Article Text

Abstract
Objective To determine if the sensitivity of the lateral flow test is dependent on the viral load and on the location of swabbing in the respiratory tract in children.
Design Phase 1: Routinely performed reverse transcriptase PCR (RT-PCR) using nose and throat (NT) swabs or endotracheal (ET) aspirates were compared with Innova lateral flow tests (LFTs) using anterior nasal (AN) swabs. Phase 2: RT-PCR-positive children underwent paired AN RT-PCR and LFT and/or paired AN RT-PCR and buccal LFT.
Setting Tertiary paediatric hospitals.
Patients Children under the age of 18 years. Phase 1: undergoing routine testing, phase 2: known SARS-CoV-2 positive.
Results Phase 1: 435 paired swabs taken in 431 asymptomatic patients resulted in 8 positive RT-PCRs, 9 PCR test failures and 418 negative RT-PCRs from NT or ET swabs. The test performance of AN LFT demonstrated sensitivity: 25% (4%–59%), specificity: 100% (99%–100%), positive predictive value (PPV): 100% (18%–100%) and negative predictive value (NPV): 99% (97%–99%).
Phase 2: 14 AN RT-PCR-positive results demonstrated a sensitivity of 77% (50%–92%) of LFTs performed on AN swabs. 15/16 paired buccal LFT swabs were negative.
Conclusion The NPV, PPV and specificity of LFTs are excellent. The sensitivity of LFTs compared with RT-PCR is good when the samples are colocated but may be reduced when the LFT swab is taken from the AN. Buccal swabs are not appropriate for LFT testing. Careful consideration of the swabbing reason, the tolerance of the child and the requirements for test processing (eg, rapidity of results) should be undertaken within hospital settings.
Trial registration number NCT04629157.
- infectious disease medicine
- paediatrics
- epidemiology
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Lateral flow tests (LFTs) for SARS-CoV-2 are a rapid, easily accessible method of testing for SARS-CoV-2 infection, but they are known to have lower sensitivity than reverse transcriptase PCR (RT-PCR) tests when tested on nose and throat specimens.
WHAT THIS STUDY ADDS
This study demonstrates that the specificity, positive and negative predictive values of LFTs performed on anterior nasal swabs are very good compared with nose and throat or endotracheal specimens in asymptomatic children but the sensitivity appears low. The sensitivity of LFTs may improve with specimens both taken from the same location (in this study anterior nares) but buccal swabbing is not an appropriate LFT specimen. This study demonstrates the low prevalence of SARS-CoV-2 in asymptomatic children during the study period.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Testing for SARS-CoV-2 in children continues in community and hospital settings. This study demonstrates the performance of LFTs compared with RT-PCR in different patient populations and using different swabbing locations in children. Consideration of the indication and impact of swabbing a child and the timeliness of results should be weighed when developing policies around SARS-CoV-2 testing in children.
Introduction
The COVID-19 pandemic made swabbing for viral reverse transcriptase PCR (RT-PCR) and lateral flow tests (LFTs) a routine part of life, including for many children. RT-PCR is well-recognised as being the most sensitive test for detecting SARS-CoV-2 with the sensitivity of LFTs appearing to increase with an increased viral load.1 2 RT-PCR testing of asymptomatic children for SARS-CoV-2 remains commonplace hospital practice before aerosol generating procedures (AGPs) and at the time of admission to hospital. In the UK, widespread community testing has ceased, meaning that more children may be attending hospital unaware that they are infected with SARS-CoV-2. The correlation between SARS-CoV-2 antigen positivity and potential transmissibility is believed to be higher than relying on the detection of SARS-CoV-2 RNA which can remain positive for an extended period.3
We have previously demonstrated that anterior nasal swabs are more acceptable to children than nose and throat swabs which are associated with a significantly higher pain score.4 Repeated swabbing procedures are likely to be poorly tolerated by children, particularly those under 5 years of age. This makes it important to understand the impact of the swabbing method on test results. The aim of this study was to determine if the sensitivity of the LFT is dependent on the viral load and on the location of swabbing in the respiratory tract. The viral load, measured on RT-PCR using the cycle threshold (CT) value, was compared with the result of the Innova LFT using swabs taken from the anterior nares and the buccal mucosa.
