Article Text

Abstract
The UK is currently in the midst of a large outbreak of pertussis, with the highest morbidity and mortality occurring in young unimmunised infants. This review considers the potential strategies to optimise control of pertussis in infants, including vaccination of (1) adolescents, (2) close household contacts of newborn infants (cocooning), (3) newborn infants and (4) pregnant women. The paper discusses the evidence base for each of these strategies and considers the rationale for the recent introduction of a temporary vaccination programme for pregnant women in the UK in response to the ongoing outbreak.
- Epidemiology
- Immunisation
Statistics from Altmetric.com
Background and recent epidemiology
High vaccine coverage, the introduction of an accelerated infant schedule, and the inclusion of pertussis in the preschool booster have contributed to a major overall decline in incidence of pertussis between 1998 and 2009.1–3 Despite this, pertussis remains the most common cause of hospitalisation and death in infants from a disease that is potentially preventable through the current UK routine vaccination programme,3 and continues to display 3–4 yearly cyclical peaks in activity. This suggests that while pertussis vaccines are effective in preventing clinically apparent disease, they are less effective in preventing Bordetella pertussis infection and transmission.
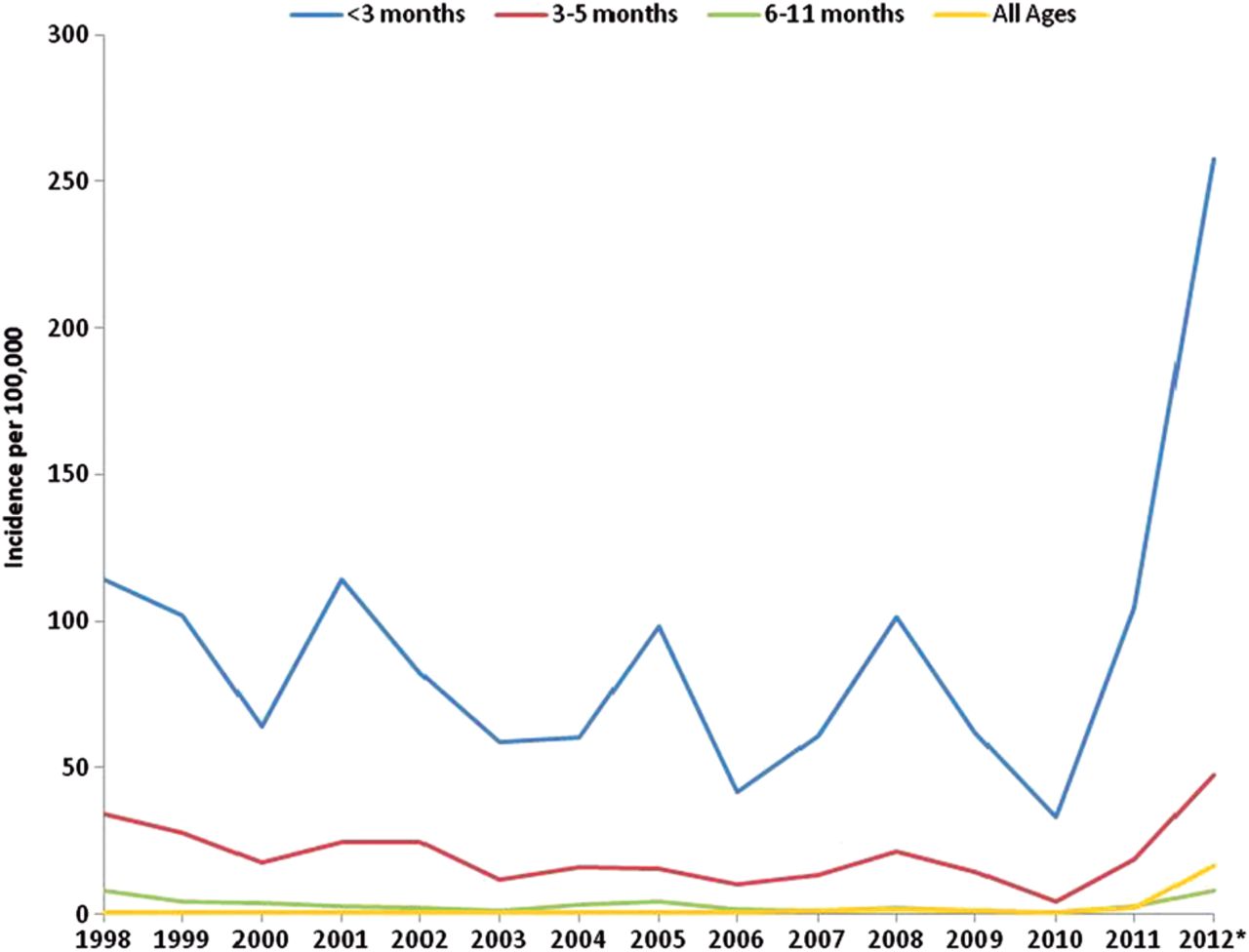
Many countries with longstanding vaccination programmes have experienced recent increases in adolescent and adult disease, attributed to improved case ascertainment and waning immunity following vaccination.4–6 Since mid-2011, the UK has been experiencing a national outbreak of pertussis, predominantly affecting adolescents and adults.7 ,8 Heightened activity continued in 2012 extending to very young infants, who are at highest risk of serious complications and death.8–10 Although the overall incidence remains low compared with the resurgence in the 1970s, the marked rise in incidence among infants less than 3 months of age (258 per 100 000 in 2012 compared with 101 per 100 000 population in the last peak year, 2008) (figure 1) led to the declaration of a national outbreak by the Health Protection Agency in April 2012.11 An urgent review by the Joint Committee on Vaccination and Immunisation (JCVI) culminated in the announcement of a temporary immunisation programme for pregnant women in the UK as an outbreak response.12 This paper considers the potential strategies for optimising pertussis control with the main focus on preventing infant deaths.

