Article Text

Statistics from Altmetric.com
Russia is the largest country in the world, with an area spanning more than 17 million km2. Her population, according to the official statistics (as of 1 January 2014), is 143 666 931 people (which is the ninth place in the world). Children under the age of 18 make for approximately 19.1% of Russia’s population (27 374 352). This population is spread extremely unevenly over her huge territory: 72.2% of Russians live in the European part of the country, which comprises only 25% of the whole territory.1 The Moscow region has the highest population density among all other regions, with more than 4626 persons/km2. The least density belongs to the Chukotka Autonomous Region, with less than 0.07 persons/km2.
Evolution of the Russian child care system: from the Russian Empire to modern days
The Russian child care system has been supported by state and private contributions since the times of monarchy. The state’s first steps towards building a childhood and motherhood protection system date back to the 18th century when the first orphanages appeared by the orders of Empress Catherine II (1763 in Moscow and 1770 in St Petersburg). These orphanages had their own hospitals where the children received medical treatment.2 3
The drive behind the formation of the system of mothers and children care was the struggle for reducing child mortality rates, which was named as one of the most important Russian social issues in the late 19th century and in the beginning of the 20th century.4 High mortality rates were largely due to poor social, cultural and economic conditions.
Russian paediatrics has always been an integral part of world science and practice. For example, Karl Martens was the first chief doctor of the Moscow foundling hospital, and saved the wards from the plague epidemic of 1771–1773. His treatise on this subject (published in Paris in 1784) had a big impact on the medical science of the day, and was republished 35 times in Europe and America in five languages. Another German doctor, Johann Heinrich Jänish, was the first doctor to vaccinate against smallpox at the same hospital in 1773–1780.
The healthcare model as formulated after the 1917 coup (the Soviet healthcare system) was based on the six following principles5 6:
the state’s responsibility for healthcare
free healthcare for everyone
special attention to maternity and childhood
promotion of a healthy lifestyle, prevention and prophylaxis
preventive treatment of socially significant diseases
involving society into healthcare activities.
The issues of maternal and child health have received special attention in the Soviet healthcare system from its very beginning, adult and child healthcare were separated, and special highly qualified child doctors (paediatricians) were being trained. For the first time in the world, medical faculties of universities began the training of child doctors in 1930 in the USSR. Paediatric education included special hours for teaching all medical subjects (anatomy, physiology, biochemistry, etc) as applied specifically to children.
The outpatient polyclinic was (and still is) the main place for the protection of children’s health (the central figure is the district paediatrician). Child polyclinics deliver all preventive and therapeutic activities (including vaccination and health monitoring), and if necessary the child can be directed for inpatient treatment to child hospitals, then depending on the situation, he or she either returns back to be observed by the local paediatrician or is sent to the next stage—sanatorium/resort rehabilitation.
During the first years of the Soviet power, there was much bidirectional academic exchange that continued after the end of the Stalin era. For the majority of doctors, however, participation in international conferences and congresses was impossible (due to the ‘iron curtain’), but leading scientists and clinicians preserved the connection to the world paediatric community.
We should note that the Soviet healthcare model for children had obvious advantages, including the following:
high accessibility of primary and specialised medical help
state-guaranteed free medical help
maternity and childhood protection priority
preventive orientation
step-by-step medical treatment.
At the same time, the Soviet model had some clear problems:
lack of funding
problems with supplying enough modern medicines, high tech medical equipment and expendables.
At the end of the 1980s there was some reorganisation of the child healthcare system that focused primarily on the neonatal and perinatal services after one of the authors of this article (AAB) became head of the child and maternity protection service of the USSR Health Ministry.
Post-Soviet child healthcare development: main state and social initiatives
The Russian healthcare system, although retaining a lot of key Soviet principles, has been greatly altered in terms of funding and management since 1991. The state healthcare has been divided into federal and regional systems. The funding became mixed—state-based and insurance-based.