Methods
This study was performed with approval from the Research Ethics Committee (London City and East: 292509) and Health Research Authority (20/HRA/6152). All children participating in the study had consent to be included either given by themselves or their parents, depending on their age and understanding.
There were four participating centres, all of which were UK specialist paediatric hospitals. Innova LFTs (Innova Medical Group, Monrovia, California, USA) were used for all LFTs reported and tests were performed according to manufacturer’s instructions. RT-PCR tests were performed within the local hospital according to manufacturer and hospital protocols and the CTs were detected using either the Cephid GeneXpert or ABI7500 Fast using Viasure SARS-CoV-2 Real-Time PCR Detection Kit (Pro-Lab Diagnostics, UK) with a positive CT of 44 being used. A CT value of 44 was chosen as within the UK this is the agreed value for reporting a positive result. Each centre had their own protocol for processing the tests. Two centres ran PCR analysis initially without CT value estimation. If the test was presumed positive based on single gene analysis, it was repeated with testing for two SARS-CoV-2 gene loci and with CT analysis. Two centres assessed CT value on all study tests with two gene loci analysis. The lowest CT value of the two tested genes was reported. The laboratory staff were not aware of the LFT results before the RT-PCR test was analysed and brief clinical details were sent with the swab. Recruitment was undertaken between March 2021 and December 2021, and the full study protocol is available in the online supplemental information.
Supplemental material
Phase 1
From January to June 2021, children under 18 years of age undergoing routine nose and throat or endotracheal (ET) aspirate RT-PCR for SARS-CoV-2 were invited to undergo a simultaneous anterior nasal swab for LFT for comparison with the CT value found at PCR. Children undergoing repeated swabbing were eligible to be included for each routine RT-PCR test that was performed during the study period. A 2-week pilot study was undertaken between November and December 2020,4 and the results were used to guide feasibility and perform a power calculation for the study. This indicated that 24 positive swabs were required to answer the primary study question and on the basis of the initial study design and current prevalence that 5400 paired swabs were required to achieve this. High recruitment numbers were required as there was a relatively low prevalence of SARS-CoV-2 in children attending hospital for swabbing, even during peaks of community prevalence; during the 2-week pilot study in two centres, 324 paired swabs were performed and therefore the study design appeared feasible. Recruitment to phase 1 of the study was substantially lower than during the pilot study with fewer patients and families willing to undergo additional tests and therefore the study design was changed.
Phase 2
From July to December 2021, children under 18 years of age with confirmed SARS-CoV-2 on nose and throat RT-PCR were approached and consented to undergo an anterior nasal swab for RT-PCR and an anterior nasal swab or buccal swab or both for LFT within 72 hours of the RT-PCR-positive nose and throat swab.
Statistical analysis
Two-sided Fisher’s exact test was used to compare categorical variables of positive and negative RT-PCR and LFT for phase 1 of the study and are described using relative risk (%, 95% CI). Sensitivity, specificity, positive and negative predictive values are calculated using the Wilson-Brown method. A comparison between the CT value at RT-PCR and the LFT result in phase 2 of the study was performed using logistic regression, and the results are described using ORs (95% CI). Statistical significance was taken as p <0.05. This study is reported according to the STARD guidelines5 used for reporting diagnostic accuracy studies.
Results
A total of 470 paired swabs were performed during the study. Four hundred and thirty-five were performed during phase 1 of the study and 35 during phase 2 of the study.
