Article Text

Abstract
Objective Liquid medicines are easy to swallow. However, they may have disadvantages, such as a bad taste or refrigerated storage conditions. These disadvantages may be avoided by the use of oral solid medicines, such as powders or tablets. The aim of this study was to investigate the acceptability of and preference among four oral formulations in domiciliary infants and preschool children in The Netherlands.
Methods Parents administered four oral placebo dosage forms that were aimed at a neutral taste, at home, to their child (1–4 years of age) twice on one day following a randomised cross-over design: small (4 mm) tablet, powder, suspension and syrup. They were asked to report the child's acceptability by a score on a 10 cm visual analogue scale (VAS score) and by the result of the intake. At the end of the study, they were asked to report the preference of the child and themselves.
Results 183 children were included and 148 children were evaluated. The data revealed a period/cross-over effect. The estimate of the mean VAS score was significantly higher for the tablet than for the suspension (tablet 9.39/9.01; powder 8.84/8.20, suspension 8.26/7.90, syrup 8.35/8.19; data day 1/all days). The estimate of the mean number of intakes fully swallowed was significantly higher for the tablet than for the other formulations (all p values <0.05). Children and parents preferred the tablet and syrup over the suspension and the suspension over the powder (all p values <0.05).
Conclusions All formulations were well accepted. The tablets were the best accepted formulation; the tablets and syrup the most preferred.
Trial Registration number ISRCTN63138435.
- Child
- Parent
- Patient Acceptance
- Medicine
- Dosage Form
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
What is already known on this subject
-
Oral medicines are frequently administered to infants and preschool children as a liquid formulation.
-
Liquid formulations may have disadvantages, such as a bad taste or refrigerated storage conditions.
-
Small tablets can be used to administer medicines to young children.
What this study adds
-
Minitablets (4 mm diameter) were the most acceptable formulation to healthy Dutch infants and preschool children.
-
Both parents and children preferred the minitablets and syrups to the suspensions and powders.
Introduction
For decades, oral liquid dosage forms, such as syrups and suspensions, have been considered as the favourable type of dosage form in which to administer medicines to young children.1 ,2 However, oral liquid medicines may have disadvantages, such as a bad taste, portability problems or refrigerated storage conditions.3–6 Therefore, WHO currently favours that young children, particularly in developing countries, be treated with oral solid medicines.7
Oral liquid medicines are more commonly available for use in infants and preschool children than oral solid (flexible) medicines, such as powders or orodispersible tablets.8 Small-sized tablets, also referred to as minitablets, have been identified as a new type of oral solid dosage form in which to administer medicines to young children. However, only few of such tablets have been authorised for children below 4 years of age.3 ,6 ,9–11 Nevertheless, small tablets have been widely used in this age group as food supplements, for example, 4 mm sodium fluoride tablets for caries prevention, or 4 mm vitamin AD tablets.12–16
The selection of an oral dosage form and the pharmaceutical aspects of the formulation, such as the palatability of an oral suspension or the size of a tablet, are important factors in the overall acceptability of an oral paediatric medicine.6 ,10 As adequate child and parent acceptability are prerequisites for good drug adherence, paediatric treatment outcomes may be enhanced by a careful selection of the formulation including the type of the dosage form. Therefore, the aim of this study was to investigate the acceptability of and preference among four oral formulations in domiciliary, infants and preschool children in The Netherlands.
Methods
Study design
A randomised cross-over trial was performed in six Dutch preschool preventive healthcare clinics in Beusichem, Beesd, Culemborg (2 clinics), Maurik and Zaltbommel. Ethical approval was waived by the Central Committee on Research involving human subjects (CCMO) on basis of the Dutch Medical Research Involving Human Subjects Act (WMO). Approval was obtained from the Institutional Review Board of the Utrecht Institute for Pharmaceutical Sciences (UIPS).
Setting and study participation
The aim of the preschool preventive healthcare clinics is to monitor the mental and physical development of children between 0 and 4 years of age, to advise parents on child-raising issues and to vaccinate children.17 The response rate to the invitation for an appointment is over 99% of children below 2 years of age and over 90% of children between 2 and 4 years of age.18
Parents were verbally approached by one of four recruiters (a licensed pharmacist and three graduate students) when attending the clinics in 2011. Parents had either received the written information by mail 2 weeks before the appointment, or this information was handed to them at the end of the face-to-face contact. Parents were asked or called by phone for written informed consent and study participation at least 2 weeks after the written information was provided. The results of the selection process were systematically gathered (date when verbally approached, healthcare clinic, recruiter, date of birth, child gender, willingness to participate, reason for exclusion if mentioned voluntarily).