Legislative initiatives. During this period of time, Russia has ratified basic international child healthcare documents, such as the United Nations Convention on the Rights of the Child (1993) and the United Nations Convention on the Rights of Persons with Disabilities (2008).
The Ministry of Health order ‘On the transfer to WHO live and still birth criteria’ was signed in 1992, with a subsequent programme being developed for reaching these criteria (criteria came into effect in 2012).
From 1999, adolescents under the age of 18 were added to the paediatric service area of responsibility. Before this paediatricians dealt only with children up to 15 years old.
Modernisation of child healthcare facilities. The number of child wards is being reasonably decreased, while their specialisation is greatly improved. At the same time the government is broadening the network of outpatient and polyclinic facilities, as well as day hospitals. The third part of medical treatment (sanatorium and resort facilities), which was lost during the 1990s (they stayed out of Russia—in Baltic and Central Asian countries, in Ukraine, etc), is now being restored through creating rehab centres all over the country for children to restore their health.
In order to reduce the infant mortality rate further, more than 100 modern perinatal centres were created and new ones are being built all the time. This allowed achieving a reduction in perinatal and obstetric pathology through rationally applying modern expensive neonatal and obstetric technologies.
Vaccination. The programme is in line with WHO recommendations, although it does not currently include rotavirus and papillomavirus immunisation and is totally funded by the federal budget. Some regions of Federation have adopted a broader local calendar of preventive vaccines, including 17 diseases (at the expenses of regional budgets).
Neonatal screening. In accordance with international recommendations, Russia conducted neonatal screening on phenylketonuria and congenital hypothyroidism. Since 2006 adrenogenital syndrome, galactosaemia and cystic fibrosis have been included in screening. Audiological screening of first-year children, which helps to diagnose hearing infringements in children at an early stage and thus make a rehabilitation possible, was started in 2007.
Professional societies. Over the years following the collapse of the Soviet Union, the paediatric community (one of the biggest medical communities), being united into the Union of Pediatricians of Russia, has developed an active social position. For example, in 2005 the community managed to save the unique structure of primary paediatric aid with the local paediatrician being the key figure, instead of the Western model with the general practitioner, which doesn’t take into account the special features of the Russian child healthcare system.
International collaboration After 1991 the international cooperation has greatly increased in terms of child healthcare. The two main trends of international cooperation in this area are political and professional.
These include the direct participation of Government and Health Ministry leaders as part of defining the global strategy, and the Russian healthcare’s role in the global and regional processes such as forming the position towards the plans and programmes of international organisations, international treaties and priority areas of international cooperation.
Further work is being undertaken as part of professional international community interchange. The Russian paediatric society actively communicates with international professional organisations, and in 2009 the IV EUROPAEDIATRICS was held for the first time in history in Moscow. In 2013 a Russian paediatrician (L Namazova-Baranova) was elected as President of the European Paediatric Association and Union of National European Pediatric Societies and Associations (UNEPSA) (which was created in 1976 to unite paediatricians from both parts of Europe through the ‘iron curtain’).
The Scientific Centre of Children’s Health is the leading paediatric facility that coordinates the scientific and research activities concerning the protection of child health in Russia. It is notable that over the centuries, child health protection is still being secured by the successor of the first Moscow hospital (now called the Scientific Centre of Children’s Health), which celebrated its 250th birthday in 2013.7
The present day
Today there is a united healthcare system in Russia that consists of subsystems ordered hierarchically. The Ministry of Health exercises the coordinating functions.
The child healthcare system is composed of a network of outpatient and inpatient facilities and health resorts, which provide all types of preventive, diagnostic, medical, rehabilitative and palliative treatment, and a network of paediatric institutions such as orphanages and palliative facilities.
Inpatient facilities include multiprofile child hospitals, infectious child hospitals, maternity hospitals, perinatal centres and child departments of special hospitals (psychiatric, narcological).
Historically the mental health services (psychoneurological dispensaries) for children and teenagers were separated from paediatric services. Recently the situation has started changing: in some regions the psychiatrist is being included into the child polyclinic’s multidisciplinary team.