Incidence of laboratory-confirmed pertussis, by total case-patients in infants <1 year and all ages in England and Wales, 1998–week 47 2012.
Adolescent pertussis booster
Reported increases in pertussis incidence among adolescent and adult populations have led some countries including the USA, Australia and France to introduce a routine adolescent pertussis booster. In 2010, a WHO review of pertussis control strategies concluded that such boosters do prevent pertussis in adolescents and adults, but that there is insufficient evidence of indirect protection for young infants.13 Since the US recommended the use of Tdap for adolescents in 2006, coverage among 13–17-year-olds has slowly increased from 10.8% in 2006 to 78.2% in 2011.14 Over this time, incidence in adolescents aged 11–18 years has declined, but there has been no discernible impact on infant disease.15 This may be partly attributable to the suboptimal coverage, but also may reflect contact patterns between adolescent and infant populations. Studies of social mixing suggest that adolescents tend to interact primarily with other adolescents, and have less contact with very young infants.16 ,17 Similarly, modelling and cost effectiveness evaluation in the UK in 2001 suggested little impact of an adolescent booster on infant pertussis.2 Recent data from Australia suggested some benefit for infants from a one-off school-based catch-up programme (with a broad age group from 12 to 19 years) followed by a routine programme targeting adolescents aged 12 years.18
Data on the duration of protection from an adolescent pertussis booster are limited, with predicted estimates of between 6 and 10 years.19 Extrapolation from an adolescent trial predicted that the various pertussis antibodies would reach prevaccination rates between 9.5 and 15 years after the dose of dTap.20 Waning immunity following an adolescent booster, has the potential to leave adults of child-bearing age susceptible. A resulting shift in disease to population groups who are a more frequent source of infection to infants,21–23 has led to calls for decennial boosting with pertussis to supplement current dT schedules in some countries.24 In the UK, where adult boosters are not used, modelling the impact of an adolescent booster is required to predict the impact on infant disease in the long term, and this is likely to influence the cost effectiveness of such an approach.
