Article Text

Abstract
Objectives Gut directed hypnotherapy (HT) is shown to be effective in adult functional abdominal pain (FAP) and irritable bowel syndrome (IBS) patients. We performed a systematic review to assess efficacy of HT in paediatric FAP/IBS patients.
Methods We searched Medline, Embase, PsychINFO, Cumulative Index to Nursing and Allied Health Literature databases and Cochrane Central Register of Controlled Trials for randomised controlled trials (RCT) in children with FAP or IBS, investigating efficacy of HT on the following outcomes: abdominal pain scores, quality of life, costs and school absenteeism.
Results Three RCT comparing HT to a control treatment were included with sample sizes ranging from 22 to 52 children. We refrained from statistical pooling because of low number of studies and many differences in design and outcomes. Two studies examined HT performed by a therapist, one examined HT through self-exercises on audio CD. All trials showed statistically significantly greater improvement in abdominal pain scores among children receiving HT. One trial reported beneficial effects sustained after 1 year of follow-up. One trial reported statistically significant improvement in quality of life in the HT group. Two trials reported significant reductions in school absenteeism after HT.
Conclusions Therapeutic effects of HT seem superior to standard medical care in children with FAP or IBS. It remains difficult to quantify exact benefits. The need for more high quality research is evident.
- Irritable Bowel Syndrome
- Functional Abdominal Pain
- Hypnosis
- Hypnotherapy
- Pediatrics
Statistics from Altmetric.com
What is already known on this topic?
-
Gut-directed hypnotherapy has been demonstrated to be effective in adult IBS patients who failed standard medical care and beneficial effects appear to be long lasting.
-
Data on the efficacy of gut-directed hypnotherapy in children and adolescents with IBS or FAP are lacking.
What this study adds?
-
This systematic review indicates that hypnotherapy is more effective than standard medical treatment in reducing symptoms in children with FAP or IBS.
Introduction
Functional abdominal pain (FAP) and irritable bowel syndrome (IBS) are characterised by chronic or recurrent abdominal pain without evidence of any underlying organic disorder. By definition, according to the Rome III criteria, the defecation pattern is normal in patients with FAP, while altered bowel movements and/or relief of pain after defecation are typically seen in IBS.1 These functional gastrointestinal disorders are among the most common complaints in paediatric patients, affecting approximately 20% of all children.2 The pathophysiological mechanisms underlying functional gastrointestinal disorders are not completely understood.3 Functioning of the gastrointestinal tract can become disrupted, for instance through dietary influences, lifestyle changes, psychological factors or after bacterial or viral gastroenteritis.4 Studies using functional brain imaging techniques suggest that alterations in the brain–gut axis in response to visceral stimuli may result in visceral hypersensitivity and an abnormal pattern of motility in the gastrointestinal tract. Interpretation of psychosocial factors can influence the brain–gut axis, thereby affecting symptom experience.4 ,5
Treatment of both conditions is often symptomatic, with standard medical care consisting of dietary advice, education and medication such as pain medication, laxatives, antidiarrhoeal or antispasmodic agents.6 ,7 Furthermore, evidence exists that cognitive behavioural therapy can improve pain and disability.6 ,8 Despite all available interventions, treatment is not effective in up to 50% of patients, and symptoms persist into adulthood.9 Gut-directed hypnotherapy has been demonstrated to be effective in adult IBS patients who failed standard medical care, and the beneficial effects appeared to be long lasting.10–17 In 2007, a Cochrane Review by Webb et al15 concluded that data on the efficacy of gut-directed hypnotherapy in children and adolescents with IBS or FAP were lacking. Since then several studies in children and adolescents have been published and, therefore, our aim is to review the efficacy of gut-directed hypnotherapy systematically in these studies.
Methods
Search strategy
An electronic literature search of Medline, Embase, PsychINFO, Cumulative Index to Nursing and Allied Health Literature databases and the Cochrane Central Register of Controlled Trials was conducted. Our search strategy was based on the strategy used by Webb et al15 in their Cochrane Review. Search terms used combined items related to FAP and IBS in children and to hypnotherapy. To identify additional studies, reference lists of relevant studies identified in the literature search were searched by hand. This review covers literature on this subject published to February 2012. No language restriction was applied. The full search strategy and keywords are available from the authors.