Children were eligible for inclusion in this study if they were between 1 and 4 years of age and if their parents had mastery of the Dutch language. Exclusion criteria were: (1) significant developmental delay; (2) having swallowing difficulties, an eating disorder or a chronic condition requiring oral medication; (3) hypersensitive to lactose, having cow-milk allergy or having an allergy of unknown origin; (4) a member of staff of the preventive healthcare clinic considered that study participation was inappropriate in view of the family situation. During the study, the criterion added was (5) according to the parents’ observation, children should not feel ill when the formulations were actually given.
Intervention
Parents were asked to administer four oral placebo formulations to their child at home during normal family routines. They were asked to administer the formulations (4 mm tablet, powder, suspension and syrup) in the same way they would administer a prescribed medicine, however, without any physical or physiological pressure (table 1). In conformity with common Dutch dispensing procedures for immediate release formulations, chewing and coadministration/mixing with food or drinks was neither recommended nor forbidden. Parents were instructed to administer the formulations on four consecutive days; however, they were allowed to skip a day if necessary. In order to study any period or carry-over effect, the formulations should be given in a predefined, randomised order, and each formulation twice on 1 day only. The formulations were specifically developed and manufactured for this study by ACE Pharmaceuticals, The Netherlands.
Characteristics of four different oral formulations
Outcomes
Acceptability after each administration: (1) visual analogue scale (VAS) score for child acceptability according to the parents’ observation (0–10 cm VAS scale; from 0 ‘heel erg vervelend’ (very unpleasant/bothersome etc), to 10 ‘helemaal niet vervelend’ (not at all unpleasant/bothersome etc) and (2) result of the intake according to the parents’ observation (full dose swallowed, parts of the dose swallowed, dose not swallowed). If parents indicated that they had forgotten to administer the formulation to the child, then the absent VAS scores and absent values for the result of the intake were considered ‘missing values’. If parents indicated that they had not administered the formulation to the child for any other reason, then the absent VAS scores were set at ‘0’ and the absent results of the intake at ‘not swallowed’.
Preference at the end of the study: (1) the single most preferred formulation of the child according to the parents’ observation; (2) the single most preferred formulation of the parents for the child.
Others: Questions concerning other family characteristics and the exact manner the formulations were administered to the child.
Sample size
The sample size for acceptability was calculated on basis of a design aimed at detecting a specified difference between the VAS scores of two treatments in a cross-over trial involving four oral formulations on four different days.19 The power was set at 0.8 and the significance level at 0.05. Due to a lack of relevant data from the literature on the acceptability of oral formulations in (young) children, the sample size calculations were based on plausible values for the mean difference and SD of the VAS scores. The sample size for preference was calculated on basis of a statistical design where parents were asked to identify the single most preferred formulation. The same approach was applied as for the calculation of the acceptability. The sample size was set at 150 evaluable children, which would, in most cases, allow a maximum difference of 2 for acceptability and 0.2 for preference to be detected.
Randomisation
The study was randomised for the order of administration of the formulations by an RIVM employee who was not involved in this study. Randomisation was conducted with a random sequence obtained from http://www.random.org. The same sequence was applied to each block of 24 children. Siblings were allocated to the same order to avoid mistakes.
Data analysis
The following analyses were conducted: (1) assessment of systematic differences between the two single VAS scores for a particular formulation (paired Z tests); (2) in case of no significant differences, calculation of the mean VAS scores per child and formulation; (3) evaluation of a potential cross-over or period effect (Z test on the order of the best accepted formulation), in case of such an effect analysis 3 and 4 were done for the administrations of the first formulation only (day 1) and for all data (all 4 days); (4) estimation of the mean VAS score per formulation and computation of the corresponding 95% CIs (Z statistics); (5) testing of differences between the mean VAS scores of two different formulations (Wilcoxon and Mann–Whitney tests); (6) estimation of the mean number of intakes that were fully swallowed by a child per formulation and computation of the corresponding 95% CIs (Z statistics); (7) computation of estimates and associated 95% CIs of the probabilities that the child and parents preferred a particular formulation, and comparison between the four probabilities (Z tests).
All statistics were conducted applying Excel 2007 (Microsoft, Redmond, Washington), R V.2.13 (R development core team).