Cocooning strategy
The rationale for a ‘cocooning strategy’ (vaccinating close household contacts of young infants, including postpartum women) is based on evidence that infants often acquire pertussis from a household contact.21–23 A study conducted in Canada, France, Germany and the USA showed that when pertussis occurred in infants, where a source was identified, household members—primarily parents—were the potential source of B. pertussis in 76–83% of cases.22 In a US study of infants with pertussis, in the 43% cases where the source was identified, over 70% had been infected by their mother or other family member, the majority of whom were aged 20 years or more.23 In a UK study of infants admitted to paediatric intensive care with respiratory complications, 20% had laboratory evidence of pertussis and half of these were probably infected from an adult family member.25
For postpartum vaccination of mothers to be effective, by preventing transmission to the infant, mothers should be protected very rapidly after delivery.26 Moreover, where infants have acquired pertussis from their mother, onset of maternal symptoms has been reported to occur before delivery in a fifth of cases.27 Studies of antibody responses to Tdap in postpartum women have shown that Immunoglobulin A and Immunoglobulin G responses to pertussis antigens are not detectable until 5–7 days postvaccination, and the maximum response is not achieved until 14 days after vaccination.28 This leaves a 2-week delay in ‘potential protection’ for the infant during a period of high vulnerability.22
The cocooning strategy has been recommended in some countries including Australia, US and France. The 2010 SAGE review concluded that while such a strategy may help to protect newborns, data on the implementation and impact at a population level were limited.13 The cocooning strategy has been difficult to implement due to the lack of a platform for postpartum administration of vaccines and programmatic issues in administering vaccine to fathers and other adult household contacts.29
Neonatal immunisation
Pertussis immunisation at birth has been proposed following the demonstration of immune responses to pertussis in neonates.30 ,31 However, the lack of a serological correlate of protection poses a significant challenge in determining the clinical efficacy of this approach. An early study using a birth dose of DTaP demonstrated lower pertussis antibody levels after completion of the primary schedule compared with the control group.32 Despite the absence of a licensed monovalent pertussis vaccine for neonatal use, more recent studies using a birth dose of a monovalent acellular