, Glasgow, UK) and the patient's notes. From this cohort, patients were excluded on the basis of being outside the age bracket (10–18 years) or having known congenital heart disease, that is, haemodynamically significant intracardiac shunts or significant valvular stenosis or incompetence (figure 1) Elite athletes were defined as those competing at county or national level. This was a retrospective review carried out under the auspices of service evaluation. Data are expressed as median with ranges.

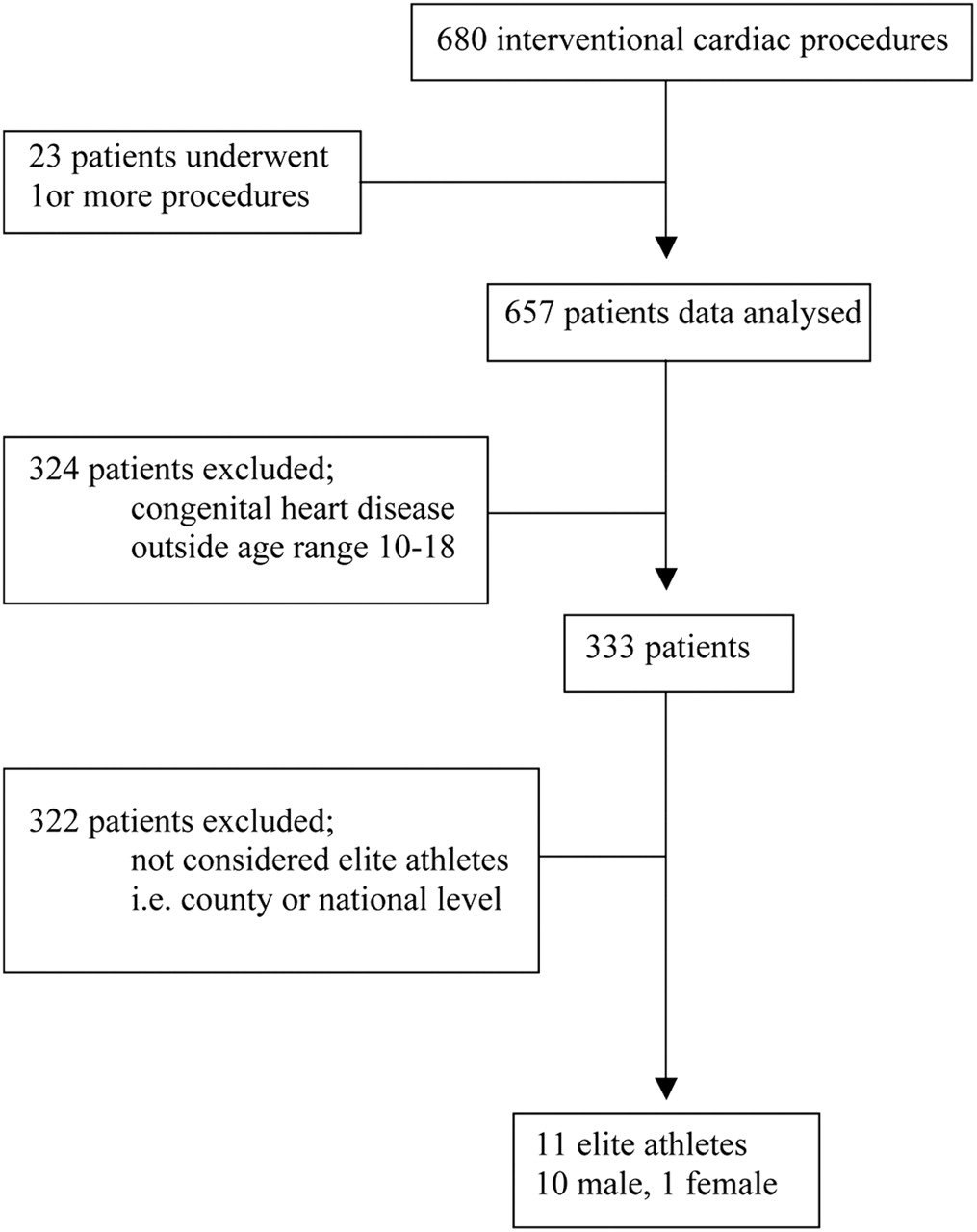{kind=link}
Identification of athletes from referred patient group.
Results
A total of 657 paediatric patients underwent 680 interventional procedures. We excluded 324 patients on the basis of exclusion criteria as described above. Of the remaining 333 patients, 11 were identified as elite athletes (table 1). The median age at first presentation was 14 years (10–17). The median period of symptoms prior to referral was 4 months (0.25–36). Eight patients presented with palpitations. Two patients were asymptomatic, presenting with bradycardia on club screening (n=1) and routine medical assessment for intercurrent illness (n=1). One patient presented for investigation of recurrent collapses. Six of the patients were treated with medication prior to intervention, including flecainide (n=5), atenolol (n=1) and verapamil (n=2). Diagnosis was made on nine patients prior to definitive intervention. These included atrioventricular (AV) nodal re-entry tachycardia (n=4), AV re-entry tachycardia (n=4) and complete heart block (n=1). One patient with recurrent collapse underwent insertion of an ILR. Diagnosis of vasovagal syncope was confirmed in this patient following exclusion of an arrhythmia during a symptomatic episode. Another patient with profound sinus bradycardia and suspected sinus node dysfunction had a normal electrophysiology study and was deemed to have high vagal tone due to intense physical conditioning. Other arrhythmia interventions included radiofrequency ablation (n=5), cryoablation (n=2) and pacemaker implantation (n=2). There was one significant procedural complication. This 12-year-old patient presented with pre-excited atrial fibrillation and Wolf Parkinson White (WPW) syndrome. He required insertion of a permanent pacemaker following ablation of a para-Hisian pathway. This was discussed preoperatively as risk of AV node damage was felt to be high due to the origin of the pathway. This needed to be balanced against the potential for sudden death with fast anterogradely conducting properties were the pathway not ablated.
