Article Text

Statistics from Altmetric.com
The development of a United Nations sponsored Millennium Development Goal (MDG) relating to childhood survival contributed significantly to reducing mortality among children under 5 years old in many countries in the first years of the twenty-first century.1 The development of an independent authoritative mechanism, the Countdown to 2015 Collaboration contributed significantly to global progress towards the goals.
While childhood mortality in the UK has also decreased over the past 40 years, the UK's child mortality trends and excess deaths figures compare unfavourably with many European countries.1 ,2 It is increasingly clear that the UK could do better in ensuring the best possible conditions for children to survive and thrive. Several recent publications have highlighted the extent of the problem, and stimulated responses from government and non-governmental sectors.3–7 We propose now that an independent cross-sector mechanism be set up to agree targets for reduction of UK excess child and adolescent mortality, identify gaps in knowledge, monitor progress in reaching goals and make recommendations that contribute towards improving UK child survival.
In this paper, we first review the UK's performance on child and adolescent mortality compared with other wealthy countries in order to establish a baseline for future monitoring. We examine why the UK has higher child and adolescent mortality compared with some other European countries, by describing main causes and social determinants of death. Finally we explore what can be done to reduce mortality, and make recommendations to improve UK child and adolescent survival.
Trends in UK and European child mortality
We used data from the Organisation for Economic Cooperation and Development (OECD) for infant mortality8 and the WHO World Mortality Database for 1–19-year-olds9 to calculate centiles of child and adolescent mortality for a group of comparable wealthy countries identified as appropriate comparators for UK mortality.1 ,10 These countries are the 15 member states of the European Union in 2004 (excluding the UK) together with Australia, Norway and Canada, referred to as the EU15+. We used OECD data for infant mortality as this is available annually from routinely published data as deaths per 1000 live births of both sexes. Comparative mortality for 1–19-year-olds required calculation of mortality rates per 100 000 population from WHO raw data. For 1–19-year-olds, we calculated total annual mortality rates from 1970 to 2010 for each country for 1–4 years, 5–9 years, 10–14 years and 15–19 years. We then calculated smoothed (3-year moving averages) 10th, 25th, 50th, 75th, and 90th centiles of mortality rates for each age group 0–19 years from 1970 to 2010 for the EU15+ using Stata V.13. Centiles were calculated for both sexes together for 0–9-year-olds (due to minimal sex differences under 10 years) and separately by sex for 10–19-year-olds. The most recent OECD infant mortality data set (accessed 12 December 2014) provided data for the UK and all EU15+ countries up to 2012. In the World Mortality Database, the latest data set (deposited November 2014) only contains UK mortality up to 2010. Similarly many other EU15+ countries lack data deposited past 2010. Thus we calculated here EU15+ centiles for infants to 2012 but other age groups to 2010.
Figures 1 and 2 for 0–9 year-olds and 10–19-year-olds, respectively, show UK mortality over the past 40 years plotted against EU15+ mortality centiles for the same period. These figures show that in 1970, UK mortality was below the 25th centile in all age groups aside from infancy which was higher (50th centile), and 5–9-year-olds which was lower and fell below the 10th centile. By 2010, the UK's position had declined markedly in all age groups. UK infant mortality was above the 90th centile in 2012, and on the 75th centile for young children 1–4 years. For 5–9-year-olds and 10–19-year-old boys, UK mortality in 2010 was very close to the 50th centile. For 10–19-year-old girls, mortality in the UK was close to the 75th centile. We have previously shown that these differences are statistically significant; mortality in the UK declined significantly less than the EU15+ over the past 40 years.1


UK mortality for 10–14-year-olds and 15–19-year-olds for boys and girls plotted against age-specific and sex-specific EU15+ mortality centiles for the same period.