pertussis (aP) vaccine showed high levels of antibodies against pertussis antigens during the first 2 months of life with no decline in pertussis antibody levels following completion of the primary schedule. However, two of these studies did demonstrate interference with the responses to Haemophilus influenzae type b and hepatitis B antigens.31 ,33 The exact mechanism for this interference is not known, although bystander T-lymphocyte interference has been proposed as one possibility.34 Further investigation of neonatal immunisation is required.
Improving the timeliness of the primary infant schedule/commencing primary infant course at 6 weeks
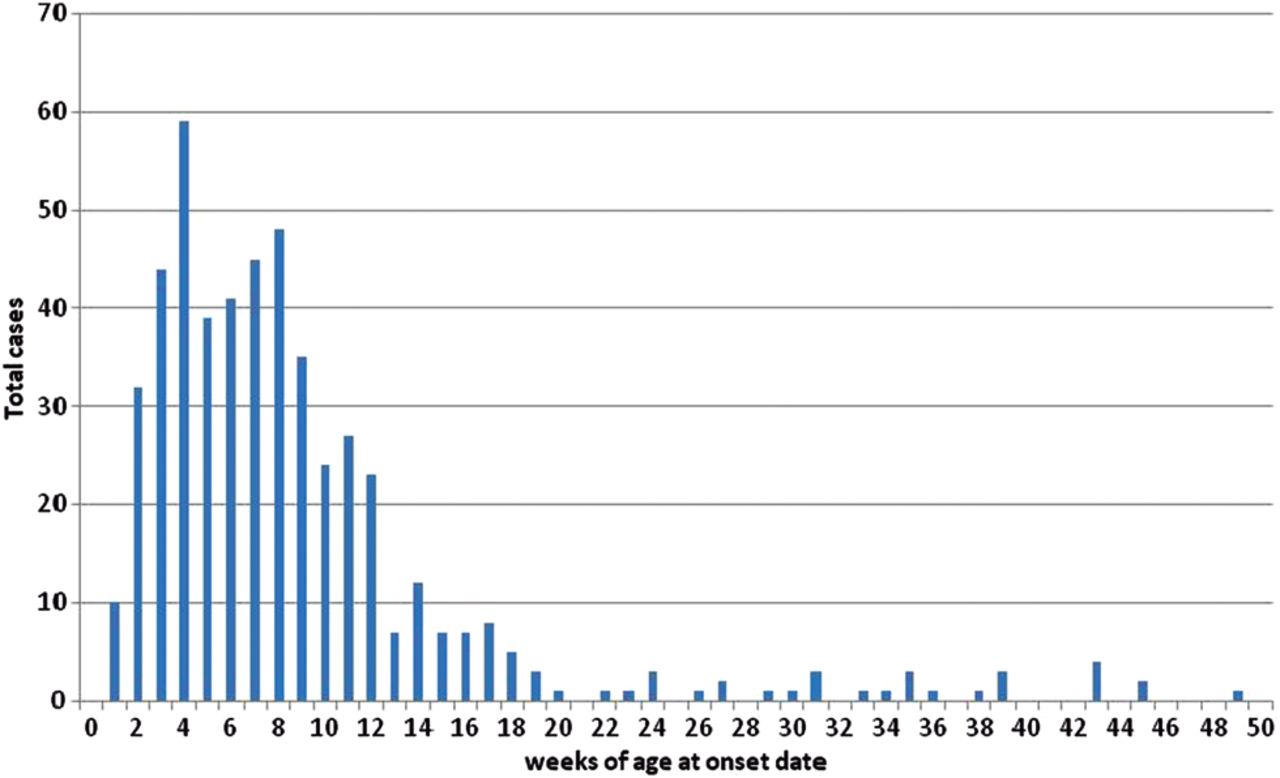
Timely primary infant immunisation is important in protecting infants at the earliest opportunity. Vaccine effectiveness of a single dose of pertussis vaccine in infants less than 6 months of age has been estimated at 61.7% (95% CI 53.4% to 68.6%) in England and Wales.3 Data on the age at which infants born between 1 January 1996 and 1 May 2010 received their first dose of DTaP in England and Wales suggest an improvement in timeliness. Before 2006, almost one-third of infants had not received a single dose of DTaP by 10 weeks age; by 2010, this had declined to less than one-fifth. While timely administration of the infant schedule is important, data on cases of pertussis confirmed during 2012 show that over 60% infant cases occurred by 8 weeks of age, prior to eligibility for routine infant vaccination (figure 2).

{kind=link}
{kind=link}
Distribution of confirmed pertussis cases in the first year of life (England and Wales, 2012 up to week 47).
Scheduling of the first dose of DTaP at 6 weeks of age, as is recommended in many countries as part of the Expanded Programme on Immunisation (EPI) schedule, could potentially afford earlier protection to infants.35 ,36 In an Australian study, the potential benefits of acceleration of the first dose was estimated to reduce notifications, hospitalisations and hospital bed days by 8%, 9% and 12%, respectively, with larger reductions in epidemic years.36 In a US study, acceleration of the first dose was predicted to result in a 9% reduction in cases, 9% reduction in hospitalisations, and 6% reduction in deaths attributable to pertussis among infants <3 months of age.35 If accurate, this would translate to 37 fewer cases of the 409 confirmed cases in infants under 3 months of age in the first 47 weeks of 2012 in England and Wales. Adding to the relatively limited impact, this option requires consideration of the impact, in terms of age-dependent immunogenicity of other vaccines in the primary infant schedule.