The sports participated in, symptoms, medications, diagnosis and intervention of the elite athletes identified
At follow-up, no patient remained on medication. Ten of the 11 patients (91%) have returned to competition at elite level in their original sports with complete resolution of symptoms (table 1). This includes one patient who returned to competitive, long-distance canoeing despite pacemaker implantation (patient 8). The remaining patient still participates in non-contact sports after insertion of a pacemaker device. Median follow-up from procedure to March 2010 is 39 months (range 30–116). At follow-up, no patient had a recurrence of symptoms which precluded sports participation.
Discussion
This study has demonstrated that we can identify and treat significant arrhythmias in young athletes and enable the majority to return to competitive sport. One point six per cent of children referred to our centre for interventional arrhythmia assessment, were elite athletes. Of these, four patients (36%) had potentially lethal arrhythmias including WPW and complete heart block. Nine of the 11 athletes had frequent persistent cardiac symptoms, which would have undoubtedly prevented them from reaching their full athletic ability. Encouragingly, 91% returned to high-level sport after arrhythmia intervention. The only significant complication was complete heart block in one patient. This patient presented in pre-excited atrial fibrillation, a potentially lethal arrhythmia, prior to the availability of cryoablation in our unit. Since the inception of cryoablation, we have had no complications of postablation heart block in more than 500 procedures.
Between 40% and 80% of trained athletes have a minor abnormality found on their ECG, for example, sinus bradycardia, first degree AV block, early repolarisation, incomplete right bundle branch block and increased QRS voltages.2 5 9 10 13 21,–,24 In the majority, these represent normal variants or physiological adaptations of the trained heart. If these ECG findings are interpreted with regard to the athlete's age, gender, race, family history of cardiovascular disease and physical findings on examination, the percentage of athletes excluded for sport on the grounds of abnormal ECG changes can be decreased.16 21 25 During high-impact training athletes' hearts undergo physiological changes and cardiac remodelling, creating ECG and echocardiographic changes. The differentiation between an athlete's heart and pathological disease is essential to avoid inappropriate disqualification from sport. One patient in our study was found to have a resting heart rate of 40/min on club screening. In view of an associated history of dizzy spells, he underwent an electrophysiological study. This was normal and he has had no further symptoms. Asymptomatic sinus bradycardia, and sinus pauses are common in young athletes due to increased vagal tone. An incorrect diagnosis of sinus node dysfunction may have excluded this patient from competitive football.18
Where athlete's careers are involved, the decision to disqualify them on the basis of cardiac disease is complex and can prove difficult to implement.19 26 Elite athletes are highly motivated and may wish to accept the risks associated with competitive sport and resist prudent recommendations to withdraw.27 A number of papers, including most recently Papadakis and Sharma13 suggest that universal screening of athletes will lead to detection of potentially lethal cardiac disorders and result in withdrawal from athletic activity. Our report suggests that detection and appropriate treatment may, in certain conditions, allow return to sport. Our study did not include any patients with disorders such as arrhythmogenic right ventricular cardiomyopathy (ARVC) where return to sport is precluded.18 However, Bauce et al28 have shown that detailed further assessment is essential to distinguish ARVC from a normal athlete's heart adaptation. In addition, we excluded from analysis all patients with significant congenital heart disease. Decision-making in this cohort requires specific assessment of prognosis and published recommendations are available.29
Anderson and Vetter7 discuss the risk-benefit ratio of restricting a young athlete from physical activity. They conclude that most cardiac conditions leading to SCD have poorly defined risk factors and children and adolescents should be encouraged to lead healthy, active lifestyles. Although practitioners should use preparticipation screening guidelines recommended by sports organisations this may lead to defensive practice and a low threshold for advice to withdraw from sport. In this setting the cost-effectiveness and socioeconomic impact of screening must be considered. This was summarised by Wren11 who calculated that in a population of 100 000 school children, approximately 30 children may be at risk of sudden death. The basic screening of each 100 000 cohort would cost approximately eight million pounds with further costs incurred from the 2500–3000 children with abnormalities detected during the screening process. In most screening studies, the most common potentially dangerous cardiac diagnoses are hypertrophic cardiomyopathy and ARVC. However, most reports do not provide age-specific diagnoses and include both adolescents and young adults. It is possible that an analysis of adolescents alone would demonstrate a different diagnostic profile. As shown in our study, these athletes are more likely to be male and we know that SCD is 5–9 times more common in males. This suggests that it may be more efficient to introduce gender-specific screening programmes. At a time when the incidence of morbidly obese children is rising, we need to be careful that fear of cardiovascular catastrophe does not deter children from exercising.30 Although this paper does not address the complex ethical, epidemiological and medical issues of child athlete screening, it does demonstrate that most child athletes who present with cardiological symptoms suggestive of a cardiac arrhythmia, have an excellent chance of undergoing effective treatment and returning to elite sport.
Conclusion
Of the young, elite athletes identified from our study (1.6% of children referred for interventional assessment), there was a high incidence of potentially dangerous arrhythmias. Cardiac intervention was usually successful and most athletes returned to elite sport without the need for long-term medication.
References
Footnotes
-
Funding This work was funded internally from departmental resources.
-
Competing interests AGS is Medical Director of Sports Cardiology UK (http://www.sportscardiology.co.uk) a company which specialises in the cardiological assessment of athletes. No other author has any competing interests.
-
Provenance and peer review Not commissioned; externally peer reviewed.