Age distribution and causes of death in the UK and Europe
More than 5000 children and young people between 0 years and 19 years of age died in the UK in 2012. The majority of child deaths (60%) happen before 1 year of age and the next largest proportion happen in adolescence (18%), and the causes vary substantially between age groups.11
Infants
Between 70% and 80% of infant deaths happen in the 1st month of life and nearly two-thirds of deaths are among babies who were born preterm.11 ,12 The risk of death from conditions which may be the consequences of preterm birth persists into later childhood.13 This can make it difficult to interpret comparisons in infant mortality rates, as countries vary in their thresholds for reporting infant deaths. OECD's metadata include a warning that ‘Some of the international variation in infant and neonatal mortality rates may be due to variations among countries in registering practices of premature infants. Most countries have no gestational age or weight limits for mortality registration. However, some countries specify limits based on some combination of gestational age, birth weight or survival.’8
The Euro-Peristat collaboration has documented these differences and analysed them in considerable detail in a series of reports, the most recent of which was based on data for the year 2010.12 Participants provided aggregated data for their countries, stratified by birth weight and gestational age. This allowed the group to produce data with a common cut-off threshold. This still showed considerable variation. With a common cut-off of 22 weeks of gestational age, preterm birth rates for the countries of the UK ranged from 7.0% to 7.2% compared with 5.3% to 6.4% for the Nordic countries.12
Low birthweight babies, weighing under 2500 g, account for around three quarters of neonatal deaths and two-thirds of infant deaths. The proportion of low weight births ranged from 3.4% to 9.8% of live births in 2010 in countries participating in Euro-Peristat, although the comparison of low birth weights did not use a common lower cut-off. The rates for countries of the UK ranged from 5.7% to 7.0% of live births while those for the Nordic countries ranged from 3.4% to 5.1%.12
Euro-Peristat used a cut-off of 22 weeks of gestational age for comparing infant mortality rates. On this basis, rates for the countries of the UK were not the highest in Europe, but they were still well above the rates for the Nordic countries. For neonatal mortality, rates were compared overall and using a common cut-off of 24 weeks of gestational age. Using this cut-off substantially reduced the reported rates for the countries of the UK, but made much less difference to the rates for the Nordic countries, bringing these sets of rates closer together. To enable valid comparisons in the future, therefore, it is important that international agencies adopt the approaches recommended by Euro-Peristat.12
Clinical causes of neonatal death are difficult to compare because of the differences in the ways they are classified, but in general, the excess neonatal mortality in the UK is largely attributable to perinatal causes, and the excess postneonatal mortality is also attributable to perinatal and other causes. Rates of deaths attributable to congenital anomalies and injuries are similar in the UK and the rest of the EU15+.1 After perinatal and congenital causes, the next most common causes of death in babies under 1-year-old are injuries and poisoning, and infection, each responsible for just 2% of deaths.11 Although there are many unintentional and accidental causes of injury-related deaths, and murder of children is comparatively rare, 35% of child victims of murder are under 1-year-old, and the likeliest perpetrators are the mother or father.14
Finally, stillbirths are an important factor to consider in relation to deaths in the 1st year of life. Comparisons are difficult because of the differences in the way terminations on the grounds of congenital anomaly are reported. Even so, after imposing a common cut-off of 28 weeks of gestation, Euro-Peristat found that the stillbirth rates for the countries of the UK, ranging from 3.4 to 3.8 per 1000 total births, were among the highest in Europe, while those for the Nordic countries ranged from 1.8 to 2.8 per 1000.12 Many of the risk factors for stillbirth, preterm birth, low birth weight, and infant death are shared, including social inequality and poverty.15
Childhood and adolescence
After the 1st year of life, the most common causes of death are cancer, other non-communicable diseases (NCDs) and external causes including injuries. More than half of deaths among adolescents are from external causes; the major modes are transport injuries, and intentional and non-intentional injuries including suicide and violent deaths.16 Notably, deaths from intentional injury among young people have not decreased for 30 years.13
The UK adolescent all-cause mortality rate is similar to the EU15+ 50th centile, however examining mortality by Global Burden of Disease categories reveals that NCD mortality among UK adolescents is higher, masked in the all-cause figures by the UK's relatively low injury mortality.1 NCDs caused 57% of deaths among 1–24-year-olds in 2008 and the disparity in NCD mortality rates between the UK and other EU15+ countries has widened over the past 40 years such that by 2008 it was in the highest quartile.1 Among NCD deaths, cancer mortality in the UK is slightly higher than EU15+ countries,1 supporting other evidence that survival from some cancers may be lower than in Northern European countries, and possibly that some tumours are at a later stage by the time children are diagnosed.17 Furthermore the UK has higher mortality rates from neuropsychiatric causes, endocrine, respiratory and digestive disorders, although injury mortality rates have fallen less in the UK than other countries.1 While suicide rates in the UK have dropped since the late 1990s, they are still high compared with some other European countries, and intentional injury deaths account for over a third of all injury-related deaths.13 Mortality from communicable diseases is now extremely low in all wealthy countries, and here the UK is similar to the EU15+ median.1
What might be the reasons for excess child and adolescent mortality in the UK?