Vaccination of pregnant women
Vaccinating women in the third trimester of pregnancy offers the opportunity to provide early protection to infants through increased transplacental transfer of maternal antibodies. A number of studies have provided evidence supporting the existence of efficient transplacental transfer of pertussis antibodies.37 ,38 Cord blood from newborn infants whose mothers received Tdap during or before pregnancy had higher concentrations of pertussis antibodies when compared with cord blood from newborn infants of unvaccinated mothers.37 ,38 Despite the lack of a serological correlate of protection, this option offers the potential of protecting the infant from birth until active immunity is achieved.39 Pertussis-specific secretory IgA has also been demonstrated in breast milk 1–2 weeks after vaccination.40 Additionally, vaccination in pregnancy is likely to prevent maternal infection at the time of delivery and exposure of the infant.
Although there is a theoretical risk for severe local reactions, including Arthus reactions for pregnant women receiving multiple doses of tetanus and diphtheria-containing vaccines at closely spaced intervals, recent data has demonstrated the tolerability of repeated doses of tetanus and diphtheria-containing vaccines in adults with intervals as short as 1 month.41 Furthermore, large studies on the use of inactivated tetanus-toxoid-containing vaccines in pregnant women have not reported clinically significant severe adverse events, and these vaccines have been extensively used in pregnant women worldwide to prevent neonatal tetanus.42 ,43 Although data on the use of acellular pertussis containing vaccines in pregnant women are limited, a review of reports to the Vaccines Adverse Event Reporting System (VAERS) in the USA did not identify any concerning patterns in maternal, infant or fetal outcomes in women receiving Tdap in pregnancy between 2005 and 2010,44 and based on current fertility rates, the majority of women in the UK are likely to require no more than two doses of pertussis vaccine in pregnancy.
In 2011, the USA was the first country to recommend the use of Tdap in pregnant women who previously had not received Tdap in adulthood.45 Based on insufficient antibody persistence from preconception or early pregnancy vaccination, this advice has recently been updated to recommend offering women Tdap in every pregnancy in the third trimester.46 ,47
Some studies have suggested that maternal pertussis antibodies can inhibit pertussis-specific antibody responses of infants vaccinated with DTaP.48 ,49 The lack of correlates of protection means that the clinical relevance of this ‘blunting’ effect is uncertain.50 Interim trial data from a study comparing immune responses in infants born to mothers vaccinated with either Tdap or Td in pregnancy, suggested elevated antipertussis antibody levels at birth and before the first dose of infant vaccines, but lower antibody levels after dose 3 in the first group (unpublished51). The US Advisory Committee on Immunisation Practices (ACIP) concluded that the duration of blunting was short,48 and potential risk of shifting the burden to older infants, where the morbidity and mortality was lower, was outweighed by the potential protection afforded by maternal antibodies.50
Conclusion
The current outbreak in the UK highlights the overwhelming burden of infant pertussis, in terms of morbidity and mortality that occurs prior to the age of routine vaccination. Maternal immunisation provides the only currently available option for protecting infants right from birth and during the period of highest vulnerability and greatest disease burden. As a consequence, the Department of Health, on the advice of JCVI, has introduced a temporary maternal pertussis immunisation programme to minimise morbidity and prevent further infant deaths while the outbreak continues. Evaluation of this programme, including monitoring vaccine coverage, impact on disease incidence and immune response in infants, vaccine effectiveness and safety, which is currently underway, will be critical in informing the long-term strategy for optimising pertussis control in the UK.
Acknowledgments
The author wishes to thank Sonia Ribeiro and Helen Campbell for providing the surveillance data which is included in the paper. The author wishes to thank Dr Mary Ramsay for her input and comments on the manuscript.
References
Footnotes
-
Contributors GA was responsible for the concept and design of the manuscript. GA undertook the literature review and drafted the initial submission and revised the manuscript in light of reviewers’ comments.
-
Competing interests None.
-
Provenance and peer review Commissioned; externally peer reviewed.