Sanatorium resort care is provided at paediatric sanatoriums/resorts. Palliative care for children is provided at home, as outpatients (offices of palliative care), in hospitals (palliative wards in paediatric hospitals) and at paediatric hospices.
Primary health for children is provided on a territorial basis (to maximise its proximity to the place of residence of a child) and based on a free choice of doctor.
The basic structural unit of primary health care (PHC) is the outpatient and polyclinic institutions (paediatric polyclinics) providing continuity, and based on the neighbourhood principle the provision of free medical care for children aged 0–18. District paediatricians, paediatric medical specialists, auxiliary medical personnel, necessary diagnostic, therapeutic and rehabilitation equipment for outpatient care, and provision of hospital-replacing technologies are located at the abovementioned paediatric polyclinics. The structure of paediatric polyclinics is determined in accordance with the assigned tasks (figure 1).
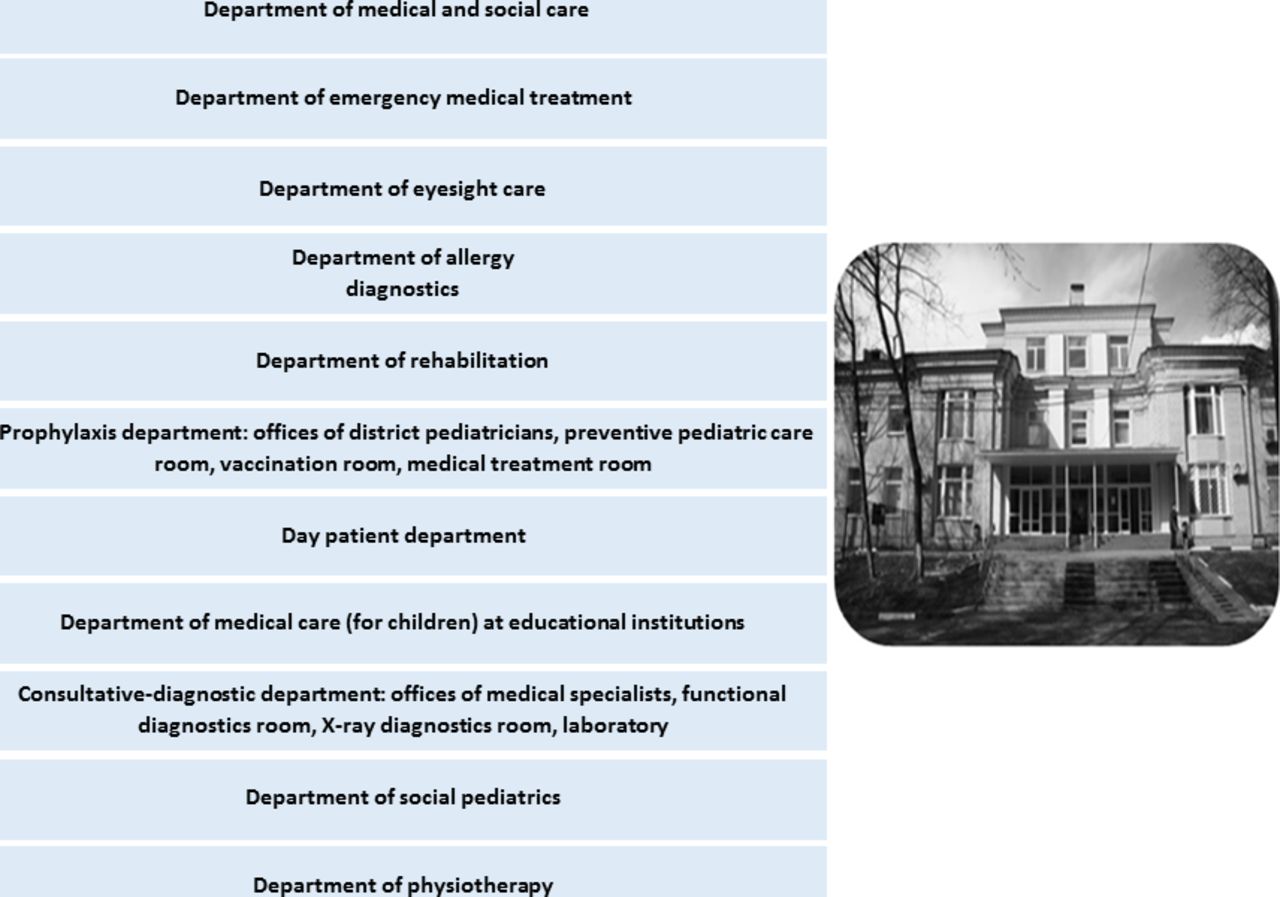
Structure of a paediatric polyclinic in Russia.