Study inclusion
Two authors independently assessed titles and abstracts of all potentially relevant studies identified in the literature search. In the case of disagreement between authors about the inclusion of a study, consensus was reached by discussion. Only studies in children and adolescents were included.
In hypnotherapy, a patient is induced into a hypnotic state and guided by a therapist to respond to suggestions for changes in subjective experience, alterations in perception, emotion, thought or behaviour.18 This hypnotic state has several elements such as a feeling of ease or relaxation, an absence of judging and an absorbed attention on imageries. Guided imagery (GI) is a form of relaxed and focused concentration, in which children are encouraged by a therapist to imagine being in their favourite place or doing their favourite activity and image the sights, sounds and smell of that place/activity.19 Although the hypnotic state is officially not induced during GI, the absorption in imageries often results in a hypnotic trance. GI, therefore, is a technique that is highly comparable to hypnotherapy, because both are using relaxation and imageries and both aim to change mental and physical experiences with the use of suggestions.18 ,19 Because of these similarities, we included studies using either hypnotherapy or GI.
Hypnotherapy/GI could be performed by a qualified hypnotherapist or through self-exercises recorded on audio CD. Control treatment could include any standardised form of care such as medical care based on symptomatic treatment, psychological therapy, waiting list controls or no treatment. We only included studies in which diagnostic criteria of FAP or IBS were explicitly defined. Only randomised controlled trials (RCT) were included. Case reports, comments and letters were not included in this review.
Data collection and analysis
The methodological quality of the included RCT was assessed using the Delphi list (table 1).20
The Delphi list
Data on the following type of outcomes were extracted: (1) abdominal pain; (2) overall bowel symptom score; (3) general wellbeing or quality of life; (4) costs; (5) sick leave from school. We also extracted key characteristics of study populations, interventions, design and conduct of each included study. This information was used to assess the risk of bias of each study and to understand variability in results between included studies. If present, results on each type of outcome, including details on the measurements itself, were recorded.