The UK and other European countries share many common challenges in child health, but are adapting their health systems to meet those challenges in different ways. Comparing and contrasting different European approaches to Government priority-setting, health systems and organisation, and healthcare and public health, provides useful insights that help shape policy recommendations to improve UK child health.18
Poverty, and social and economic inequities shape the chances of child survival
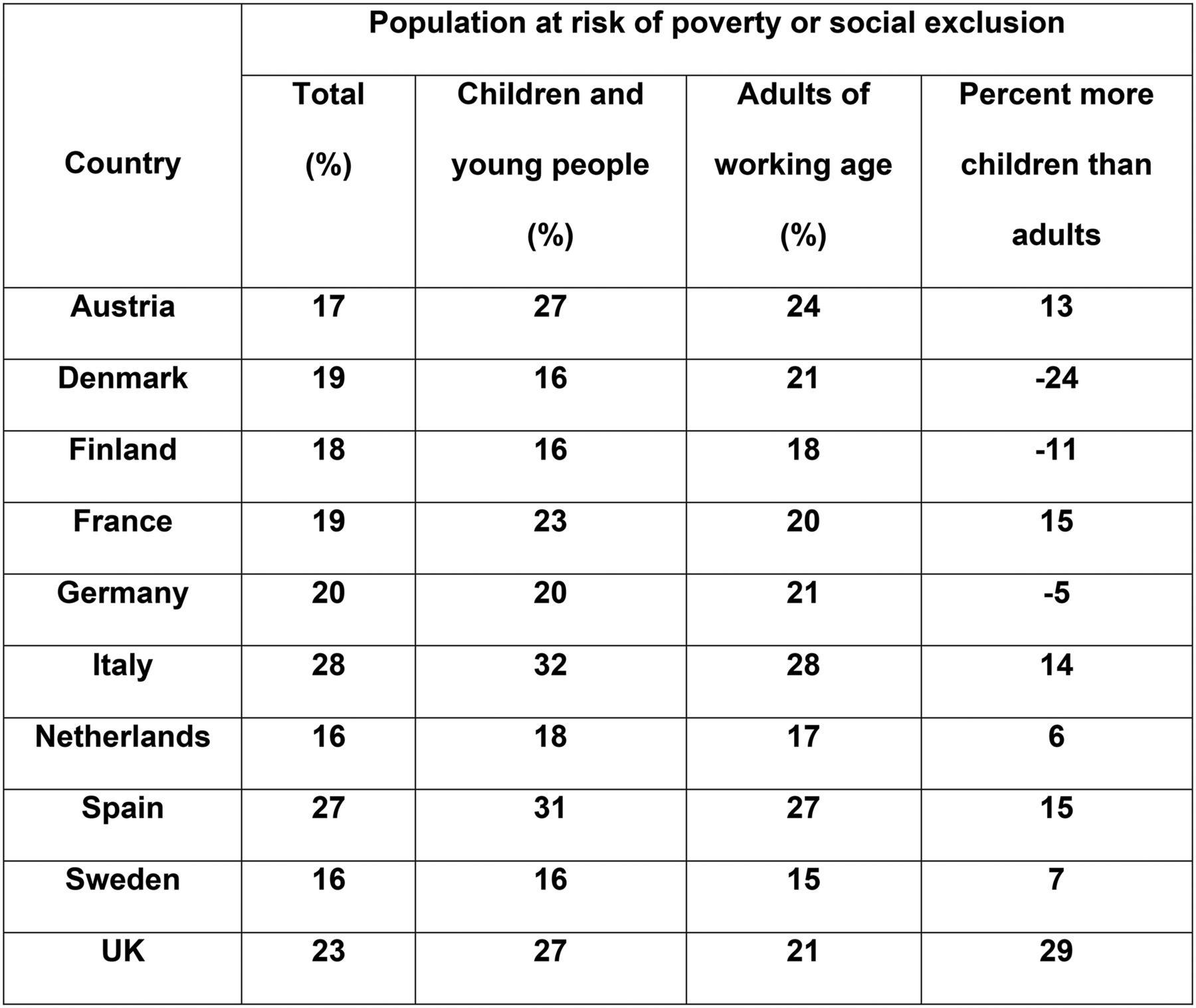
Children who live in poverty and deprivation are less likely to survive than their richer peers. This is true in the UK, as it is elsewhere in Europe. A social gradient for survival affects infants and adolescents,19 and continues through the life course. The distribution of wealth within a country matters too. Children who live in countries with wide gaps between rich and poor people are more likely to die than their peers living in countries where wealth is more equitably shared. It is notable that infant mortality in the UK slowed less rapidly from around 1990 onwards, coincident with rising income inequality in the UK. Absolute child poverty is an increasing problem in the UK,20 35% of households with children do not have an income that is high enough to ensure an acceptable standard of living,21 and the UK remains in the upper range of income inequality among European countries.22 Pressures on families are increasing throughout Europe, and are likely to be exacerbated by ongoing economic problems and reduced public service funding. Among families receiving services, there are increasing rates of alcohol and substance addictions, mental ill health, relationship difficulties, challenging behaviour in children, intimate partner violence and parent-child conflict.23 ,24 The UK is notable because poverty and deprivation disproportionately affect children and young people compared with other age groups.25 As shown in figure 3, this is in distinction to many other European countries, where poverty and social exclusion are more fairly shared between age groups. By contrast, in Britain, recent social spending cuts disproportionately affect families with children. A third of British households have children, but those families bear two-thirds of the burden of recent benefit cuts.26 Food poverty and hunger are growing problems in the UK, with increasing numbers of families reliant on food banks.27
{kind=link}
{kind=link}
{kind=link}
UNICEF. ‘The Children Left Behind: A league table of inequality in child well-being in the world's rich countries’, Innocenti Report Card 9, Florence. UNICEF Innocenti Research Centre, 2010.
How do poverty and inequity kill? Babies born in poverty are more likely to be stillborn or die in infancy.12 ,15 Babies who are born too early or who have low birth weights are at higher risk for infant death, and there is also a link to other risk factors such as age at motherhood. Babies with mothers aged under 20 years or in their 40s have higher rates of infant death than those with mothers aged between 20 years and 34 years. In the UK, over 5% of mothers of babies born in 2010 were under 20 years old, whereas in Sweden, 1.6% of mothers were under 20 