Phase 1
During phase 1 of the study, 8/435 (2%) had a positive RT-PCR, 9/435 (2%) had a RT-PCR test failure and 2/435 (0.5%) had an initial LFT test failure. The LFT test failures were immediately repeated on a second cassette with the same extraction solution and were successful. The relative risk of (RR) test failure was significantly lower with LFTs than RT-PCR (RR 0.98 (95% CI 0.96 to 0.99), p=0.004). 68/435 (16%) had their RT-PCR sample taken as an ET aspirate, and all results of these tests (RT-PCR and LFT) were negative. 431/435 (99%) swabs were performed on asymptomatic children. The correlation between RT-PCR and LFT test results are shown in table 1.
Matrix of RT-PCR and LFT findings along with calculated sensitivity, specificity, positive and negative predictive values
Phase 2
Twenty-nine of the 35 anterior nasal swabs taken in the second phase of the study were RT-PCR positive. Of children swabbed in the second phase, 43% (15/35) were asymptomatic. Six patients with negative RT-PCR tests also had negative LFT tests.
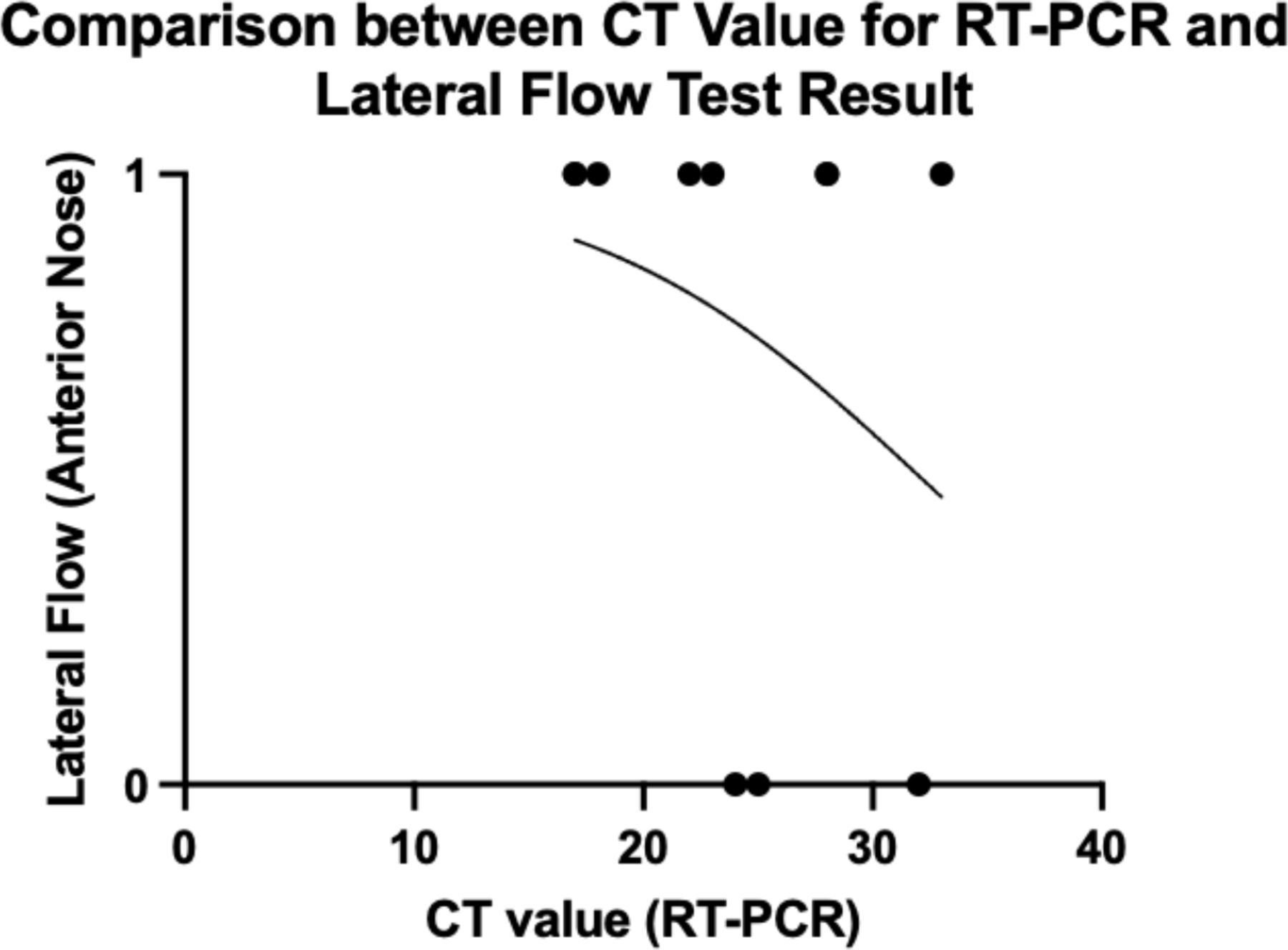
Fourteen paired swabs taken from the anterior nose were compared using RT-PCR and LFT, and one was negative for both. Ten of 13 LFTs were positive, demonstrating an overall sensitivity of 77% (95% CI 50% to 92%). There was no significant correlation demonstrated between CT value (provided in 11 samples) and LFT result (OR 0.87 (95% CI 0.62 to 1.12), p=0.32) (figure 1).

{kind=link}
Comparison between cycle threshold (CT) value for reverse transcriptase PCR (RT-PCR) and the result of lateral flow test (1—positive, 0—negative).
Twenty-one paired swabs compared anterior nasal RT-PCR and buccal LFT, and 16 were RT-PCR positive. Fifteen out of 16 positive RT-PCR swabs were negative on buccal LFT and one was positive.
Discussion
Testing has been a cornerstone of controlling the spread of SARS-CoV-2 globally and remains important in healthcare settings. The use of LFTs for near-patient testing was a novel development resulting from the SARS-CoV-2 pandemic. The speed of introduction and initial paucity of real-world data was a source of significant disagreements in the scientific community as to their role and utility in detection of infection and control of spread of infection. It was in this context that this study was conducted.