Random effects models were used to meta-analyse and calculate summary estimated with corresponding 95% CI. Pooling was performed if there were at least four studies reporting on the same outcome and if those studies are comparable in design and conduct.
Results
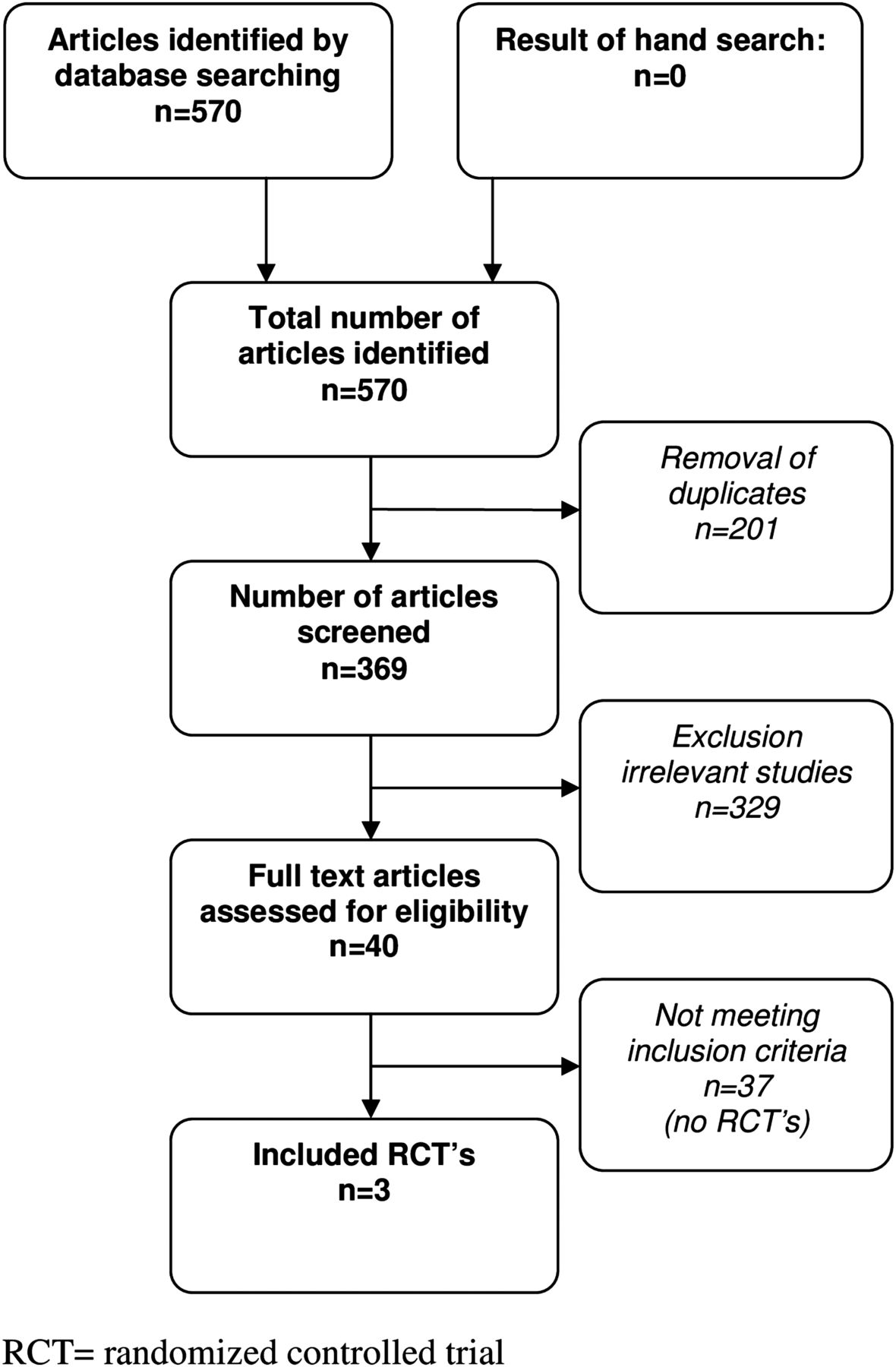
A total of 570 potentially relevant studies was identified in our electronic literature searches. Cross-referencing did not identify any additional studies. After the exclusion of duplicates (n=201), irrelevant studies (N=329) and studies not meeting the inclusion criteria (N=40), three RCT remained.21–23 No RCT were excluded after full text evaluation. A flowchart of the retrieval and inclusion process is shown in figure 1.
{kind=link}
Flowchart showing results of literature search and study inclusion. RCT, randomised controlled trial.
Sample sizes in the three included trials were 22, 34 and 52 patients, respectively, for a total of 108 patients.21–23 A range of different outcomes was reported. When a similar outcome was reported, for example, abdominal pain, different instruments and measurement protocols were applied. One study reported long-term outcomes, with a follow-up period of at least 1 year, to assess whether the effects of hypnotherapy were sustained over time.23 One study assessed general health-related quality of life.22 Costs were not reported in any of the trials. School absenteeism was reported in two studies.21 ,22 One study reported on school absenteeism at baseline, but did not report on these results after therapy.23
Risk of bias
All included studies were randomised, but details on concealment of allocation were not reported in one trial.22 In all studies the groups compared were similar at baseline with respect to the most relevant prognostic factors.
Because of the impossibility of blinding the intervention to patients and treating physicians results could be influenced by other factors besides the intervention. However, in the trial by Weydert et al21 the research associate assessing the outcomes was blinded and in the trial by Vlieger et al23 pain diaries were extracted by a blinded research associate.21 ,23 Because symptoms were recorded by patients and/or parents in all trials, outcome measurements were not influenced by the judgement of an investigator.
Completeness of follow-up was adequate in all trials, so the risk of attrition bias was low. Table 2 shows scores on methodological quality. Two of the included trials examined hypnotherapy performed by a therapist,21 ,23 while one trial examined hypnotherapy through self-exercises on audio CD.22 The characteristics and results of these studies are shown in table 2 and below.