years.12 Adverse health behaviours that are linked to low birth weight and preterm birth, such as poor antenatal care, substance abuse, poor nutrition in pregnancy and smoking, are more common in less advantaged socioeconomic groups.28–30 Smoking in pregnancy, for example, is associated with a 20–30% higher likelihood of stillbirth, a 40% higher rate of infant mortality and a 200% higher incidence of sudden infant death syndrome.31 Low birthweight rates are higher among teenage mothers, possibly because of competition for nutrients between the fetus and its mother who is also growing and developing.32 Breastfeeding, which can protect babies from infection and help prevent sudden infant death syndrome, is less common in more disadvantaged socioeconomic groups.33 Adolescents and young people who grow up in disadvantageous conditions face higher risks of external injury, and are more likely to engage in excessive alcohol intake and other risk behaviours.34 Finally, there is evidence to suggest epigenetic effects of early disadvantage may add cumulative risk throughout the life course and may be transmitted to subsequent generations.35
Deaths that are preventable through health systems policy and healthcare practice
The concept of avoidable deaths in childhood provokes controversy and challenge. How would we go about defining what proportion of childhood deaths ought to be preventable? Sweden currently has the lowest child mortality rate in Europe. Excess deaths indicate the scale of difference between countries’ mortality rates, in a way that is meaningful to public and politicians. The UK has just under 2000 more deaths among children under 14 years old than it would do if it had the same mortality rate as in Sweden.2 But is Sweden's mortality rate as low as is realistically achievable in the current state of social advancement and medical progress? Crucially, is there any reason why the UK could not achieve at least the same mortality rate as Sweden?
The proportions of the UK's excess child and adolescent death rates attributable to social determinants, health system factors or healthcare are not clear. Since most deaths happen in the 1st year of life, when there is a strong association between social disadvantage and risk of death, it has been argued that social determinants explain most of the excess mortality in the UK, while micro-level healthcare-related causes provide an overly simplistic explanation for lay media seeking to explain country differences. How much does healthcare contribute to population-level child health? Attempts have been made to estimate the proportion of adult deaths that are healthcare-amenable or avoidable, with answers ranging from 20% to 40%,36 but no estimates appear to have been published for children. It is widely accepted that medicine probably contributed rather little to health gain before the middle of the 20th century, but paediatrics has advanced considerably since then, increasingly technically able to intervene more effectively and in many more diseases and problems than ever before. While it is likely that the marginal contribution of healthcare to health has increased, social determinants of health and health system factors remain vitally important.