Results
Setting and study participation
Between February and July 2011, 421 children from 373 families were verbally approached; 405 children from 358 families were eligible for inclusion if their parents would pass the language check. Informed consent was obtained for 183 children from 153 families. Diaries including information on the acceptability and preference of the formulations were returned for 151 children from 124 families (recruitment success rate 45%, loss to follow-up 17%). Three diaries from two families could not be used in the data analysis because it was not clear in which order the formulations were administered (figures 1 and 2). The recruitment success rate in the population eligible for inclusion was similar among all the participating healthcare clinics and recruiters. The age and gender of the children eligible for evaluation were not statistically different from the children eligible for inclusion.
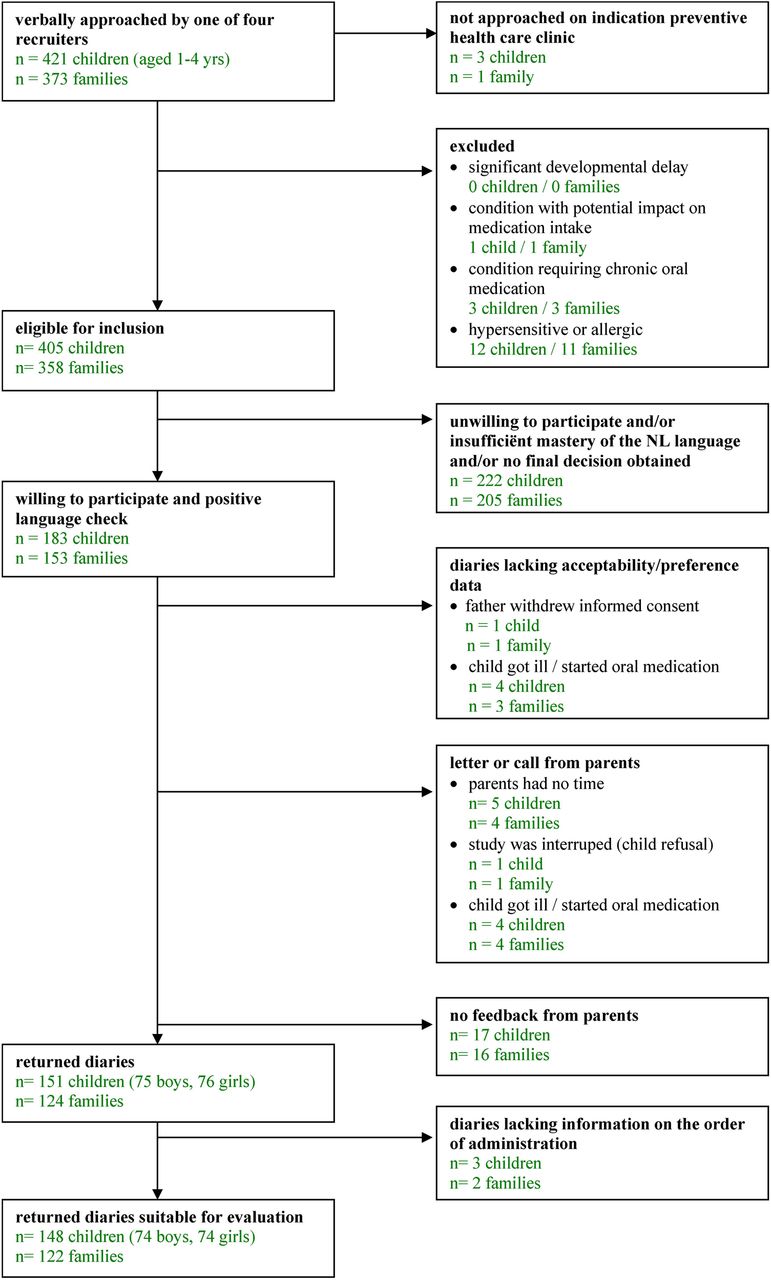
Participant flow through the study.

{kind=link}
{kind=link}
Visual analogue scale to report the child acceptability example shown for the powder.