Study characteristics and results from included trials
Individual hypnotherapy by a therapist
The two trials examining hypnotherapy performed by a therapist included a total of 74 children aged 5–18 years.21 ,23 In one study hypnotherapy was given by a single experienced and qualified hypnotherapist.23 In the other study the number of experienced and qualified hypnotherapists participating in the treatment was not specified.21 In both trials the hypnotherapy protocol used consisted of techniques that emphasise control of abdominal symptoms together with general relaxation, ego-strengthening and changing of cognitive perspective and coping skills.24 The period of treatment was 1 month21 and 3 months.23 Patients in both studies had long-lasting symptoms, but different diagnostic criteria were used. Weydert et al21 used Apley's criteria for recurrent abdominal pain, in which no differentiation is applied between FAP and IBS. Children with a history of at least three episodes of abdominal pain severe enough to affect normal activities, during the previous 3 months, were included. Participants were required to be stable on the current medication they were taking and were instructed not to add, delete, or change the dosing of medication. Patients in the control group received sessions of supportive therapy in which they received breathing exercises.
In the trial by Vlieger et al,23 Rome II criteria for FAP and IBS were used to include children. Controls received standard medical care consisting of education, dietary advice, extra fibre and medication if necessary. They also received six sessions of supportive therapy with their paediatrician or paediatric gastroenterologist.
Efficacy of hypnotherapy by a therapist
Both trials reported statistically significant lower levels of abdominal pain and symptom scores in patients receiving hypnotherapy at the end of therapy compared to controls (table 2). Due to difference in the outcome measures used, we refrained from pooling them.
Long-term results were only reported by Vlieger et al,23 showing a significant effect in favour of hypnotherapy. After 1 year of follow up, 85% of children in the hypnotherapy group were in clinical remission compared to 25% of controls. A long-term follow-up study in the same group was recently published. Five years after treatment significantly more children who received hypnotherapy were still in remission compared to children receiving standard care plus supportive therapy: 68% vs 20%, p=0.005.25 Results on quality of life and costs were not reported in either trial. Weydert et al21 reported a significant decrease in the number of days on which children missed activities, such as school, sports and social activities, in favour of hypnotherapy. Vlieger et al23 only reported school absenteeism at baseline. No harmful side effects were reported in either trial.
Hypnotherapy through self-exercises on audio CD
A single randomised trial was included, which examined the efficacy of hypnotherapy induced by self-exercises on audio CD.22 Van Tilburg et al22 included 34 children aged 6–15 years, with a physician diagnosis of FAP, who had abdominal pain severe enough to disrupt activities at least once per week in the past 3 months. Patients were treated with standard medical care with or without home-based, GI. GI treatment was based on a protocol for developed by Palsson et al26 and contained the same elements used in individual hypnotherapy given by a therapist.19 Children were instructed to listen to the audio CD at least 5 days per week for 2 months.
Efficacy of hypnotherapy through self-exercises on audio CD
At the end of treatment, levels of abdominal pain and symptom scores were significantly lower in patients undergoing hypnotherapy through self-exercises on audio CD compared to controls receiving only standard care. Treatment response was defined as a 50% or greater reduction in abdominal pain score. After treatment there were significantly more treatment responders in the group receiving hypnotherapy (63%) than in the group receiving standard care only (27%). After 6 months of follow-up, consolidation of this treatment effect was demonstrated, with 62.5% of treatment responders in the hypnotherapy group. The trial showed significantly improved quality of life scores in the hypnotherapy group. Results on costs were not reported. No difference in school absenteeism was demonstrated between both groups after treatment. The trial also did not report any harmful side effects.
Discussion
Our systematic review identified three RCT with a limited number of paediatric patients. All three trials indicated that both hypnotherapy given by a qualified therapist and hypnotherapy through self-exercises on audio CD are effective treatments in paediatric patients with FAP or IBS. Pain levels after treatment were significantly more reduced in patients receiving hypnotherapy compared to patients receiving various control treatments. Vlieger and colleagues23 ,25 reported long-term treatment outcomes indicating that beneficial effects are long lasting, up to approximately 5 years after treatment.21 ,22 Quality of life was only reported in one trial and showed a significant improvement in patients receiving GI.22 Costs were not reported in the included trials.
Drawing firm conclusions on the results of those trials is difficult. Foremost, the body of evidence is still limited given that only three trials have been performed, all having very small sample sizes. The methodological quality of the studies was adequate, taking into account that blinding of patients and care providers was not possible.
The interpretation of results was also hampered by different types of control treatments and outcomes that were selected in the trials. We decided to refrain from statistical pooling because of the low number of studies and many differences in design and reported outcomes.