Although mortality rates are crude measures of healthcare quality for children and therefore of limited use on their own as quality indicators, assessing signals of concern around quality of care can help point to areas deserving further enquiry and efforts towards improvement. Approximately one in five deaths among children and young people is considered preventable through policy and practice changes in health services and the wider health system,37 though the lessons from statutory reviews of childhood deaths have yet to be translated comprehensively into effective policies.38 There are no reliable comparable figures for European countries, so we cannot answer with precision the question why children are more likely to die in the UK than in some other European countries. Indeed there are no overall measures of quality of healthcare for children. In addition, between-country comparisons are fraught with difficulties relating to definition and coding consistency, so rigorous comprehensive comparative assessments are currently unavailable. However we can identify where systems and practices vary notably between countries, and we can also identify deficits in UK practice which are remediable and may therefore improve mortality and morbidity.
In the year ending 31 March 2013, 21% of the 3857 deaths reviewed in the child death reviews published by the Department for Education, were judged to have had modifiable factors which may have contributed to death and which through nationally or locally achievable interventions may reduce the risk of future deaths.37 The highest proportion of deaths with modifiable factors (nearly 30%) were among children aged between 1 month and 1 year old, and between 15 years and 17 years old. A recently published report reviewing deaths from asthma found that a key risk for children and young people was the failure, in primary and secondary care, to recognise risk of adverse outcome, and that in 93% of deaths reviewed, routine care was inadequate.39
What system-level factors are important for ensuring a high functioning children's health service? Health systems comparisons across Europe can give indications where the UK performs well, and where and how improvements could be made. The UK's tax-funded nationalised health service delivers high quality outcomes for the general adult population and overall performs efficiently and well in high-level indicators compared with many similar OECD and European countries.40 However recent health system reforms in England seem to be producing increasing fragmentation of commissioning and provider functions, and accountability for the quality of children's healthcare remains unclear. Sweden followed the UK's example of market-based reforms in the 1980s, however in response to increasing fragmentation of services, later reverted to a more cooperative model. For example, extensive decentralisation was partially reversed with the formation of elected regional health authorities, while county-level taxes for funding a high proportion of health sector costs were intended to enhance system responsiveness.41 Child health professionals are involved in planning children's health services, to help ensure a child-centric model of care. At a micro level, ‘chains of care’ backed by financial incentives were developed specifically to improve integration and encourage cooperation between professionals and providers.42
An important advantage in the UK compared with many other countries, is an equitable and accessible system of universal primary care, since countries with strong primary care systems deliver high quality outcomes.43 However much less is known about exactly how best to organise everyday healthcare in the interests of children and young people. Primary care has an important gatekeeping role in the UK and delivers the majority of healthcare for children, so a strong primary care service, which is essential for children and families, is also crucial for the rest of the health service to function well. It is challenging to ensure optimal balance between expertise and access in primary care for children, and it is crucial to ensure that workforce is appropriately skilled and resourced.44–46 For example, in England GPs make up only 16% of the primary and community care team (67% are nurses, 14% pharmacists and 3% allied health professionals),47 yet there is no mandatory requirement for training in child health across the primary care workforce, and in contrast to much of the rest of Europe, paediatricians do not routinely work alongside general practitioner (GP) colleagues in primary care settings. Furthermore, integrated care, variously defined as a means of ensuring strong cooperation between providers and sectors, is held as an important mechanism for services to become more responsive to evolving health needs. Shifting care away from a hospital-centric model towards a strong community-based primary care service that can effectively prevent illness and manage children and young people with chronic conditions, as well as acute minor illness, has become a policy imperative.48 Countries with strong primary care systems which also enable close cooperation between health professionals seem to be making progress in delivering high quality care.2 ,18 There are several factors which facilitate such cooperation, including financial incentives for team working and co-location, for example in the Netherlands and Sweden. Workforce numbers, training and teamworking are also important; Sweden has more doctors per child than the UK, and GPs in Sweden are required to be trained specifically in paediatrics and work in teams with children's nurses and doctors.49
Notable differences between country approaches to strengthening important determinants of health, risk factors for death, and health systems policy and practice helps provide a rational approach to making recommendations for reducing child mortality in the UK to bring rates closer to European levels.