Responsibilities of polyclinics are presented in figure 2.

Responsibilities of paediatric polyclinics in Russia.
Continuity and interdepartmental cooperation with educational institutions (preschool and school) is provided by the department of medical care to children at educational institutions. Medical examinations of children are carried out directly at schools and kindergartens.
Evident preventative orientation of paediatric healthcare is reflected in the organisation of regular preventive examinations of healthy children in the decreed time. A paediatrician and medical specialists up to 26 times during first year of life conduct preventive examinations of infants. Subsequently, children are assessed annually by a paediatrician until the age of 18 years. Preventive examinations in the aforementioned periods encompass from 90% to 92% of children aged 0–18 (according to the data of the Ministry of Health). Vaccination covers up to 95%–97% of children, one of the highest in the world.
Support for vulnerable and maltreated children is an important activity of paediatric polyclinics. Departments of health and psychosocial care of paediatric polyclinics provide professionals such as paediatrician, psychologists, social workers and lawyers. Special attention is given to the early detection of psychosocial risk factors and interdisciplinary care for children at social risk.8
When hospital treatment or high tech medical care is required, a child is transferred to other levels of the system: to the nearby paediatric hospital, or in severe cases to republican or federal specialised centres.
Paediatricians are still trained at paediatric faculties of universities. The unique potentialities of the newly constructed, highly specialised simulating training centre on the basis of medical schools are used widely.
Insufficient funding remains a serious problem today: the government health spendings are still below 6%—the WHO recommended minimum—and are still around 4% gross domestic product.
Dynamics of the main indicators of children’s health in Russia
Infant mortality
During the post-Soviet period, there was a significant decrease in the infant mortality rate—from 17.4 per 1000 live births in 1990 to 6.5 per 1000 live births in 2015 (figure 3). The maximum rate of decline of infant mortality has been observed within the past decade and showed the effect of improvement of living standards on infant mortality.9 10

Infant mortality in Russia (per 1000 live births).
The last increase in infant mortality in 2012 (8.6 per 1000 live births) was associated with the transition to the new criteria of live birth registration. The 24.7% difference between rural and urban infant mortality still needs to be addressed, and there remain wide provincial differences: 4.1 per 1000 live births in the Tambov region to 21.2 in the Chukotka Autonomous Region (2012).
The mortality of children under 5 has decreased twice within the past decade (from 21.3 in 1990 to 9.6 in 2014 per 1000 children of the relevant year of birth) (figure 4).

Mortality under 5 in Russia (per 1000 live birth).
In terms of death of children under 5, the leading positions are occupied by certain conditions originating from the perinatal period (46.4% in 2012) and congenital anomalies (20%). It is noted that the third place is occupied by external causes of death (10.6%)—injuries, poisoning and accidents. A significant proportion in this age group is occupied by such controlled factors as respiratory diseases (5.4%) and infectious diseases (4.3%). The proportion of deaths of cancer is up to 2%.
Adolescent mortality has fallen (figure 5), although it continues to remain the highest among economically developed countries and many (70%) are from preventable causes such as injuries and poisoning.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Adolescent mortality in Russia (per 100 000 of corresponding age).