The positive effects of hypnotherapy in children with FAP and IBS found in the three trials are in accordance with reports in adults. Since 1984, seven RCT on the efficacy of gut-directed hypnotherapy including a total of 337 adult IBS patients have been performed.10 ,11 ,13 ,14 ,16 ,17 In six RCT hypnotherapy was given by a qualified therapist,10 ,11 ,13 ,16 ,17 in one study hypnotherapy consisted of self-exercises on audio CD.14 All trials reported significantly lower pain levels and symptom scores in patients receiving hypnotherapy compared to various control treatments. Although sample sizes were relatively small (range 6–90 patients) and some methodological limitations were present, hypnotherapy can be considered a valuable therapeutic intervention for adult IBS patients.15 Adult studies on long-term follow-up ranging from 1 to 7 years after treatment, show persisting effects of gut-directed hypnotherapy.12 ,27 One trial in adult IBS patients suggested that the effectiveness of hypnotherapy is influenced by the setting in which it is given, with hypnotherapy given outside a highly specialised centre being less effective.16 Future research has to show whether this may also be the case in children.
Working mechanism of hypnotherapy
The mechanism by which hypnotherapy/GI acts in improving abdominal symptoms in FAP and IBS is still not well understood. It is hypothesised to have effects on both physiological and psychological processes.11 Hypnosis has been demonstrated to lead to a change in colonic motility, but whether this effect persists when a patient is no longer in a hypnotic state is unknown.28 The effect of hypnotherapy on visceral hypersensitivity is not well defined. Two studies in adult IBS patients identified a reduction in visceral sensitivity after hypnotherapy,29 ,30 but one trial in children failed to find this effect.31
Hypnotherapy significantly reduces psychological factors such as somatisation and psychological stress, and this effect seems to persist over time.11 Hypnotherapy may exert these effects by modulating the abnormal hypothalamo–pituitary–adrenal axis response to stress seen in IBS patients.32 ,33 It is also known that many IBS patients have dysfunctional cognitions, and it has been demonstrated that symptom improvement in adult IBS patients receiving hypnotherapy is associated with a change in these negative cognitions.34 The improvement in IBS symptoms is also associated with an improvement in general quality of life and reduction of psychopathology, such as depression and anxiety. It does, however, remain unclear whether an improvement in psychological factors causes the positive effects of hypnotherapy or is a consequence of it.35 Hypnotherapy may also act on central nervous system processes, because FAP and IBS may be caused by altered central modulation of visceral stimuli. Pain processing regions in the brain, such as the anterior cingulated cortex and amygdala, appear to react more extensively in adult IBS patients,36 and hypnotherapy seems to reduce this activity in these brain regions.37 ,38 To date, no trials evaluating these brain regions in paediatric IBS patients after hypnotherapy are available.
Conclusion
It remains difficult to quantify the exact benefits of hypnotherapy, because of the limited number of RCT on this subject, small sample sizes of the included studies, differences in control treatments used and inconsistency in reported outcome measurements. However, all three available randomised trials do provide an indication that hypnotherapy performed by a qualified therapist or through self-exercises on audio CD is more effective than standard medical treatment in reducing symptoms in children with FAP or IBS.
The need for more high quality RCT in this paediatric population is, however, evident. Future research must take into account the following factors: (1) sufficient samples sizes; (2) follow-up period of at least 1 year to determine whether treatment effects sustain; (3) using strict criteria for diagnosing FAP and IBS; (4) evaluation of both newly diagnosed and treatment-resistant FAP and IBS patients; (5) quality of life; (6) costs; and (7) to assess whether the efficacy of hypnotherapy in children is influenced by the setting in which it is given and the level of experience of the hypnotherapist.
Acknowledgments
The authors thank Arnold G E Leenders for his assistance with the electronic literature search.
References
Footnotes
-
Contributors All authors participated in the design of the study. JMTMR: collected data, performed data analysis, drafted the initial manuscript, approved the final manuscript as submitted and was responsible for overall content as guarantor. JBR: critically reviewed methods and the manuscript and approved the final manuscript as submitted. AMV: collected data, performed data analysis, critically reviewed the manuscript and approved the final manuscript as submitted. MAB: collected data, performed data analysis, supervised drafting of the manuscript and approved the final manuscript as submitted.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.