Article Text

Abstract
Introduction Renal cancers constitute about 6%–7% of all childhood tumours. Wilms’ tumour is the most common renal tumour in childhood. Clear cell sarcoma, malignant rhabdoid tumour, congenital mesoblastic nephroma, renal cell carcinoma can also found infrequently. Clinically, they are indistinguishable from Wilms’ tumour. They are usually diagnosed by tissue biopsy in the form of histopathological examination and immunohistochemistry. Early stage Wilms’ tumour and mesoblastic nephroma have favourable prognosis; but others are rapidly progressing and have a poor outcome with high risk of metastasis and relapse. Hence, these tumours should be kept in mind in differential diagnosis. In this article, we present two cases of clear cell sarcoma and rabboid tumour, which are rare renal tumours in childhood.
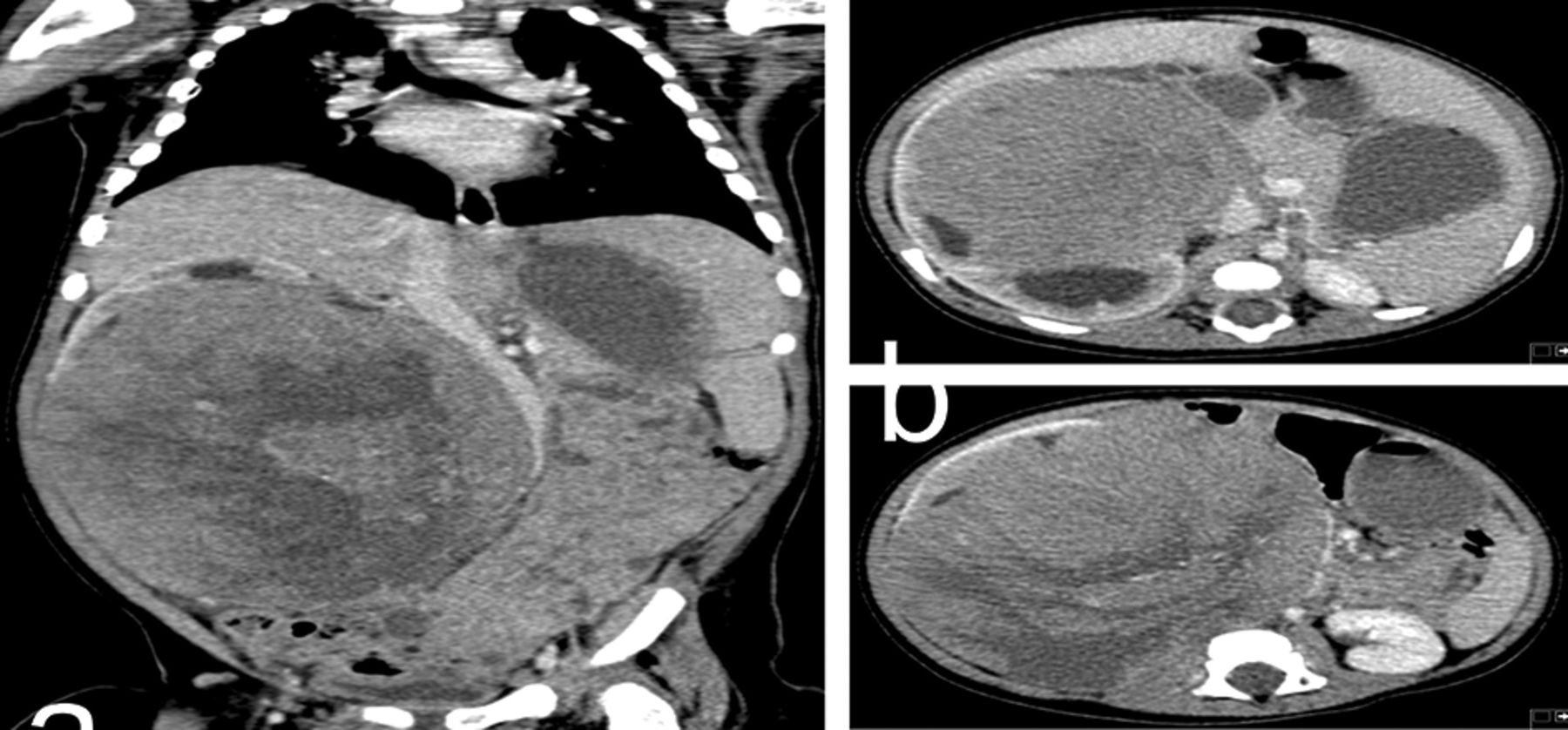
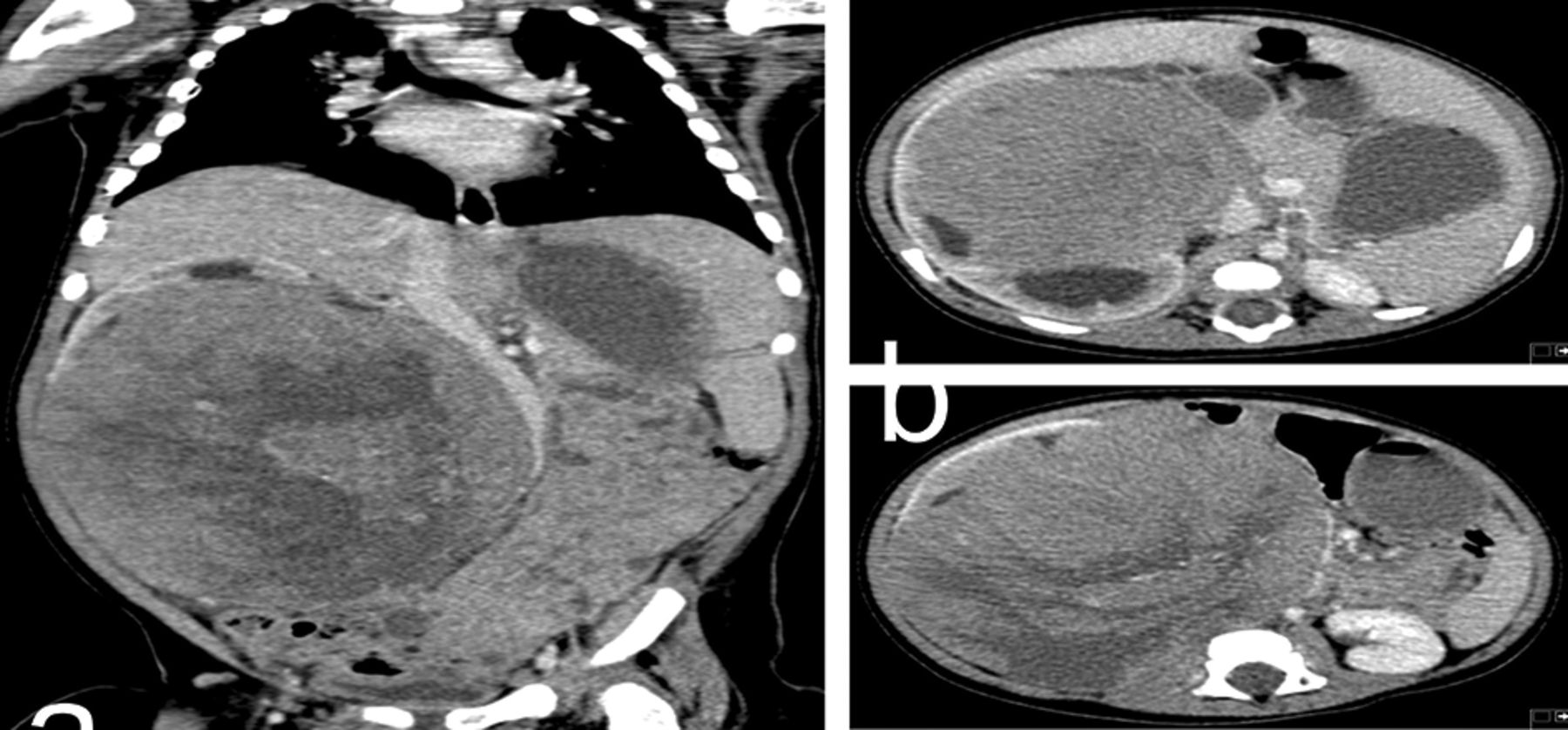
Case report 1 A 6-month-old male child presented with a palpable abdominal mass recognised by his mother. He was asymptomatic except for a palpable solid mass extending from the right flank. Blood tests were unremarkable. Ultrasonography and computed tomography (CT) scan of the abdomen revealed a large heterogeneous, hypoechoic solid mass arising from the right kidney measuring 17.5 × 13 × 15 cm and the mass crossed the midline (Figure 1). No metastasis was detected in the lungs, liver, or bone by analysis of CT, magnetic resonance imaging and 99mTc scintigraphy. The patient underwent right radical nephroureterectomy with lymph node dissection.Pathological analysis resulted as ‘clear cell sarcoma of the kidney’ (Figure 2).Chemotherapy and radiotherapy were administered according to the ‘National Wilms Tumour Study Group (NWTS)−5. The patient has remained in complete remission for 2 years.