The main external causes of adolescent deaths are suicides, which amount to about one-quarter (24.3%) of all traumatic deaths in this age group; other causes are traffic accidents (23.9%) and accidental poisoning (9.4%). The suicide rate among Russian adolescents is the highest in Europe. The increase in this rate is of particular concern. Thus, whereas in 2009, 260 suicidal deaths were registered, in 2012 the rate amounted to 487 deaths as a result of deliberate self-inflicted injury.
The rate of mortality of injuries inflicted with uncertain intentions or injuries (not specified) remains extremely high in Russia.10 A significant part of mortality caused by such socially driven and socially important causes as murder and drug poisoning can be disguised in the aforementioned causes.
The reduction of mortality caused by infectious diseases (50%), injury and poisoning (37.4%), and cancer (27.3%) has been considered to be the most significant over the past 10 years.
Reducing child mortality
The Russian experience of universal paediatric care coverage for child population as an instrument for achieving Millennium Development Goals.
The Russian Federation is a country with the most child-oriented and even child rights-oriented systems of paediatric healthcare, and has achieved considerable success in reducing infant, child and maternal mortality, as well as in the prevention, diagnosis and treatment of infectious and non-infectious diseases in children, and continues its consistent steps to other states on achievement of the Millennium Development Goals.
Altruism
Since 2010, as part of the implementation of the Muskoka Initiative on maternal, newborn and children under 5 health, Russia has assisted with the transfer of health service experience to countries with developing economies. For this purpose during the last 5 years, the Government of the Russian Federation has funded a number of projects on supplementary training for paediatricians, neonatologists, anaesthetists and other paediatric specialists from Asia, Africa and Latin America. The Russian Federation also provided a 3-year (2012–2014) project funding to be administered by the WHO to support improvement in the paediatric quality of care at first-level hospitals in Africa and Central Asia.11
The main objectives of the project were to (1) improve the quality of paediatric care in at least 80 selected first-level referral hospitals in the four countries; (2) provide support to expand the experience nationally; (3) introduce the concept of paediatric care standards in the national education and training of health professional to sustain the project's results; and (4) update and develop relevant international guidelines and tools on the basis of experience gained through the project implementation.
Over the past 3 years, the Scientific Centre of Children’s Health has worked closely with the WHO to decrease child mortality in low/middle-income countries of Asia and Africa (Angola, Ethiopia, Kyrgyzstan and Tajikistan).12 A modern simulative training centre for paediatricians of different specialisations was opened in the Scientific Center of Children's Health (SCCH) as part of this project.
This project has provided a very excellent model of collaboration with the Russian institutions. The capacity of the National Scientific Centre of Child Health has been very instrumental in participating and supporting various activities that have so far been implemented.
In accordance with the Prime Minister’s Decree,11 nine medical educational seminars were conducted in 2014–2015. These were attended by 270 paediatricians from 10 countries (Angola, Armenia, Botswana, Kirgizstan, Moldova, Mongolia, Nicaragua, Tajikistan, Uzbekistan and Vietnam). The course was devoted to treating emergency acute states in children. The programme of each seminar was planned for 72 hours, including lections (24 hours) and practical skills training (48 hours).
Conclusion
From the very first days of the formation, Russian paediatrics has always been an integral part of the world’s science and practice. At the same time, Russia has a healthcare system that possesses its own distinctive features, many of which were inherited from the Soviet model.
Footnotes
Contributors Conception or design of the work: A
B, LN-B, VA, NU.
Data collection: VA, NU, RT.
Data analysis and interpretation: AB, LN-B, VU, NU, RT.
Drafting the article: LN-B, VA, NU.
Critical revision of the article: AB, LN-B, VA, NU, RT, OK.
Final approval of the version to be published: AB, LN-B, VA, NU, RT, OK.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.
Correction notice This paper has been amended since it was published Online First. Owing to a scripting error, some of the publisher names in the references were replaced with 'BMJ Publishing Group'. This only affected the full text version, not the PDF. We have since corrected these errors and the correct publishers have been inserted into the references.