What can be done to strengthen conditions for children in Britain to survive and thrive?
Three related findings help us shape policy recommendations to improve the life chances of British children: first, more children die in infancy and adolescence than the middle childhood years, so policies that address the main causes of death in these age groups should have the greatest impact on child mortality. Second, wealthy children who live in socially advantageous circumstances have a greater chance of survival than those in poor families who live with social disadvantage; furthermore greater harm is done to children when there is a wide gap between rich and poor. Macroeconomic and social policies are therefore matters of life and death for children and young people. Third, many deaths in childhood are preventable through changes in health systems policy, public health and healthcare practice, so improvements are needed at the individual and population levels.
Government and civil society
From before birth, social determinants such as poverty and inequity and the policies that reinforce or mitigate their effects, influence children's health, development, happiness and future economic prosperity.50
Approximately a quarter of all infant deaths in England and Wales would potentially be prevented if all babies were born in circumstances as favourable as the least deprived families.51 Supportive family policy can help protect children from the damaging effects of poverty and inequality. Countries that spend more on social protection for families have lower child mortality rates.2 Child survival in Britain would be improved through macroeconomic policies to redistribute wealth and narrow the gap between rich and poor people. Social policies that protect children and families would also help ensure that children survive and thrive. More downstream policies designed to improve social determinants of health are sometimes translated into policies to modify health behaviours. These interventions need to go beyond providing information on healthy choices, since social disadvantage is often linked with poor self-esteem, lack of personal agency and poor mental health. Improving negative health behaviours such as smoking and alcohol consumption requires a nuanced and evidenced approach to health policy. Making healthy choices the easy ones to make means implementing policies such as financial subsidies on fruit and vegetables and taxes on less healthy foods, plain packaging of tobacco, and minimum price per unit of alcohol.52 Finally, policies to improve social determinants must be targeted proportionately across the social gradient to reduce health inequalities.53
Health systems, public health and healthcare
Health system stewardship, financing and organisation are important for ensuring accessible high quality and responsive care for children and young people. Primary care and the structures and processes that foster integration—horizontally (between health, education and social care) and vertically (between primary and secondary care), are important aspects of health systems that affect children. Information systems that enable coherent health service planning, and foster cooperation between institutions and individuals, are equally critical to the delivery of high quality care.
While the explanation for country differences is not yet clear, there are measures that would be likely to improve the quality of care for children and young people in the UK. A renewed focus on primary care, delivered by a team of professionals that achieves an optimal balance between access and expertise for physical and mental health, social care and other specialties, should enable the majority of children's urgent and scheduled health needs to be managed in community settings.18 Such a comprehensive strong model of care, backed by wider policy actions to reduce risk and enhance resilience and quality of life, would help improve prevention and care of long-term conditions in children and young people.
Public health policies and services delivered at population or individual levels are important means of preventing deaths in the longer term. Public health interventions that directly or indirectly reduce risk factors and causes of child mortality include interventions to reduce or prevent smoking, alcohol consumption, and non-intentional and maltreatment-related injuries.