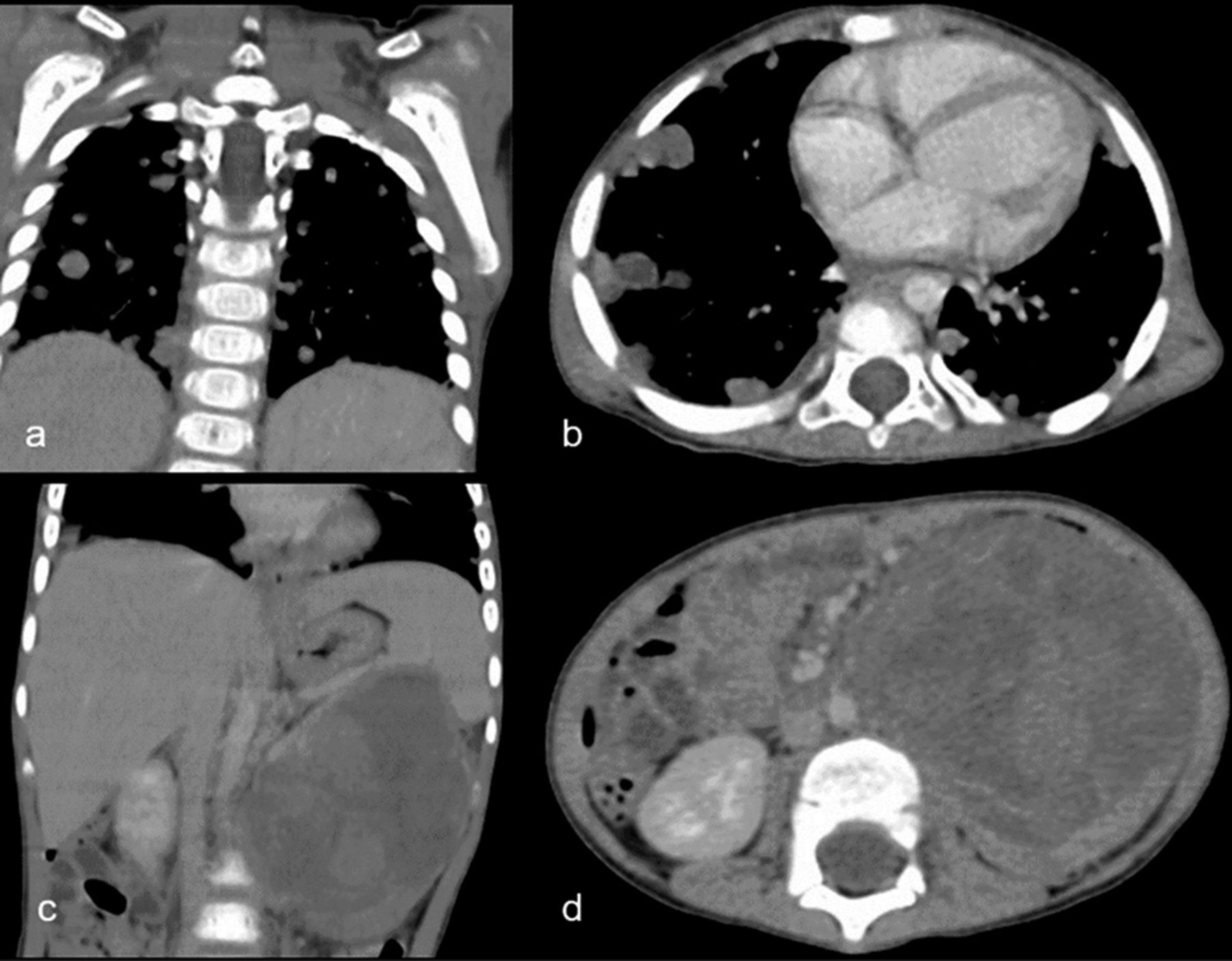
Case report 2 A 2-year-old boy was brought to the emergency department with a history of hematuria, fatigue, abdominal pain and weight loss. Physical examination revealed a palpable abdominal mass extending from the left flank. The abdominal USG and CT revealed a 98 × 73 mm lobulated solid mass in the upper pole of left kidney, as well as enlarged perirenal lymph nodes and multiple metastatic nodules in liver. Thorax CT showed multiple metastases in both lungs. No metastasis was detected in brain (Figure 3). These CT findings were highly suggestive of a malignant renal tumour with lymph nodes lung and liver metastases. The patient underwent left radical nephroureterectomy with lymph node dissection, histopathological examination was reported as ‘Malignant Rhaboid tumour of kidney’ (Figure 4). Despite treatment, he developed multiple metastases 2 months after initial presentation and died soon after.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Discussion A paediatric renal tumour is much more commonly to be a Wilms’ tumour. Clear cell sarcoma and malignant rhabdoid tumours of kidney are frequently confused with Wilms’ tumour though such tumours are very rare in children. Clear cell sarcoma comprises of 3% of all childhood renal tumour and also known as ‘bone metastasing tumour’. Rhabdoid tumour of kidney accounts for 2% of all renal tumours and it is the most aggressive renal tumour in paediatric age group. Both of these tumours present in advanced stage and resistant to chemotherapy. Aggressive surgical approach followed by chemotherapy and radiotherapy is necessary. Relapses are common.The prognosis for children remains poor, depending on the stage of the tumour at presentation.