Child and parent acceptability
The data did not indicate systematic differences between the single VAS scores of the two administrations of each formulation to a child. Therefore, the mean VAS scores were used for the further evaluations. The VAS score data indicated a period or cross-over effect by which formulations administered earlier tended to have somewhat higher scores (p value <0.0001). As a consequence, analysis started with the data of the first day only. The estimates of the mean VAS scores of the first day were: tablet 9.39 (32 children); powder 8.84 (45 children); suspension 8.26 (34 children) and 8.35 syrup (37 children); see table 2 for the CIs. The tablet scored better than the suspension even when applying a Bonferroni correction (p=0.001: for correction multiply by 6). The other comparisons were less clear, but there was an indication that the tablet scored better than the syrup as well as the powder.
Acceptability of four different oral formulations (n=148 children)
Using the data from all 4 days, estimates of mean scores per formulation were obtained across the 24 different orders of administrations, each order getting the same weight. Although no clear ranking was visible between the syrup, suspension and powder, the superiority of tablet over the other three forms was more evident than by considering the data from the first day only (table 2).
The estimate of the mean number of administrations that were fully swallowed were 1.96 (tablet), 1.58 (powder), 1.70 (suspension) and 1.67 (syrup) This number was significantly higher for the tablet than for the other formulations (p value <0.05) (table 2). The scatter-plot of the single VAS scores versus the result of the intake (data not shown) clearly illustrated that the VAS score was predictive for the result of the intake. No choking was reported.
Child and parent preference
Children and parents appeared to prefer the tablet and syrup over the suspension and the suspension over the powder (p values <0.001). There is also some indication (p value=0.082) that parents preferred the tablet to the syrup (table 3).
Preference of four different oral formulations (n=148 children)
Discussion
In this randomised cross-over trial, the four formulations investigated can all be considered well accepted by children between 1 and 4 years? The small 4 mm tablet was significantly better accepted than the suspension, and there was an indication that the tablet was also better accepted than the powder and syrup. The tablet was significantly more often fully swallowed than the other formulations. Children and parents preferred the tablet and syrup over the suspension, and the suspension over the powder.
Child acceptability of oral medicines has been studied for many years.20–22 Few studies however, have focussed on the acceptability of oral dosage forms as such. Ansah et al23 compared tablet with syrup formulations in 155 children from between birth and five years (of age) for the treatment of malaria, and Bagenda et al24 in 129 children from between 6 months and 12 years of age in case of treatment with highly active anti-retroviral therapy (HAART). Both teams concluded that the tablet formulations resulted in better adherence. Spomer et al3 compared 2 mm uncoated placebo tablets with a sweet syrup in 60 inpatient children aged from between 6 months and 6 years of age, and concluded that the acceptability of the tablet was at least as good as that of the syrup. Despite key differences in the patient population and methodology, the results of our study are consistent with those of the aforementioned authors.
Three studies have been identified on the child acceptability of small tablets.3 ,9 ,10 Apart from the study of Spomer et al,3 the study of Van de Vijver et al10 demonstrated that 2 mm medicated tablets were good to excellently swallowed by 16 outpatient Belgium or Dutch cystic fibrosis patients who were between 6 and 30 months of age. Thomson et al9 demonstrated that larger 3 mm tablets could be swallowed by 46 out of 100 inpatient British children who were 2 years old. Like the team of Spomer3 and Van de Vijver,10 we found good to excellent acceptance of the tablet, even though our tablets were of a larger size. When comparing our results with those of Thomson et al,9 we found a better acceptance of our 4 mm tablets. The reason for this difference is not known, but differences in tablet characteristics, setting, cultural and behavioural attitudes may be considered.11 ,25 ,26
This study is the first randomised cross-over trial investigating the child and parent acceptability of and preference among four oral placebo formulations in infants and preschool children. It is also the first study investigating the child acceptability of oral placebo formulations in a domiciliary rather than inpatient setting, with a double rather than single administration of each formulation, a 4 mm, rather than a 2 or 3 mm tablet, and with two different measuring instruments for child acceptability.
In this study, an indication was found that the mean VAS acceptability score of the tablet was higher than that of the syrup, and that the parents preferred the tablet over the syrup. However, when parents were asked to report the child's preference, no significant difference was found between the syrup and the tablet. Results such as ours provide an argument for the fact that child and parent acceptability and preferences are different outcomes providing complementary information on the suitability of a formulation. Preferably, these outcomes are investigated in the same study.
This study has some limitations. First, the administrations were not supervised by the research team as this would bias normal family routines. Consequently, the evaluation of the child acceptability and preference relied on parental reports. This self-reporting methodology was not validated prior to the start of the study. Therefore, recruiters focused heavily on adequate verbal instructions to the method of administration and reporting.