Smoking habits often begin in adolescence, yet there are effective policies for tobacco control that could usefully supplement existing policies. Although the UK scores highly on implementation of tobacco control policies compared with some other countries,54 specifically for children and young people, and women who are planning or expecting a baby, there are further actions that could be taken. Legislation for standardised packaging of tobacco has now been introduced, and this should be welcomed.55 Alcohol consumption among young people in the UK is a considerable public health concern, with signs of alcohol-related liver disease affecting people at increasingly younger adult ages.56 ,57 There is good evidence that minimum pricing of alcohol is effective at reducing consumption, and there are further alcohol-related harm reduction strategies that can be implemented.54 ,58 There are effective policies to prevent most common causes of death from injuries, however legislation, policy implementation and enforcement are crucial.59 Given the lack of progress in reducing violence-related deaths and injuries among children and young people, an effective policy response is needed urgently. The England and Wales Children Act 1989 (section 17)60 places a duty on local authorities to provide services to children in need of additional services beyond universally available care. The intention is to ensure children achieve a reasonable standard of well-being or that their health or development is not significantly impaired. However increasing demand and reduced funding puts pressure on social workers, which can result in rapid turnover of staff, such that there is a risk that professionals working in social work and safeguarding roles are inexperienced or inadequately supported. Legislation in most European countries has been reviewed in light of the United Nations (UN) Convention on the Rights of the Child61 and although there are many common features in country approaches to services, for example an emphasis on working collaboratively with parents and families, encouraging self-referral and providing readily available social work services in local settings such as Sure Start Children's Centres (though many have now closed62), there are many interesting differences. Despite the team around the child (or family) approach that is commonly recommended, the extent of interagency working between social and mental health services and youth criminal justice services, varies between countries.63 In England, youth justice services are separate, unlike in Scotland or Sweden, for example. Another interesting difference in many European countries such as France and Italy, is the social pedagogue, a qualified professional who works alongside children and parents, usually more highly trained than UK family support workers.63 Finally, in some countries, for example France and Italy, child psychiatrists and clinical psychologists play an important role as lead professionals for vulnerable children and young people.63
A population-based approach to planning, delivering and evaluating children's health and social care is wholly dependent on measures of health and social care need and system performance. The Nordic countries’ system of national data registries strongly supports the ability to deliver health and care services tailored to need. Universal data collection and widespread data sharing is a point of national pride and enables health service improvements and research that are important elements contributing to their leading position in many of the European league tables of health system performance. In the UK, data sharing is developing well in Scotland and Wales. Major problems have developed in England, however data sharing may be more complex in England because of the plurality of providers of healthcare who compete with each other for business, and difficulties with data linkage systems.
Recommendations to improve child survival in the UK
The UK could, in theory, achieve the same mortality rate as European countries where children have a greater chance of surviving. Although there is no single cause for the disparities between the UK and other countries and no simple solutions, it is possible to make reasoned policy and practice recommendations. The messages are stark and crucial. Poverty and inequity kill children. Social protection is life-saving medicine for the population. Health systems and services, and public health interventions that save children's lives must be financed, implemented and incentivised appropriately, and sustained.
Policy recommendations to reduce child mortality in the UK were published accompanying our Why Children Die report.3 The recommendations were targeted specifically for the policy environments of the devolved UK nations, and include measures directed at Government and civil society, health systems and organisations, and public health and healthcare policy-makers and providers. Four key themes underpin the recommendations: first, addressing common causes of deaths or substantial contributors to the mortality burden; second, diseases or conditions where significant deficiencies in care have been identified and for which there are identifiable and achievable solutions; third, systems and organisation issues that seem to be important when comparing the UK with other European countries; and finally, societal and policy issues that make a difference to children's survival.
Recognising the understandable emphasis and investment in health policy initiatives to address the needs of an aging population, a collaborative approach from across the children's health sector is needed to advocate effectively for measures to improve the wider determinants of child health and quality of healthcare. As yet there is no collective voice for children across the UK with the capacity and breadth of membership to speak with a loud and united voice for child health.
Therefore, our final and unifying recommendation is for a Countdown UK Child and Adolescent Survival initiative. An independent UK Countdown collaboration should be established across disciplines and institutions, providing a bridge between the technical and the political, identifying gaps in knowledge and practice, reporting annually on progress, and proposing new actions to promote child survival. Setting goals, targets and indicators will direct and maintain efforts towards reducing UK child mortality, and help ensure a process of accountability for action. The Collaborative's attentions should encompass a continuum of care from prepregnancy through maternity, birth, postnatal, infancy, childhood and adolescence; and stretch across boundaries in place from home and community to healthcare facilities and non-health sectors. Such a broad approach to the UK child survival Countdown will help ensure optimal efforts towards the twin goals of mortality reduction and maximal gain in health and well-being. Linking our efforts to the global work in forging Sustainable Development Goals for 2030, and learning from the Countdown to 2015 collaboration64 for low and middle income countries towards achieving the Millennium Development Goals, will help secure the best possible chances for success.
It is a grave injustice that children in the UK do not enjoy the highest standards of health and well-being, and the greatest chances to fulfil their individual potential in life. That children in the UK are dying unnecessarily, shames us as a nation. As child health advocates, professionals, policy makers and citizens, we have a duty to act urgently and effectively, since every child has the right to life and the best possible health.
Acknowledgments
Enver Solomon, of the National Children's Bureau; Francine Bates, of the Lullaby Trust, staff of the Royal College of Paediatrics and Child Health; and the British Association for Child and Adolescent Public Health.
References
Footnotes
Contributors IW conceived the paper, IW and RV led the writing and data analyses. All authors contributed to revisions of the manuscript.
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.