Lateral flow testing is recommended for asymptomatic individuals coming into contact with clinically vulnerable people, those who are isolating and those who are working in high-risk environments.6 Furthermore, many children being admitted to hospital and those undergoing an AGP are routinely tested for SARS-CoV-2. The UK Health and Security Agency (UKHSA) recommends that rapid or near-patient testing should be available for risk mitigation of infection prevention and control,7 and the Royal College of Paediatrics and Child Health ‘Recovery of Elective Surgery Guidance’8 has recommended the use of a rapid test, rather than RT-PCR, before an AGP because of the ability to perform it just before the procedure. Despite this guidance, many centres continue to use RT-PCR as the screening test before procedures and at the time of admission to hospital.
This study demonstrates that the Innova LFT test failure rate is much lower than has been previously reported and the false positive rate is very low and consistent with previous studies.9 It also highlights that the negative predictive value of the test is extremally high in asymptomatic children within hospital settings, primarily a reflection of the low prevalence of SARS-CoV-2 in asymptomatic children in this setting. A recent systematic review reviewed the sensitivity and specificity of eight different brands of LFT and demonstrated that the specificity of the majority of these tests is above 96%.2 In-keeping with the findings of phase 2 of this study, the sensitivity of LFTs are shown to be over 70% for the majority of tests studied too.2
This study demonstrates that buccal swabbing for SARS-CoV-2 is not an appropriate means of testing for the virus. The correlation between RT-PCR and LFT when both swabs are taken from the same location appears to be higher than when the PCR is taken from the nose and throat and the LFT from the anterior nares, although this study does not demonstrate this conclusively. However, it is suggestive that swabbing the anterior nares is less sensitive than swabbing the nose and throat. The method of swabbing chosen may depend on the importance of having an absolutely accurate result and on how well the child tolerates the swab.