Second, child acceptability may be influenced by taste aspects. The powder and tablet were manufactured from the same blend, so their taste was identical. However, the taste of the suspension and syrup differed due to the intrinsic nature of these dosage forms. Therefore, it cannot be excluded that any differences in the acceptability and preference among the liquid formulations were also related to taste.
Third, the recruitment was tailored to healthy domiciliary children between 1 and 4 years of age and parent with mastery of the Dutch language. Hence, the applicability of our findings to children outside this population, for example, children who are feeling ill, who are otherwise fractious or who are from a foreign ethnicity is left for future research. In view of the findings of the teams of Ansah,23 Bagenda,24 and Spomer,3 it is anticipated that our study's findings will equally hold for older children.
Fourth, chewing was not evaluated as it is common practice in The Netherlands that children may chew on immediate release tablets if they want to. Therefore, the acceptability (swallowabilty) of tablets that should be taken as a whole, for example, monolithic extended release tablets or tablets with essential taste masking, is left for future research.
Fifth, we did not systematically evaluate the parents’ reasons to decline participation. However, from the voluntary reasons provided, it seemed that parents were mainly ‘too busy’ or having a second name suggesting a non-European ethnicity. It cannot be excluded that parents who did not participate in this study might be more reluctant to administer a particular formulation to their child than those who participated.
This study showed that the acceptability of 4 mm tablets is unlikely to be inferior as those of three currently employed dosage forms in infants and preschool children when aimed at a neutral taste. Thus, there is no reason to further question the acceptability of 4 mm immediate release tablets for children from the age of 1 year. Rather than discussing whether small tablets should be the preferred type of dosage form for the development of future paediatric medicines, pharmaceutical industries are recommended to consider the possibility of developing two essentially different dosage forms alongside each other.
Conclusion
Oral placebo 4 mm round uncoated tablets, powders, suspensions and syrups may be considered well accepted dosage forms in children between 1 and 4 years of age when aimed at a neutral taste. The tablets were significantly better accepted than the suspension, and there is an indication that they were also better accepted than the powder and syrup. Children and parents preferred the tablet and syrup over the suspension, and the suspension over the powder, but it was not clear whether they preferred the tablet over the syrup or otherwise. This study does not support the historic approach that medicines should normally be given to young children as an oral liquid formulation as other formulations may result in equivalent acceptability.
References
Footnotes
-
Contributors DAvRN: conceptualised and designed the study, coordinated the participant recruitment, coordinated the manufacture and dispensing of the placebo formulations, was responsible for the liaison with the statistician (JAF), drafted the initial manuscript and approved the final manuscript as submitted. BJdN: provided support in the design of the study towards the participant recruitment and questions in the participant diaries, was responsible for internal affairs at the preventive healthcare clinics, reviewed and revised the manuscript and approved the final manuscript as submitted. AFAMS: supervised the conceptualisation and design of the study, supervised the recruitment process and data collection, reviewed and revised the manuscript and approved the final manuscript as submitted. JAF: provided support in the design of the study towards the calculation of the sample size; he conducted the data analysis, reviewed and revised the manuscript and approved the manuscript as finally submitted. TCGE: supervised the conceptualisation and design of the study, supervised the recruitment process and data collection, reviewed and revised the manuscript and approved the final manuscript as submitted. CMAR: supervised the conceptualisation and design of the study, supervised the recruitment process and data collection, reviewed and revised the manuscript, and approved the final manuscript as submitted.
-
Funding The study was sponsored by a grant from the National Institute for Public Health and the Environment and the Medicines Evaluation Board in The Netherlands.
-
Disclaimer The opinions in this article are only those of the authors. This article is not intended to reflect the opinion of the Medicines Evaluation Board in the Netherlands (MEB) nor any of the working parties or scientific committees of the European Medicines Agency (EMA).
-
Competing interests Diana van Riet is coordinator/senior assessor at the department of chemical pharmaceutical assessment of the Medicines Evaluation Board in The Netherlands. She is vice chair of the European Medicines Agency's (EMAs) Quality Working Party. Alfred Schobben is a member of the MEB and expert for the EMA. Toine Egberts is also an expert for the EMA. No other conflicts of interest apply.
-
Ethics approval Not applicable. However, the protocol was approved by the Institutional Review Board of the Utrecht Institute for Pharmaceutical Sciences.
-
Provenance and peer review Not commissioned; externally peer reviewed.