When contemplating the approach to testing asymptomatic children for SARS-CoV-2 within hospital settings, the reasons for selecting a test should be considered. For adults undergoing surgery, there is evidence that recent infection within the preceding 7 weeks increases the risk of adverse outcomes,10 but the same has not been shown in children.11 As RT-PCR tests continue to detect viral particles for an extended period following acute infection, there may be an advantage of using RT-PCR in preoperative adults to detect recent asymptomatic infection. Children are more likely than adults to have asymptomatic SARS-CoV-2 infection12 but as the risks of adverse outcome after surgery do not appear to be increased in children following asymptomatic SARS-CoV-2 infection, the requirements of the test differ. For children undergoing AGP when they are asymptomatic and SARS-CoV-2 positive, the primary risk is that of transmission to healthcare staff rather than an increased risk of adverse outcome to the child. The requirement of a test is, therefore, to detect those children who are infectious with SARS-CoV-2 prior to undergoing AGP. The viral load of a person infected with SARS-CoV-2 changes substantially during the incubation period of the virus before symptoms start.13 Current UK recommendations highlight that testing should be performed as close to the time of the procedure as possible but it is acceptable to test up to 72 hours before an AGP8 which many continue to enable time for an RT-PCR test to be processed. The advantage of a point-of-care test (POCT) such as LFT is that they can be performed just before a procedure. Modelling performed by UKHSA demonstrates that the risk of performing an AGP on an asymptomatic SARS-CoV-2-positive child is reduced by performing an LFT within 6 hours before the procedure compared with an RT-PCR test performed 36 hours before the procedure.8 The high negative predictive value and specificity of the Innova LFT demonstrated in this study highlights that there would be very low numbers of children requiring to be cancelled ‘on the day’ due to either a true positive or a false positive test.
Strengths and limitations of the study
This study demonstrates the ‘real-life’ applicability of LFTs within a clinical environment. Tests were performed by clinical staff within their routine roles and therefore demonstrates the clinical applicability of the approach to testing. The study is significantly limited by the inability to achieve adequate power to determine a more precise sensitivity of the LFTs compared with PCR. Variability in PCR testing processes (platforms) is likely to also have played a role in the inability to identify a relationship between the LFT result and the CT value at PCR.
Conclusions
The Innova LFT is shown to have a positive and negative predictive value and specificity over 99% compared with RT-PCR. When RT-PCR and LFT are performed on swabs from the same region, the sensitivity is good—approximately 77%. The sensitivity of LFT performed on anterior nares swab compared with nose and throat PCR appears to be reduced, although this study does not demonstrate this conclusively. Careful consideration of the reason for swabbing, the tolerance of the child to swabbing and the requirements for test processing (eg, rapidity of results) should be undertaken within hospital settings.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by 20/HRA/6152City and East NHS REC: 292509 Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The writing team thank Hannah Williams and Thomas Finnie (Emergency Preparedness, Response and Resilience, UK Health Security Agency, Porton Down, UK Joint Modelling Team (JMT); UK Health Security Agency, UK) and Adam Finn (University of Bristol) for their advice when setting up the study.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @RachelHarwood10
Correction notice This article has been corrected since it first published. The open access licence type has been changed to CC BY. 17th May 2023.
Contributors RH, EW, TF, HW, SD, SP, AF, NG and SK conceived and designed the study. RH, LR, CK, ES and MR undertook the delivery of the study, recruiting patients, inputting data and overseeing trial quality in individual centres. RH wrote the manuscript and all authors reviewed, edited and approved the manuscript before submission. RH is the guarantor of this paper.
Funding Test and Trace (Department of Health and Social Care), supplied the lateral flow tests used within the study and funded the study.
Competing interests Public Health England, now UK Health and Security Agency, supplied the lateral flow tests used within the study and contributed £100,000 towards the running of the study.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.